w w w . e l s e v i e r . c o m / l o c a t e / b j i d
The
Brazilian
Journal
of
INFECTIOUS
DISEASES
Review
article
Antifungal
pharmacodynamics:
Latin
America’s
perspective
Javier
M.
Gonzalez
a,b,
Carlos
A.
Rodriguez
b,
Maria
Agudelo
b,c,
Andres
F.
Zuluaga
b,
Omar
Vesga
b,c,∗aClinicaCARDIOVID,Medellín,Colombia
bUniversidaddeAntioquia,FacultaddeMedicina,GrupoInvestigadordeProblemasenEnfermedadesInfecciosas(GRIPE),Medellín,
Colombia
cHospitalUniversitarioSanVicenteFundación,UnidaddeEnfermedadesInfecciosas,Medellín,Colombia
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6May2016 Accepted19September2016 Availableonline5November2016
Keywords:
Antifungalagents Pharmacology Pharmacodynamics Pharmacokinetics Candidiasis Aspergillosis
a
b
s
t
r
a
c
t
The currentincrementofinvasive fungalinfectionsandthe availabilityofnew broad-spectrum antifungal agents has increased the use of these agents by non-expert practitioners,withoutanimpactonmortality.Toimproveefficacywhileminimizing pre-scriptionerrorsandtoreducethehighmonetarycosttothehealthsystems,theprinciples ofpharmacokinetics(PK)andpharmacodynamics(PD)arenecessary.Asystematicreview ofthePDofantifungalsagentswasperformedaimingatthepracticingphysicianwithout expertiseinthisfield.Theinitialsectionofthisreviewfocusesonthegeneralconceptsof antimicrobialPD.Invitrostudies,fungalsusceptibilityandantifungalserumconcentrations arerelatedwithdifferentdosesanddosingschedules,determiningthePDindicesandthe magnituderequiredtoobtainaspecificoutcome.HereinthePDofthemostusedantifungal drugclassesinLatinAmerica(polyenes,azoles,andechinocandins)isdiscussed.
©2016SociedadeBrasileiradeInfectologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
Introduction
Invasivefungalinfections arecurrentlyanimportantcause ofmorbidityandmortality,especiallyinimmunosuppressed patientsandthoseadmittedinintensivecareunits.1,2Candida spp.arethemostfrequentetiologicalagentoffungal infec-tionsinhumans,rankingfourthamongtheetiologicagents ofbloodstreaminfectionsintheUnitedStates,witha mortal-itysimilartosepticshock.InLatinAmerica,ahigherincidence
∗ Correspondingauthor.
E-mailaddress:[email protected](O.Vesga).
ofcandidemiahasbeenreportedcomparedtocountriesofthe northernhemisphere.3Additionally,thediversityofclimates and habitatsin Latin America leads toa higher incidence ofendemic mycoses,including histoplasmosis, paracoccid-ioidomycosis,andcoccidioidomycosis.4
In thelast years,theincidenceofhealthcare-associated fungalinfectionshasbeenrising,mainlyofinvasive candidia-sisandaspergillosis.5Therehasalsobeenanincreasedreport ofnon-albicansCandidainfections,whichdisplayreduced sus-ceptibilitytoantifungaldrugs.6Finally,thenumberofpatients
http://dx.doi.org/10.1016/j.bjid.2016.09.009
withprofound immunosuppressionsecondarytothe treat-mentofhematologicmalignanciesandorgantransplantation isgrowing,and ithasbeenassociatedwiththeincreaseof invasivefungalinfectionsduetoseveralgeneraofmoldsthat representformidablediagnosticandtherapeuticchallenges.7 Despitetheavailabilityofeffectiveantifungaldrugs, mortal-ity dueto fungal infections remains high,8 afact that has promptedthesearch fornewproductsandabetter under-standing ofthe pharmacologyof theseagents to optimize therapy.
ThereareadditionalcomponentsinLatinAmericatothe “host-fungi-drug”triadthatmayalterthepharmacodynamics (PD)withunknownimpactonresistance.Foreconomicand politicalreasons,genericsareextensivelyuseddespitetheir unproven therapeuticequivalence and,in somecases, the treatmentmustbestoppedduetoshortageinsupply. More-over,thepharmacokinetics(PK)/PDknowledgehasnotbeen extensivelyintroducedinthecurriculumofmedicalschools andrelatedclinicalmedicaleducationactivitiesarelimited, mainlybecausePKandPDintegrationsmaybeseenas com-plexandnotpractical.Inconsequence,theadvancementson thePDofantifungalhavenotbeenimplementedasinother regionsoftheworld.
Methods
Aliteraturesearch wasperformedinthePubMed/MEDLINE databaselookingforclinicaltrials,journalarticlesorreviews availableinfull-text,writteninSpanishorEnglishlanguages,
published from January 1962 to July 2015, including the keywords: pharmacodynamics (PD), pharmacokinetics (PK), antifungals,candidiasis,andaspergillosis.Papersabout anti-fungaltherapyco-authoredbytheexpertinthefieldDavidR. Andes,were alsosearched.Outof140papersidentifiedthe authorsselectedtherelevantpapersaboutinvitro,invivo,and clinicalPDofantifungalagents,mainlyemphasizingonthe PK/PDconcepts;tobuildapracticalreviewforgeneral physi-cians,especiallyindevelopingcountries.Thereferencesofthe selectedpaperswerealsousediftheauthorsconsideredthem relevantforthereview.
Review
Generalconceptsofantimicrobialpharmacodynamics
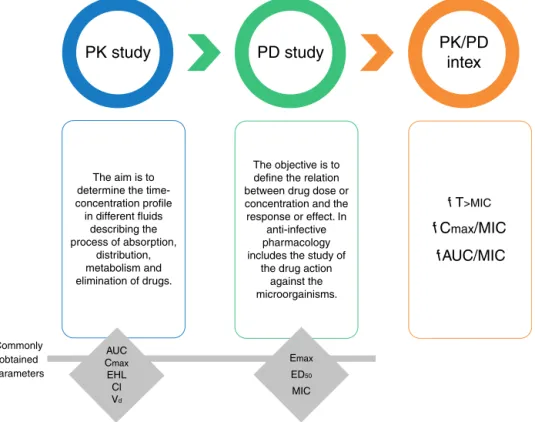
The study of the PK and PD properties of any antimicro-bial isbased on the exposure-response relationshipof the drug andthe infectingpathogen.9 Thisrelationshipcanbe modeled (Fig. 1) byintegrating a PK parameter (e.g., max-imal concentration or Cmax, and area under the curve or AUC)andaPDparameterrelatedwiththeresponseexpected againsttheinfectingmicroorganism(i.e.,minimalinhibitory concentration or MIC). Theknowledge derived from these integrationshasfacilitatedthedesignofoptimaldrug regi-mensandpotentiallyreducetoxicityandthedevelopmentof resistance.10
Classically,PKstudiesareaboutassessingabsorption, dis-tribution,metabolism,andeliminationofdrugs.Theaimof
The aim is to determine the time-concentration profile in different fluids
describing the process of absorption,
distribution, metabolism and elimination of drugs.
