w w w . r b o . o r g . b r
Original
Article
Acromioclavicular
dislocation:
postoperative
evaluation
of
the
coracoclavicular
ligaments
using
magnetic
resonance
夽
Rafael
Salomon
Silva
Faria,
Fabiano
Rebouc¸as
Ribeiro,
Bruno
de
Oliveira
Amin
∗,
Antonio
Carlos
Tenor
Junior,
Miguel
Pereira
da
Costa,
Cantídio
Salvador
Filardi
Filho,
Cleber
Gonc¸alves
Batista,
Rômulo
Brasil
Filho
HospitaldoServidorPúblicoEstadualFranciscoMoratodeOliveira,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11September2013 Accepted13March2014 Availableonline24April2015
Keywords:
Acromioclavicularjoint Ligaments
Magneticresonanceimaging
a
b
s
t
r
a
c
t
Objective:Toradiologicallyevaluatethehealingofthecoracoclavicularligamentsafter sur-gicaltreatmentforacromioclaviculardislocation.
Methods:Tenpatientswhohadundergonesurgicaltreatmentforacromioclavicular disloca-tionviaaposterosuperiorrouteatleastoneyearearlierwereinvitedtoreturnforradiological assessmentusingmagneticresonance.Thisevaluationwasdonebymeansofanalogywith thescaledescribedintheliteratureforstudyingthehealingoftheanteriorcruciateligament ofthekneeandformeasuringthehealedcoracoclavicularligaments.
Results:Ascarstructureoffibrousappearancehadformedin100%ofthecases.In50%of thecases,theimagesofthisstructurehadagoodappearance,whiletheother50%were deficient.
Conclusion: Latepostoperativeevaluationusingmagneticresonance,onpatientswhohad beentreatedforacuteacromioclaviculardislocationusingaposterosuperiorrouteinthe shoulder,showedthatthecoracoclavicularligamentshadhealedin100%ofthecases,but thatthishealingwasdeficientin50%.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Luxac¸ão
acromioclavicular:
avaliac¸ão
pós-operatória
dos
ligamentos
coracoclaviculares
por
ressonância
magnética
Palavraschave:
Articulac¸ãoacromioclavicular
r
e
s
u
m
o
Objetivo:Avaliarradiologicamenteacicatrizac¸ãodosligamentoscoracoclavicularesapóso tratamentocirúrgicoparaluxac¸ãoacromioclavicular.
夽
WorkdevelopedintheShoulderandElbowGroupoftheDepartmentofOrthopedicsandTraumatology,HospitaldoServidorPúblico EstadualFranciscoMoratodeOliveira,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](B.d.O.Amin).
http://dx.doi.org/10.1016/j.rboe.2015.04.007
Ligamentos
Imagemporressonância magnética
Métodos: Foramconvocados10pacientessubmetidosaotratamentocirúrgicoparaluxac¸ão acromioclavicularpelaviaposterossuperior,comtempodepós-operatóriomínimodeum ano,paraavaliac¸ãoradiológicaporressonânciamagnética.Essaavaliac¸ãofoifeitapormeio deanalogiacomaescaladescritanaliteraturaparaestudodacicatrizac¸ãodoligamento cruzadoanteriordojoelhoepelaaferic¸ãodasmedidasdosligamentoscoracoclaviculares cicatrizados.
Resultados: Houveformac¸ãodeestruturacicatricialaparentementefibrosaem100%dos casos.Em50%doscasos,aimagemdessaestruturaeradebomaspectoàressonância nuclearmagnéticae50%deficiente.
Conclusão: Aavaliac¸ãoporressonâncianuclearmagnéticadospacientesempós-operatório tardiodecirurgiaparatratamentodaluxac¸ãoacromioclavicularaguda,pelavia posterossu-periordoombro,mostrouacicatrizac¸ãodosligamentoscoracoclavicularesem100%dos casos,sendo50%deficiente.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Acromioclaviculardislocation(ACD)isatraumatic patholog-icalconditionoftheshoulderthatpredominantlyoccursin youngadults.Theanatomicalandbiomechanicalalterations causedbythetearingofthecoracoclavicularligamentsarea crucialfactorindecidingwhethertotreattheinjurysurgically ornon-surgically.1–3
The well-established radiographic classification system described byRockwood1 usesthe contralateralshoulder as
acomparisonparameter,asfollows:noabnormalityofthe coracoclaviculardistance(ACDgradeI);changetothe cora-coclavicular distance, but less than 25% (ACD grade II); coracoclaviculardistanceincreasedby25–100% (ACD grade III);posteriordisplacementoftheclavicle(ACDgradeIV); cora-coclavicularspaceincreasedby100–300%(ACDgradeV);and coracoclavicularspacediminishedorinverted(ACDgradeVI). Thecoracoclavicularligamentsarethemainstabilizersof the acromioclavicular joint and the main supports forthe upperlimbs.1–3Nevertheless,littleisknownabouttheir
heal-ingaftersurgicaltreatmentforACD.