The objective is to define the relation between drug dose or concentration and the response or effect. In
anti-infective pharmacology includes the study of
the drug action against the microorgainisms.
f
T
>MICf
C
max/MIC
f
AUC/MIC
AUC Cmax EHL Cl Vd Commonly
obtained parameters
Emax
ED50
MIC
PK study
PD study
PK/PD
intex
PKistodeterminethetime-concentrationdrugprofilein dif-ferentfluidsandthedegreeofpenetrationtodifferentorgans, becausethedrugeffectisexpectedtocorrelatewiththe con-centrationatthesiteoftheinfection.Onceadrugisinsideof thehumanbody,itsmovementbetweencompartmentsand fluidsdependson factors suchas the fractionofunbound drug.Forthisreason,inadditiontothetotaldrug concentra-tion,forPKstudiesitisnecessarytodeterminethedegreeof proteinbindingasonlyunbounddrugexertspharmacological activity.11
PDstudies,ontheotherhand,havetodowiththe rela-tionbetweenthedrugconcentrationatsiteofactionandthe responseoreffect.Inanti-infectivepharmacology,PDstudies integratethesusceptibilityofthemicroorganisms(measured bytheMICs)withtheantimicrobialexposure(basedonthe PKdata)andtheobservedeffectorresponse.Withthis infor-mationitispossibletoestimatePDindices(orPK/PDindex) relatedtoefficacy,as wellas theirlevel necessaryfor spe-cifictherapeuticgoals.Forantifungaldrugs,threePDindices havebeen described: (i) the fractionofthe dosing interval thefreedrugconcentrationisabovetheMIC(fT>MIC);(ii)the ratiooftheareaundertheconcentration-timecurveandthe MIC(fAUC/MIC);and(iii)theratioofthemaximum concen-trationorpeakandtheMIC(fCmax/MIC).Duringthelast15 years,theseindiceshavebeenusedtodesignoptimal anti-fungal dosing regimens with known probability of success alongawiderangeofMICandalsotoestablishsusceptibility breakpoints.12,13
ToelucidatethePK/PDindexforeachantifungal,invitro
and in vivostudies are necessary. Theprocess begins with
in vitro susceptibility testing to determine the MIC under reproducible conditions,14 followed by a PK study to esti-mate the populationparameters (clearance and volume of distribution). Thefinal stepisa dose-responseexperiment torelateexposurewithantimicrobialeffectusingdrug frac-tionation,thatis,testing thesame doseinmultipledosing schedules(e.g. q1h,q3h, q6h, q8h, q12h,and q24h).Atthe end,the threeindicesmentionedbefore(fT>MIC, fCmax/MIC and fAUC/MIC) are plotted against the effect todetermine whichindexexhibitsthe bestcorrelationwithefficacy and toestimate the level required toachieve a particular end-point (for instance, to obtain 50% of maximal efficacy or 90%survival).Thus,fordrugsdrivenbythefCmax/MICindex (concentration-dependent),thedosingstrategyistouselarge doses with infrequent intervals, whereas for fT>MIC drugs (time-dependent)theoptimalregimenwouldbesmallerbut morefrequentdosesorevenextendedorcontinuousinfusion. InthecaseofdrugsdrivenbyfAUC/MIC,thekeyfactoristhe totalamountofdrugadministeredin24h,independentlyof thedosingscheduleused.
AnotherkeyfactortodeterminethePDindicesisthe per-sistenteffect,i.e.,thecapacityofadrugtosuppressthegrowth ofthefungusafterthecompoundisfullyremovedfromthe medium(thepost-antifungaleffectorPAFE),orafterthe con-centrationfallsbelowtheMIC(sub-MICPAFE).15Drugsdriven byfCmax/MICandfAUC/MICexhibitprolongedPAFEwhilstthe
fT>MICdrivenonesusuallydisplayshortornoPAFE.The dura-tionofthePAFEdependsonthetypeofaction(fungicidalor fungistatic),thedrugconcentrationandthepathogenbeing treated.For example,theechinocandinsare fungicidaland
exhibitlongPAFEagainstCandidaspp.,whilefungistaticand devoidofPAFEagainstAspergillusfumigatus.16
The systemic antifungal classes currently available are polyenes, triazoles, echinocandins, and flucytosine. For all of them, the PK/PD indices have been determined both
in vitroand in vivo,17–21 and the resultsconfirmed by clini-calstudies(Table1),demonstratingthatdoseoptimizationto attainPDtargetsleadstohigherclinicalefficacy.22,23Dueto limitedavailabilityofflucytosineindevelopingcountries,the presentreviewwillfocusonthePDofpolyenes,triazoles,and echinocandins.
Polyenes
ThisantifungalclassincludesamphotericinBdeoxycholate (AMBd)andthelipidformulations:lipidcomplex(AMBlc), col-loidaldispersion(AMBcd),andliposomal(AMBl).
The mechanism of action requires its binding to the ergosterol in the fungal membrane, altering the cellular permeability and leading to cell death.All formulations of AMBdisplayaconcentration-dependenteffectwithprolonged PAFE,andthedrivingPK/PDindexisthefCmax/MIC.15,16,19,24
Dose fractionation studies with the neutropenic mouse disseminatedcandidiasis(NMDC)model,confirmedthatthe fungicidalefficacyofAMBdcorrelatedwithlarge,infrequent doses;forinstance,dosingAMBdevery72h(q72h)achieved maximalefficacywithdoses5–7timeslowerthanq6horq12h schedules.19Forfungistaticandmaximallyfungicidaleffects, theCmax/MICwere2–4and10,respectively.Similarly,butin themurinemodelofinvasivepulmonaryaspergillosis,q72h dosingschedulesalsoledtoalargerreductioninthefungal burdenandlongersurvivalofinfectedanimalsincomparison withq8horq24h;inthismodel, theCmax/MICrequiredfor maximalefficacywas2.4.25
IntheNMDCmodel,AMBdwas4.3-to5.9-foldmorepotent than AMBlc and AMBl ina mg/kgbasis.26 Similarly,in the neutropenic-rabbit modelofinvasivepulmonary aspergillo-sis,near-maximalantifungalactivitywasevidentwithAMBd at1mg/kg/dayandAMBlcandAMBlat5mg/kg/day.27Thus,to achievetheneededCmax/MICwithlipidformulationsin clin-icalpractice,thedailydoseshouldbealmost5-timeshigher thanthedoseofAMBd.Inoppositiontothenarrow therapeu-ticindexofAMBd,thelipidformulationsaresignificantlyless toxicinrelationtothedoseofAMBd,specificallyintermsof electrolyticimbalance,azotemia,renaltubularacidosis, ane-mia,andarrhythmias.28
RegardingthePKofpolyenes,theconcentration-time pro-file of amphotericin is nonlinear but there are important differencesbetweenAMBdandlipidformulations.29AMBdis extensivelydistributedtotissuessuchasliver,kidneys,spleen and,insmallquantities(<1%),toheartandbrain,but clear-ance(Cl) from these sitesisso slow(38±15mL/h/kg)as it takesmorethanoneweektoclearasingledose.Additionally, ithasavolumeofdistribution(Vd)of5±3L/kgandtheprotein bindingisveryhigh(>95%).30,31 AMBlevelsincerebrospinal fluidandvitreousarenulltominimal,thereforeintrathecalor intravitrealadministrationisneededinselectedcases.
Table1–SummaryofthePK/PDindicesandtheirrequiredmagnitudeforefficacywithantifungaldrugsand recommendedgoalsfortherapeuticdrugmonitoring(TDM).
Antifungalclass Drug PK/PDindex drivingthe
efficacy
Targettoattain Preferred dose
TDMgoal (trough con-centrationsin
mg/L)[79]
References
Polyenes
AMB deoxycholate
fCmax/MIC
≥10 0.4–1mg/kgIV
q24h
Not
recommended
18,27
AMBlipid complex
≥50 5mg/kgIVq24h Not
recommended 25
AMBliposomal ≥50 3–5mg/kgIV
q24h
Not
recommended 25
AMBcolloidal dispersion
≥50 4mg/kgIVq24h Not
recommended 25
Triazoles
Itraconazole
fAUC/MIC
Notdetermined 200mgPOq24h 0.5–1(measured
duringthefirst 5daysof therapyand regularlyafter)
54
Fluconazole 13–50 400–800mg/day
PO/IVfor systemic infections; 1200–2000mg/day PO/IVfor cryptococcal meningitis. Dosingcanbe scheduledq12h orq24h
Notused. 12,13,39,44
Voriconazole 11–52(candidiasis)
80–100(aspergillosis)
200mgPOq12h 1–5(measured
duringthefirst 5daysof therapyand regularlyafter)
17
Posaconazole 6–27(candidiasis)
20(aspergillosis)
200–600mgPO q24h
>0.7 (prophylaxis) >1(established infection)
16,60
Isavuconazonium sulfate(prodrug)
34 Loadingdose
372mgq8h×6 doses,then 372mgIVq24h
Unknown 45
Echinocandins
Anidulafungin fCmax/MIC
(or
fAUC/MIC)
1(or10–20) Loadingdose
200mgIV,then 100mgIVq24h
Notused 20
Micafungin 1(or7.5–30) 150mgIVq24h Notused 74
Caspofungin 1(or10–20) Loadingdose
70mgIV,then 50mgIVq24h
Notused 69
molecules,itdisplaysthehighestVd(131±8L/kg)andfastest Cl(426±189mL/h/kg)ofallformulations.Incontrast,AMBl has the lowest Vd (0.11±0.08L/kg) and Cl (11±6mL/h/kg) amongamphotericinformulations,whileAMBcdhasasimilar
Vdbutfasterclearance(117mL/h/kg)thanAMBd.Additionally, aslipidformsaccumulatemoreinthemononuclear phago-cyticsystemand10-timeslessinthekidneys,theyareless frequentlyassociatedwithnephrotoxicitythanAMBd.33
Amongthelipidformulations,AMBlisthesmallest, uni-lamellarmolecule(60–70nm vs.1600–11,000nm forAMBlc), achievingthehighestCmax(83±35mg/L)afterasingledose,34 butalsodisplayingthehighestproteinbinding.However,the
smallsizeofAMBlfacilitatesslightlyhigherconcentrationsin centralnervoussystemcomparedtootherlipidformulations. Infact,inthecentralnervoussystemmodelofcandidiasis, onlyAMBlandAMBdsterilizedthebraintissue,whereasthe otherlipidformulationsdidnot,34andonlyAMB
dandAMBl reacheddetectablecerebrospinalfluidconcentrations,witha transferraterangingfrom0.02%to0.92%.35
generallyadvocatedforAMBandtherearenowidelyaccepted drugexposuretargets.However,theoptimaltargetattainment hasbeendefinedforAMBdaswellasAMBl.APK/PDstudyin ninechildrenwithfungalinfectiontreatedwithAMBlfound that,whileaCmax/MIC=40±13producedapartialresponse, fullresponseneededittobe67.9±17(p=0.021).36Considering thatAMBdisapproximately5×morepotentthanAMBl,these resultsareconsistentwiththereportedvalueofCmax/MICof 10formaximalefficacyofAMBd.
Cornelly et al. conducted a multicenter randomized double-blindstudyinpatientswithprobableordemonstrated moldinvasiveinfections.Theirstudyaimedtooptimizethe
Cmax/MICwithAMBlcomparinga3mg/kgvs.a10mg/kgdose basedonapreviousworkthatshowedthatthelatterreaches
Cmax>100mg/L.Nosignificantdifferenceswerefoundinthe globalclinicalresponse(50%vs.46%)orsurvivalafter12weeks (71%vs.58%),buttherewasahigherincidenceofrenaltoxicity (16%vs.30%).37Theabsenceofclinicalbenefitofthehigher dosecanbeexplainedbythefactthatat3mg/kgthegoalofthe PK/PDindexrequiredformaximalefficacyhasalreadybeen reached,andhigherdosesonlyleadtoincreasedtoxicity.30 Finally, a999-patient simulation basedinthe neutropenic-rabbitmodelofinvasivepulmonaryaspergillosisshowedthat 3mg/kg/dayofAMBlor1mg/kg/dayofAMBdwaspredictedto resultinnear-maximalantifungalactivityandsuppressionof biomarkers.27TheoptimaldoseofAMB
lcandAMBcdhasnot beenasclearlyestablishedastheAMBdandAMBl.