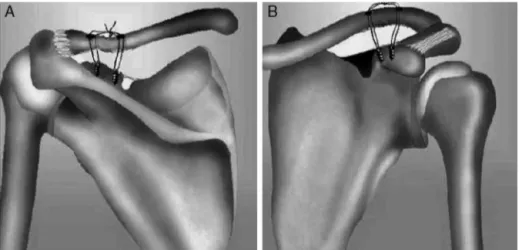
Fig.1–Schematicdrawingdemonstratingthepositioningoftheanchorsandholesdrilledintheclavicle,in(A)posterior viewand(B)anteriorview.
Materials
and
methods
Magnetic resonance imaging(MRI) on 10 patients aged 20 to 50 years (bothmen and women), withinitial diagnoses ofACDgradesIII toV,was evaluated. Thesepatients were selected randomly(drawn)fromamongourpopulation. All ofthemhadbeenoperatedbythesameteamandwiththe samesurgicaltechnique:bindingoftheclavicletothecoracoid processusingtwometalanchors(5mmindiameter,with non-absorbablethreads),bymeansofaposterosuperioraccessin the shoulder4 (Fig. 1A andB). Theminimumpostoperative
follow-upwasoneyear.
The exclusion criteria were as follows: treatment per-formedusingaclosedmanner;surgicaltreatmentinwhich othertechniqueswereused(suchastransferofthe coraco-clavicularligamentstothedistalclavicle);andagelessthan 20ormorethan50years.
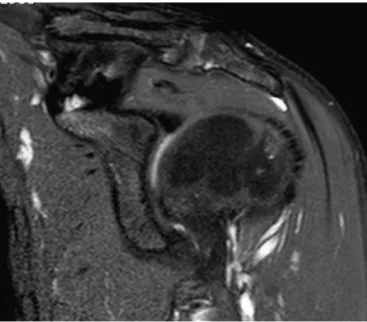
Fig.2–MRIusingthestandardsdescribedforviewingthe coracoclavicularligamentsofapatientwhounderwent surgicaltreatmentforACD.
linethat was tracedout betweenthe apex ofthe coracoid processandtheapexofthelessertubercleofthehumerus. Theslices were of thickness 3.5mm, T1and T2-weighted, and were produced with the patient in the neutral posi-tion.Theimagingparameterswereasfollows:field ofview from145mm×145mmto150mm×150mm;matrix sizeof 353×512or256×512;andsectionthicknessof3.5mm.5The examinationswereevaluatedjointlybyanorthopedistwho wasaspecialistinshoulderandelbowsurgeryandatrainee physicianinthehospital’sshoulderandelbowgroup.
Toevaluatethepresenceandqualityofhealingofthe cora-coclavicular ligaments, ascale previously described in the literaturewasused.6Thiswasascaleforevaluatingthe
heal-ingofgraftsfromtheflexortendonsoftheknee,whichare usedinreconstructionsfollowinganteriorcruciateligament injury.Thisscalegradestheimageoftheligamentthatwas obtainedusingMRI,intofourstagesaccordingtotheirsizeand signsofhomogeneity(Table1).Ligamentsclassifiedasgrades IandIIcorrelatewithgoodstabilityandcanthereforebe con-sideredtohavehealed,whilethosegradedasIIIandIVare consideredtopresentdeficienthealingorabsenceofhealing. The geometry of the scar tissue encountered (neoliga-ment) was evaluated using the Impax 6.3 client software.
Table1–Gradingforevaluatingligamenthealingby
meansofMRI.
GradeI:Well-definedstraightbandofnormalsizewith homogenouslow-intensitysignal.
GradeII:Well-definedstraightbandwithlow-intensitysignaland pointsshowinghigh-intensitysignal.