Triazoles
Thesefungistatic drugsactblocking the synthesisof ergo-sterolmainly byinhibiting the cytochrome P450 dependent 14-␣demethylase(CYP51A1),whichconvertslanosterolinto ergosterol.38,39Thesedrugsareactuallytime-dependent,but theyalsoexhibitprolongedPAFE,thereforethePDindex driv-ingefficacyisthefAUC/MIC.13,15,17,18,24,40
Fluconazoleabsorptionfrom thegastrointestinaltract is almostcompleteandunaffectedbygastricacidityorfood,is poorlymetabolized,andbioavailabilityisnear100%.Its elim-inationhalf-liferanges from25to30h,itexhibitsminimal proteinbinding(12%),andisexcretedmainlybythekidneys. The Cmax obtained aftera 100mgoral dose was 2mg/L.41 Asfluconazoleisa smallmolecule (MW=309) actively dis-tributedintobodyfluids(Vd=46±8L),thelevelsattainedin cerebrospinalfluid(oreveninbrainparenchyma)atsteady stateare≥50%oftheconcentrationobservedinplasma.Due tothisPKproperty,fluconazoleisawell-acceptedalternative therapyforcryptococcal(athighdosesof1200–2000mg/day) andCandidameningoencephalitis.Itraconazole,bycontrast,is alargemolecule(MW=705)highlyboundtoproteins, exhibit-ingacerebrospinalfluid/plasmaconcentrationratioof≤0.1242 thatpreventitsuseinfungalCNSinfections.
Regarding fluconazole, Louieet al. demonstrated inthe murinemodelofsystemiccandidiasisthattheeffectofthis drugonthefungal burdenwasthesamewhen administer-ing asingledose or dividingit intwo or four injections.40 However,itshouldbenotedthatprolongedperiodsof expo-sure below the MIC might favor resistance of C. albicans
againstfluconazole.43,44Multiplestudiesinvivowith flucona-zole against several species of Candida along a wide MIC
rangehaveconclusivelyshownthatthefAUC/MICnecessary toreach50%ofthemaximalefficacy(ED50)isbetween12.5and 50.12,13,40WedeterminedintheNMDCmodelthattwovastly differentstrainsofC.albicans(MIC0.25and4mg/L)required
fAUC/MICof25–38toattaintheED50.45
Therelationshipbetweenfluconazoledose,theMICofthe infectingagent,andthe outcomeinpatientswith mucocu-taneouscandidiasisandcandidemiahasbeenaddressedin severalpapers.12,22,23Rexetal.publishedtwodecadesagothat theclinicalefficacyoffluconazolebegantodiminishwithMIC above8mg/L,buttheydidnotrunaPK/PDanalysis.22Later, Rodriguez-Tudelaetal.studied126patientswithcandidemia and 110withpharyngeal candidiasisfinding thatdose/MIC ratios ofatleast 100(corresponding to fAUC/MIC=79) pre-dicted curefor93%ofthe subjects.22 In theLatin America Invasive Mycosis Network, the MIC90 for blood-isolated C.
albicans,C.parapsilosis,andC.tropicaliswere≤1mg/L3;asthose threestrainsrepresent82%ofcases,nomorethan400mg/day offluconazoleshouldbenecessarytotreatmostofpatients.
With the other triazoles, similar fAUC/MIC ratios have been foundagainstseveralCandidaspp.17,18,46 Forexample, voriconazoleandposaconazolerequirerespectivelyfAUC/MIC of11–52and6–27toreachtheED50intheNMDCmodel,while isavuconazole(proteinbinding>95%)requiredfAUC/MICof34 toachieve90%survival,quitesimilartoothertriazoles. Phar-macokineticstudiesofvoriconazoleinhumanshaveshown 58% proteinbindingand nonlinear saturablekinetics, with theAUCincreasinginahigherproportionthanthedose.At dosesof200mgPOq12hor3mg/kgIVq12h,thefAUCis20.47 ConsideringthatthetargetforED50 isfAUC/MIC around20 (range11–50),onecouldinferthatclinicalsuccesswouldbe attainedwithstrainswithMICupto1mg/L.Thisagreeswith thesusceptibilitybreakpointdefinedbyCLSI,highlightingthe relevance ofthe PK/PDapproach.48 AllCandidaspecies iso-lated inthe LatinAmerica InvasiveMycosisNetworkhada MIC≤0.5mg/L.
The pharmacodynamics of voriconazole has also been studiedinthedisseminatedaspergillosismodel(inducedby intravenous inoculation).49 The fAUC/MIC requiredfor 50% survival(ED50)wasaround12,whilefor100%survival(Emax) it went up to80–100. Regarding posaconazole,Lepaket al. assessed its pharmacodynamics againstAspergillus spp. in thepulmonaryinvasiveaspergillosismodel(inducedbynasal instillation),50findingthatthefAUC/MICnecessarytoachieve the ED50was 1.8,butatleast10wasrequiredtoreach the
Emax. Howardet al. published similar results,51 and Conte etal.foundinastudyofpulmonarytransplantpatients52that posaconazoleconcentrationwas50timeshigherinalveolar cellsthaninserumorepithelialliningfluid.Theseresults sug-gestthatthePK/PDprofileofposaconazoleisfavorableforthe treatmentofpulmonaryaspergillosis.
onthesedata,arandomizedclinicalstudywascarriedoutto assesstheimpactofTDMofvoriconazolein110patientswith invasivefungal infections. Thetrialshowed that TDMwas associatedwithhigherefficacy(81%vs.57%,p=0.04)andlower drugdiscontinuationduetotoxicity(4% vs.17%,p=0.02).54 These results supportthe recent recommendations bythe BritishSocietyforMedicalMycologyindicatingTDMforall patientsreceivingvoriconazole.Thegoal istoreachtrough levels(Cmin)between1and 4–6mg/Lor,ideally, aCmin/MIC ratioof2–5.55
Posaconazoleischaracterizedbyalonghalf-life (approxi-mately30h),saturableabsorptionat800mg/day,highprotein binding(98%),andalongtimetoreachsteadystate concen-trations(10days).56Itisusuallyadministeredasasuspension twiceaday, sothe concentration-timecurve isalmost flat withverysimilarpeaksandtroughs.Among67patientswith refractoryinvasiveaspergillosis thatreceived posaconazole and underwent TDM, it was found that those with peak (Cmax)andaverageconcentrations(Cavg)of0.14and0.13mg/L, respectively,onlyhad24%response.Incontrast,inpatients withCmax andCavg of1.48 and1.25mg/L,75%hada favor-ableresponse.57Theseresultssupporttherecommendation oftroughlevels>1mg/Lforpatientswithestablished infec-tionsand0.7mg/Lforprophylaxis.55ThePKofposaconazole alsoexhibitshighbetween-subjectvariabilityinpatientswith hematologicmalignancies,58anotherreasonforTDM.Tothe best ofour knowledge, thereare noclinical studies corre-latingthefAUC/MIC ofposaconazolewithclinicaloutcome, but considering that 800mg per day yields fAUC around 0.30–0.44,52,59 afAUC/MICnear3canbeattainedwithMICs upto0.125mg/L,theEUCASTsusceptibilitybreakpointforA. fumigatus.60Toimprovebioavailabilityandreduce between-subjectvariability inpatients, adelayed-release(DR) tablet formulationwasdeveloped.Atadoseof300mgonceaday (three100mgDRtablets),90%ofpatientsachieved posacona-zoleserumconcentrationsgreaterthan700ng/mL,compared with58% patientsreceiving theoralsuspension. Acid sup-pressiondidnotaffectposaconazolelevelsintheDRtablet cohort.61
Echinocandins
Thesearelargelipoproteinswithnegligibleoral bioavailabil-ity,extensiveproteinbinding(>95%),lackofrenalclearance, andnopenetrationtocerebrospinalfluid.Theirunique mech-anismof action(inhibition of1,3--glucan synthase), high
in vivoefficacy,and safety profile,has increasedits use as treatmentforinvasivecandidiasisandaspergillosis.Thethree approvedagentsarecaspofungin,anidulafungin, and mica-fungin.
Beingthenewergroupofantifungals,echinocandinshave been studied thoroughlyfrom a PK/PDperspective.62 They are fungicidal against Candidaspp. and fungistatic against
Aspergillusspp.ThePDindexthatbestdrivetheiractionis thefCmax/MIC,displayingprolongedPAFE.21,63–65However,in theNMDCmodel,thefAUC/MICratioisalsoastrongpredictor ofefficacy,presumablyduetotheprolongedtissue distribu-tion ofthesecompoundsincluding the kidneys,wherethe antifungaleffectismeasured inthis model. Dose fraction-ationstudies haveshownthat thedose requiredtoreduce
thefungalburdenby1log10 is4-foldlowerwhenthedrugs areadministeredoncedaily.21,62Ofnote,aparadoxicaleffect consistinginareducedfungicidalefficacyagainstCandidaspp. hasbeenobservedinvitroatconcentrationsabovetheMIC.66 Sucheffectresultsofcompensatoryresponsesto1,3--glucan synthesisanddisappearswhenhumanserumisadded, indi-catingthatitisnotlikelytoimpactthetreatmentofpatients withcandidemia.67
ThemagnitudeofPDindicesbound tomaximal efficacy in animalmodels ofinvasivecandidiasis isafCmax/MICof 1 or a fAUC/MIC between 10 and 20 for anidulafungin,21 micafungin,62 and caspofungin.Considering thatthe usual dose of anidulafungin (200mg loading dose followed by 100mg q24h) is associated with fCmax=1.15mg/L and
fAUC=1.12mghL−1,68thePDtargetwillbeattainedagainst strains withMIC≤0.125mg/L. Recentepidemiological stud-ies indicate that the MIC90 ofanidulafungin is<0.125mg/L formanyCandidaspeciesexceptingC.parapsilosis,C. guillier-mondii,C.lusitaniaeandC.famata.69AninvivoPDstudyfound thatthefAUC/MICtobefungistaticagainstC.parapsilosisand
C.glabratawas7,incontrastto20againstC.albicans.70These datasupporttheCLSIsusceptibilitybreakpointof0.25mg/L for C.albicans, C.tropicalis, and C. krusei, and 2mg/L forC. parapsilosis.71
The majority of clinical trials with echinocandins have focusedontheevaluationofclinicalefficacy72,73andits rela-tiontotheMIC.74Regardingmicafungin,aPK/PDanalysisof datafrom 493patientsfoundthat afAUC/MICbetween7.5 and30wasassociatedwith98%microbiologicalsuccess, com-paredto85%whentheindexwas<7.5.75Finally,inpatients withC.parapsilosisinfection,afAUC/MIC>0.71wasrelatedto 100%microbiologicalsuccesscomparedwith82%inpatients withvalues<0.71.ThisisafurtherdemonstrationthatC. para-psilosis requires a10-fold lesser fAUC/MIC, in line with its highersusceptibilitybreakpoint.
Finally,inpediatricpatients,dosingadjustmentis neces-saryformostantifungaldrugstoobtainthesameexposure achieved in adults. Also, differences are known in drug metabolismandclearance,andthemagnitudeofthePK/PD indices requires more studies in that specific population. Fungalinfectionsinchildrencomparedtoadultsmayaffect organsandsystemsdifferently(e.g.CNSinfectionduring can-didemiaisfrequentinchildren).Arecentreviewonpediatric pharmacologyofantifungalagentsisavailable.76
Conclusion
and
future
perspectives
toxicity,amelioratingthedevelopmentofresistanceand cut-tingcosts,ascorroboratedbyclinicaltrials.78Thisknowledge canbeappliedtoeachpatientinanyclinicalsetting(Table1), althoughTDMisnecessarytoassurethatthemagnitudeof the PK/PDindices required formaximal efficacy are effec-tivelyachieved.Thisprocesswould introduceanadditional expenditurerelatedtothequantificationofdrugsin special-izedlaboratories,whichcouldbeoffsetbythemuchgreater economicandsocialbenefitsofoptimizedtherapy.79
Author’s
contribution
JMG made the search of literature, reviewed the papers included,andwrotethefirstdraftofthemanuscript.CAR,MA andAZreviewedtheliterature,madecriticismtothearticle andapprovedthefinalversion.OVreviewedandeditedthe finaltext.
Conflicts
of
interest
Gonzalez, Agudelo and Vesga have no conflicts ofinterest to declare. Rodriguez has received honorary for unrelated lecturesfromRocheandAmgen.Zuluagahasreceived hon-orary for unrelated lectures from Allergan, Amgen, Lilly, Mundipharma,NovoNordisk,Pfizer,RocheandSanofi.None ofthesecompaniesoranyotherpharmaceuticalcompanywas involvedinthedesign,execution,orpublicationofthisstudy.
Acknowledgments
FundingforthisprojectcamefromtheUniversidadde Antio-quia(UdeA)andSistemaGeneralRegalíasofColombia(BPIN: 2013000100183).Thefundershadnoroleinstudydesign,data collectionandanalysis,decisiontopublish,orpreparationof themanuscript.
r
e
f
e
r
e
n
c
e
s
1. AzieN,NeofytosD,PfallerM,Meier-KriescheHU,QuanSP, HornD.ThePATH(ProspectiveAntifungalTherapy) Alliance(R)registryandinvasivefungalinfections:update 2012.DiagnMicrobiolInfectDis.2012;73:293–300.