GradeIII:Thinbandwithlow-intensitysignalcontainingmass withhigh-intensitysignal.
GradeIV:Abandwithdarkindiscerniblesignal.
Source:Iharaetal.6
Thefollowingmeasurementswere made:length,measured alongthedirectionofthefibersoftheneoligament,fromthe midpointoftheoriginintheclavicletothemidpointofthe insertioninthecoracoidprocess;width,inthecoronalplane initsproximalportion(originintheclavicle)anddistalportion (insertioninthecoracoidprocess);angle,measuredbetween thelinealongwhichthelengthwasmeasuredandastraight linealongtheloweredgeofthedistalclavicle(Fig.3A–C).
Results
ItwasobservedthatintheMRIexamination,allthepatients presentedanimageofscartissueoffibrousappearancethat connectedthedistalclavicletothecoracoidprocess.Infive examinationsthatwereclassifiedasgradeII,itwasconsidered thatgoodligamenthealinghadbeenachieved.Theotherfive examinationsshoweddeficienthealing.Threewereclassified asgradeIIIandtwoasgradeIV.
Regarding the geometry of the healed coracoclavicular ligaments,nodistinctionwasobservedbetweenthetwo lig-aments(conoid andtrapezoid).Onlyasinglescarstructure wasobserved,withvariationinmeasurementsbetweenthe patients(Table2).However,inmostcases,thenewligament was seen to have maintained the trapezoidal appearance ofthecoracoclavicularligaments,suchthattheirclavicular portionwaswiderthantheirdistalportionatthecoracoid pro-cess.TheexaminationsonthepatientsclassifiedasgradeIV (twocases)didnotalloweffectivemeasurements,becauseof theiranatomicalirregularities.
Discussion
To evaluate the healing of the coracoclavicular ligaments, anatomicalparametersthathadpreviouslybeenestablished forknee ligament injuries were usedinthe present study, giventhatnopreestablishedparametersforthe coracoclavic-ularligamentswereencounteredintheliterature.Thetime period taken into consideration for healing to take place among the patients who were treated surgically for ACD wasdeterminedbasedontheminimumpostoperativetime neededfortheanteriorcruciateligamentoftheknee, recon-structedusingagraft fromtheflexortendons,toachievea histological state similar to the original. Thisranges from 30 to52weeks,according totheliteratureconsulted.7 Ina
studyconductedbyClayeretal.,8usingsequentialMRI
exam-inationson sixpatientswhounderwent surgicaltreatment forACD, inwhichanabsorbableloop wasusedfor coraco-clavicularfixation,itwasobservedthatsixmonthsafterthe operation,astructureoffibrousappearanceconnectingthe coracoidprocesstotheclaviclecouldalreadybeseen.
MRIisanefficientandaccurateexaminationfordetailed evaluations on the ligament structures of the joints of the humanbody, suchas the shoulderand knee.9 Nemec
etal.10comparedMRItoradiographyforclassifyingACDthat
Fig.3–Parametersusedformeasuringtheneoligamentbetweenthecoracoidprocessandtheclavicle,inapatientatalate postoperativetimeaftersurgicaltreatmentforACD.A,length;B,widthattheoriginintheclavicleandinsertioninthe coracoidprocess;C,angleinrelationtothedistalclavicle.
Inourstudy,astructureofscartissuecharacteristicswas observed using MRI in 100%of the cases operated. It had a fibrous appearance, with trapezoidal format and coraco-clavicular ligature. However, there were signs of deficient healingin50%ofthecases.Thesefindingswerecompatible withthoseofthestudybyClayeretal.,8inwhichformation
of ananatomical structureof fibrous appearancewas also observed in the regions of the coracoclavicular ligaments, whichsuggeststhattheseligamentshadhealed.
Inananatomicalstudyonthecoracoclavicularligaments, Harrisetal.11mademeasurementson24shouldersof
cadav-ers and found the following means: length of the conoid
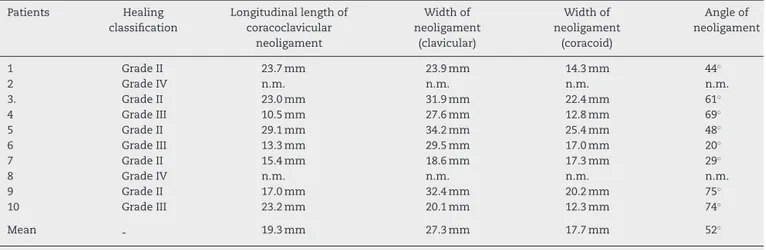
Table2–ResultsfromlatepostoperativeMRIevaluationsonpatientswhoweretreatedsurgicallyforACD.