2. TrickWE,FridkinSK,EdwardsJR,HajjehRA,GaynesRP, NationalNosocomialInfectionsSurveillanceSystemH. Seculartrendofhospital-acquiredcandidemiaamong intensivecareunitpatientsintheUnitedStatesduring 1989–1999.ClinInfectDis.2002;35:627–30.
3. NucciM,Queiroz-TellesF,Alvarado-MatuteT,etal. EpidemiologyofcandidemiainLatinAmerica:a laboratory-basedsurvey.PLOSONE.2013;8:e59373.
4. ColomboAL,TobonA,RestrepoA,Queiroz-TellesF,NucciM. EpidemiologyofendemicsystemicfungalinfectionsinLatin America.MedMycol.2011;49:785–98.
5. AlangadenGJ.Nosocomialfungalinfections:epidemiology, infectioncontrol,andprevention.InfectDisClinNAm. 2011;25:201–25.
6. PfallerMA,AndesDR,DiekemaDJ,etal.Epidemiologyand outcomesofinvasivecandidiasisduetonon-albicansspecies ofCandidain2,496patients:datafromtheProspective
AntifungalTherapy(PATH)registry2004–2008.PLOSONE. 2014;9:e101510.
7.PappasPG,AlexanderBD,AndesDR,etal.Invasivefungal infectionsamongorgantransplantrecipients:resultsofthe Transplant-AssociatedInfectionSurveillanceNetwork (TRANSNET).ClinInfectDis.2010;50:1101–11.
8.KriengkauykiatJ,ItoJI,DadwalSS.Epidemiologyand treatmentapproachesinmanagementofinvasivefungal infections.ClinEpidemiol.2011;3:175–91.
9.CraigWA.Pharmacokinetic/pharmacodynamicparameters: rationaleforantibacterialdosingofmiceandmen.ClinInfect Dis.1998;26:1–10,quiz1-2.
10.DrusanoGL.Pharmacokineticsandpharmacodynamicsof antimicrobials.ClinInfectDis.2007;45Suppl.1:S89–95.
11.CraigWA,KuninCM.Significanceofserumproteinandtissue bindingofantimicrobialagents.AnnuRevMed.
1976;27:287–300.
12.RexJH,PfallerMA,GalgianiJN,etal.Developmentof interpretivebreakpointsforantifungalsusceptibilitytesting: conceptualframeworkandanalysisofinvitro-invivo correlationdataforfluconazole,itraconazole,andcandida infections.SubcommitteeonAntifungalSusceptibility TestingoftheNationalCommitteeforClinicalLaboratory Standards.ClinInfectDis.1997;24:235–47.
13.AndesD,vanOgtropM.Characterizationandquantitationof thepharmacodynamicsoffluconazoleinaneutropenic murinedisseminatedcandidiasisinfectionmodel. AntimicrobAgentsChemother.1999;43:2116–20.
14.CLSI.Referencemethodforbrothdilutionantifungal susceptibilitytestingofyeasts.M27-A3.Wayne,PA:Clinical andLaboratoryStandardInstitute;2008.
15.TurnidgeJD,GudmundssonS,VogelmanB,CraigWA.The postantibioticeffectofantifungalagentsagainstcommon pathogenicyeasts.JAntimicrobChemother.1994;34: 83–92.
16.ManavathuEK,RameshMS,BaskaranI,GanesanLT,
ChandrasekarPH.Acomparativestudyofthepost-antifungal effect(PAFE)ofamphotericinB,triazolesandechinocandins onAspergillusfumigatusandCandidaalbicans.JAntimicrob Chemother.2004;53:386–9.
17.AndesD,MarchilloK,ConklinR,etal.Pharmacodynamicsof anewtriazole,posaconazole,inamurinemodelof
disseminatedcandidiasis.AntimicrobAgentsChemother. 2004;48:137–42.
18.AndesD,MarchilloK,StamstadT,ConklinR.Invivo pharmacokineticsandpharmacodynamicsofanewtriazole, voriconazole,inamurinecandidiasismodel.Antimicrob AgentsChemother.2003;47:3165–9.
19.AndesD,StamstedT,ConklinR.Pharmacodynamicsof amphotericinBinaneutropenic-mouse
disseminated-candidiasismodel.AntimicrobAgents Chemother.2001;45:922–6.
20.LouieA,DezielM,LiuW,DrusanoMF,GumboT,DrusanoGL. Pharmacodynamicsofcaspofungininamurinemodelof systemiccandidiasis:importanceofpersistenceof caspofunginintissuestounderstandingdrugactivity. AntimicrobAgentsChemother.2005;49:5058–68.
21.AndesD,DiekemaDJ,PfallerMA,etal.Invivo
pharmacodynamiccharacterizationofanidulafunginina neutropenicmurinecandidiasismodel.AntimicrobAgents Chemother.2008;52:539–50.
22.Rodriguez-TudelaJL,AlmiranteB,Rodriguez-PardoD,etal. CorrelationoftheMICanddose/MICratiooffluconazoleto thetherapeuticresponseofpatientswithmucosal
candidiasisandcandidemia.AntimicrobAgentsChemother. 2007;51:3599–604.
inpatientswithcandidemia.AntimicrobAgentsChemother. 2008;52:3022–8.
24.ErnstEJ,KlepserME,PfallerMA.Postantifungaleffectsof echinocandin,azole,andpolyeneantifungalagentsagainst
CandidaalbicansandCryptococcusneoformans.Antimicrob AgentsChemother.2000;44:1108–11.
25.WiederholdNP,TamVH,ChiJ,PrinceRA,KontoyiannisDP, LewisRE.PharmacodynamicactivityofamphotericinB deoxycholateisassociatedwithpeakplasmaconcentrations inaneutropenicmurinemodelofinvasivepulmonary aspergillosis.AntimicrobAgentsChemother.2006;50: 469–73.
26.AndesD,SafdarN,MarchilloK,ConklinR.
Pharmacokinetic-pharmacodynamiccomparisonof amphotericinB(AMB)andtwolipid-associatedAMB preparations,liposomalAMBandAMBlipidcomplex,in murinecandidiasismodels.AntimicrobAgentsChemother. 2006;50:674–84.
27.Al-NakeebZ,PetraitisV,GoodwinJ,PetraitieneR,WalshTJ, HopeWW.PharmacodynamicsofamphotericinB
deoxycholate,amphotericinBlipidcomplex,andliposomal amphotericinBagainstAspergillusfumigatus.Antimicrob AgentsChemother.2015;59:2735–45.
28.GallisHA.AmphotericinB:acommentaryonitsroleasan antifungalagentandasacomparativeagentinclinicaltrials. ClinInfectDis.1996;22Suppl.2:S145–7.
29.AtkinsonAJJr,BennettJE.AmphotericinBpharmacokinetics inhumans.AntimicrobAgentsChemother.1978;13:271–6.
30.BekerskyI,FieldingRM,DresslerDE,LeeJW,BuellDN,Walsh TJ.PlasmaproteinbindingofamphotericinBand
pharmacokineticsofboundversusunboundamphotericinB afteradministrationofintravenousliposomalamphotericinB (AmBisome)andamphotericinBdeoxycholate.Antimicrob AgentsChemother.2002;46:834–40.
31.BekerskyI,FieldingRM,DresslerDE,LeeJW,BuellDN,Walsh TJ.Pharmacokinetics,excretion,andmassbalanceof liposomalamphotericinB(AmBisome)andamphotericinB deoxycholateinhumans.AntimicrobAgentsChemother. 2002;46:828–33.
32.AdedoyinA,BernardoJF,SwensonCE,etal.Pharmacokinetic profileofABELCET(amphotericinBlipidcomplexinjection): combinedexperiencefromphaseIandphaseIIstudies. AntimicrobAgentsChemother.1997;41:2201–8.
33.Wong-BeringerA,JacobsRA,GuglielmoBJ.Lipidformulations ofamphotericinB:clinicalefficacyandtoxicities.ClinInfect Dis.1998;27:603–18.
34.GrollAH,GiriN,PetraitisV,etal.Comparativeefficacyand distributionoflipidformulationsofamphotericinBin experimentalCandidaalbicansinfectionofthecentralnervous system.JInfectDis.2000;182:274–82.
35.StrengerV,MeinitzerA,DonnererJ,etal.AmphotericinB transfertoCSFfollowingintravenousadministrationof liposomalamphotericinB.JAntimicrobChemother. 2014;69:2522–6.
36.HongY,ShawPJ,NathCE,etal.Populationpharmacokinetics ofliposomalamphotericinBinpediatricpatientswith malignantdiseases.AntimicrobAgentsChemother. 2006;50:935–42.
37.CornelyOA,MaertensJ,BresnikM,etal.Liposomal
amphotericinBasinitialtherapyforinvasivemoldinfection: arandomizedtrialcomparingahigh-loadingdoseregimen withstandarddosing(AmBiLoadtrial).ClinInfectDis. 2007;44:1289–97.
38.SanatiH,BelangerP,FrattiR,GhannoumM.Anewtriazole, voriconazole(UK-109,496),blockssterolbiosynthesisin
CandidaalbicansandCandidakrusei.AntimicrobAgents Chemother.1997;41:2492–6.
39.HofH.Anew,broad-spectrumazoleantifungal:posaconazole –mechanismsofactionandresistance,spectrumofactivity. Mycoses.2006;49Suppl.1:2–6.
40.LouieA,DrusanoGL,BanerjeeP,etal.Pharmacodynamicsof fluconazoleinamurinemodelofsystemiccandidiasis. AntimicrobAgentsChemother.1998;42:1105–9.
41.DebruyneD.Clinicalpharmacokineticsoffluconazolein superficialandsystemicmycoses.ClinPharmacokinet. 1997;33:52–77.
42.KethireddyS,AndesD.CNSpharmacokineticsofantifungal agents.ExpertOpinDrugMetabToxicol.2007;3:573–81.
43.AndesD,ForrestA,LepakA,NettJ,MarchilloK,LincolnL. Impactofantimicrobialdosingregimenonevolutionofdrug resistanceinvivo:fluconazoleandCandidaalbicans. AntimicrobAgentsChemother.2006;50:2374–83.
44.AndesD,LepakA,NettJ,LincolnL,MarchilloK.Invivo fluconazolepharmacodynamicsandresistancedevelopment inapreviouslysusceptibleCandidaalbicanspopulation examinedbymicrobiologicandtranscriptionalprofiling. AntimicrobAgentsChemother.2006;50:2384–94.
45.GonzalezJM,AgudeloM,LeivaLM,RodriguezCA,VesgaO, editors.StandardizationofamurinemodelofCandidaalbicans
infectiontostudytherapeuticequivalence(TE)offluconazole (FCZ)generics.InterscienceConferenceonAntimicrobial AgentsandChemotherapy,AmericanSocietyfor Microbiology;2012.
46.WarnPA,SharpA,ParmarA,MajithiyaJ,DenningDW,Hope WW.Pharmacokineticsandpharmacodynamicsofanovel triazole,isavuconazole:mathematicalmodeling,importance oftissueconcentrations,andimpactofimmunestatuson antifungaleffect.AntimicrobAgentsChemother. 2009;53:3453–61.
47.PurkinsL,WoodN,GhahramaniP,GreenhalghK,AllenMJ, KleinermansD.Pharmacokineticsandsafetyofvoriconazole followingintravenous-tooral-doseescalationregimens. AntimicrobAgentsChemother.2002;46:2546–53.
48.CLSI.Referencemethodforbrothdilutionantifungal susceptibilitytestingofyeasts.M27-S4.Wayne,PA:Clinical andLaboratoryStandardInstitute;2012.
49.MavridouE,BruggemannRJ,MelchersWJ,VerweijPE,Mouton JW.Impactofcyp51Amutationsonthepharmacokineticand pharmacodynamicpropertiesofvoriconazoleinamurine modelofdisseminatedaspergillosis.AntimicrobAgents Chemother.2010;54:4758–64.
50.LepakAJ,MarchilloK,VanheckerJ,AndesDR.Posaconazole pharmacodynamictargetdeterminationagainstwild-type andCyp51mutantisolatesofAspergillusfumigatusinan invivomodelofinvasivepulmonaryaspergillosis.Antimicrob AgentsChemother.2013;57:579–85.
51.HowardSJ,LestnerJM,SharpA,etal.Pharmacokineticsand pharmacodynamicsofposaconazoleforinvasivepulmonary aspergillosis:clinicalimplicationsforantifungaltherapy.J InfectDis.2011;203:1324–32.
52.ConteJEJr,DeVoeC,LittleE,GoldenJA.Steady-state
intrapulmonarypharmacokineticsandpharmacodynamicsof posaconazoleinlungtransplantrecipients.Antimicrob AgentsChemother.2010;54:3609–13.
53.PascualA,CalandraT,BolayS,BuclinT,BilleJ,MarchettiO. Voriconazoletherapeuticdrugmonitoringinpatientswith invasivemycosesimprovesefficacyandsafetyoutcomes.Clin InfectDis.2008;46:201–11.
54.ParkWB,KimNH,KimKH,etal.Theeffectoftherapeutic drugmonitoringonsafetyandefficacyofvoriconazolein invasivefungalinfections:arandomizedcontrolledtrial.Clin InfectDis.2012;55:1080–7.
agents:guidelinesfromtheBritishSocietyforMedical Mycology.JAntimicrobChemother.2014;69:1162–76.
56.CourtneyR,PaiS,LaughlinM,LimJ,BatraV. Pharmacokinetics,safety,andtolerabilityoforal
posaconazoleadministeredinsingleandmultipledosesin healthyadults.AntimicrobAgentsChemother.
2003;47:2788–95.
57.WalshTJ,RaadI,PattersonTF,etal.Treatmentofinvasive aspergillosiswithposaconazoleinpatientswhoare refractorytoorintolerantofconventionaltherapy:an externallycontrolledtrial.ClinInfectDis.2007;44: 2–12.
58.DoltonMJ,BruggemannRJ,BurgerDM,McLachlanAJ. Understandingvariabilityinposaconazoleexposureusingan integratedpopulationpharmacokineticanalysis.Antimicrob AgentsChemother.2014;58:6879–85.
59.UllmannAJ,CornelyOA,BurchardtA,etal.Pharmacokinetics, safety,andefficacyofposaconazoleinpatientswith
persistentfebrileneutropeniaorrefractoryinvasivefungal infection.AntimicrobAgentsChemother.2006;50: 658–66.
60.ArendrupMC,Cuenca-EstrellaM,Lass-FlorlC,HopeWW, EuropeanCommitteeonAntimicrobialSusceptibilityTesting SubcommitteeonAntifungalSusceptibilityT.EUCAST technicalnoteonAspergillusandamphotericinB, itraconazole,andposaconazole.ClinMicrobiolInfect. 2012;18:E248–50.
61.DuraniU,ToshPK,BarretoJN,EstesLL,JannettoPJ,TandeAJ. Retrospectivecomparisonofposaconazolelevelsinpatients takingthedelayed-releasetabletversustheoralsuspension. AntimicrobAgentsChemother.2015;59:4914–8.
62.AndesDR,DiekemaDJ,PfallerMA,MarchilloK,BohrmuellerJ. Invivopharmacodynamictargetinvestigationformicafungin againstCandidaalbicansandC.glabratainaneutropenic murinecandidiasismodel.AntimicrobAgentsChemother. 2008;52:3497–503.
63.WiederholdNP,KontoyiannisDP,ChiJ,PrinceRA,TamVH, LewisRE.Pharmacodynamicsofcaspofungininamurine modelofinvasivepulmonaryaspergillosis:evidenceof concentration-dependentactivity.JInfectDis. 2004;190:1464–71.
64.LewisRE,AlbertND,KontoyiannisDP.Comparisonofthe dose-dependentactivityandparadoxicaleffectof
caspofunginandmicafungininaneutropenicmurinemodel ofinvasivepulmonaryaspergillosis.JAntimicrobChemother. 2008;61:1140–4.
65.GumboT,DrusanoGL,LiuW,etal.Anidulafungin pharmacokineticsandmicrobialresponseinneutropenic micewithdisseminatedcandidiasis.AntimicrobAgents Chemother.2006;50:3695–700.
66.StevensDA,EspirituM,ParmarR.Paradoxicaleffectof caspofungin:reducedactivityagainstCandidaalbicansathigh drugconcentrations.AntimicrobAgentsChemother. 2004;48:3407–11.
67.ShieldsRK,NguyenMH,DuC,PressE,ChengS,ClancyCJ. ParadoxicaleffectofcaspofunginagainstCandida
bloodstreamisolatesismediatedbymultiplepathwaysbut eliminatedinhumanserum.AntimicrobAgentsChemother. 2011;55:2641–7.
68.LeitnerJM,MeyerB,FuhrmannV,etal.Multiple-dose pharmacokineticsofanidulafunginduringcontinuous venovenoushaemofiltration.JAntimicrobChemother. 2011;66:880–4.
69.PfallerMA,BoykenL,HollisRJ,etal.Invitrosusceptibilityof invasiveisolatesofCandidaspp.toanidulafungin,
caspofungin,andmicafungin:sixyearsofglobalsurveillance. JClinMicrobiol.2008;46:150–6.
70.AndesD,DiekemaDJ,PfallerMA,BohrmullerJ,MarchilloK, LepakA.Invivocomparisonofthepharmacodynamictargets forechinocandindrugsagainstCandidaspecies.Antimicrob AgentsChemother.2010;54:2497–506.
71.CLSI.ClinicalbreakpointsforCandidaandtheechinocandins. Subcommitteeonantifungalsusceptibilitytests.Wayne,PA: ClinicalandLaboratoryStandardInstitute;2010.
72.ReboliAC,RotsteinC,PappasPG,etal.Anidulafunginversus fluconazoleforinvasivecandidiasis.NEnglJMed.
2007;356:2472–82.
73.KuseER,ChetchotisakdP,daCunhaCA,etal.Micafungin versusliposomalamphotericinBforcandidaemiaand invasivecandidosis:aphaseIIIrandomiseddouble-blind trial.Lancet.2007;369:1519–27.
74.PfallerMA,DiekemaDJ,Ostrosky-ZeichnerL,etal. CorrelationofMICwithoutcomeforCandidaspeciestested againstcaspofungin,anidulafungin,andmicafungin:analysis andproposalforinterpretiveMICbreakpoints.JClin
Microbiol.2008;46:2620–9.
75.AndesD,AmbrosePG,HammelJP,etal.Useof
pharmacokinetic-pharmacodynamicanalysestooptimize therapywiththesystemicantifungalmicafunginforinvasive candidiasisorcandidemia.AntimicrobAgentsChemother. 2011;55:2113–21.
76.AutmizguineJ,GuptillJT,Cohen-WolkowiezM,BenjaminDK Jr,CapparelliEV.Pharmacokineticsandpharmacodynamics ofantifungalsinchildren:clinicalimplications.Drugs. 2014;74:891–909.
77.NucciM,Thompson-MoyaL,Guzman-BlancoM,etal. Recommendationsforthemanagementofcandidemiain adultsinLatinAmerica.LatinAmericaInvasiveMycosis Network.RevIberoamMicol.2013;30:179–88.
78.NicolauDP,FreemanCD,BelliveauPP,NightingaleCH,Ross JW,QuintilianiR.Experiencewithaonce-daily
aminoglycosideprogramadministeredto2,184adult patients.AntimicrobAgentsChemother.1995;39:650–5.