Patients Healing
classification
Longitudinallengthof coracoclavicular
neoligament
Widthof neoligament
(clavicular)
Widthof neoligament
(coracoid)
Angleof neoligament
1 GradeII 23.7mm 23.9mm 14.3mm 44◦
2 GradeIV n.m. n.m. n.m. n.m.
3. GradeII 23.0mm 31.9mm 22.4mm 61◦
4 GradeIII 10.5mm 27.6mm 12.8mm 69◦
5 GradeII 29.1mm 34.2mm 25.4mm 48◦
6 GradeIII 13.3mm 29.5mm 17.0mm 20◦
7 GradeII 15.4mm 18.6mm 17.3mm 29◦
8 GradeIV n.m. n.m. n.m. n.m.
9 GradeII 17.0mm 32.4mm 20.2mm 75◦
10 GradeIII 23.2mm 20.1mm 12.3mm 74◦
Mean 19.3mm 27.3mm 17.7mm 52◦
ligament,19.4mm;lengthofthetrapezoidligament,19.3mm; width oftheorigin ofthe conoidligament on the clavicle, 20.6mm;widthoftheinsertionoftheconoidligamentinthe coracoidprocess,10.6mm;widthoftheoriginofthetrapezoid ligamentontheclavicle,21.7mm;andwidthoftheinsertion ofthetrapezoid ligamentinthecoracoidprocess,14.0mm. InourstudyusingMRI,similarmeansforthelengthofthe neoligamentthatformedaftertheoperationwereobtained. Themeans forthewidths could notbecomparedbecause ofthedifferencesinshapebetweenthecoracoclavicular liga-mentsandtheneoligament.
Noclinicalandbiomechanicalcorrelationsweremadein relationtothe findings ofthis study,because ofthe small samplespace.
Conclusion
ThelatepostoperativeMRIevaluationsonpatientswhowere treatedsurgicallyforacuteACDbymeansofaposterosuperior accessintheshouldershowedhealingofthecoracoclavicular ligamentsin100%ofthecases,although50%weredeficient.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. CollinsDN.Disordersofacromioclavicularjoint.In:
RockwoodCAJr,MatsenFA3rd,WirthMA,LippittSB,editors. Theshoulder.4thed.Philadelphia:SaundersElsevier;2009.p. 453–526.
2.CosticRS,VanguraA,FenwickJA,RodoskyMW,DebskiRE. Viscoelasticbehaviorandstructuralpropertiesofthe coracoclavicularligaments.ScandJMedSciSports. 2003;13(5):305–10.
3.DawsonPA,AdamsonGJ,PinkMM,KornswietM,LinS, ShankwilerJA,LeeTQ.Relativecontributionof acromioclavicularjointcapsuleandcoracoclavicular ligamentstoacromioclavicularstability.JShoulderElbow Surg.2009;18(2):237–44.
4.DalMolinDC,RibeiroFR,BrasilFilhoR,FilardiJuniorCS, TenorJuniorAC,StippWN,etal.Viadeacessocirúrgico posterossuperiorparaotratamentodasluxac¸ões acromioclaviculares:resultadosde84casosoperados.Rev BrasOrtop.2012;47(5):563–7.
5.AlyasF,CurtisM,SpeedC,SaifuddinA,ConnellD.MR imagingappearancesofacromioclavicularjointdislocation. Radiographics.2008;28(2):463–79.
6.IharaH,MiwaM,DeyaK,TorisuK.MRIofanteriorcruciate ligamenthealing.JComputAssistTomogr.1996;20(2): 317–21.
7.FuFH,BennettCH,LattermannC,MaCB.Currenttrendsin anteriorcruciateligamentreconstruction.PartI:Biologyand biomechanicsoreconstruction.AmJSportsMed.
1999;27(6):821–30.
8.ClayerM,SlavotinekJ,KrishnanJ.Theresultsof
coraco-clavicularslingsforacromio-claviculardislocation. AustNZJSurg.1997;67(6):343–6.
9.CohenM,MarcondesFB.Lesõesligamentares.In:CohenM, MattarJúniorR,GarciaFilhoRJ,editors.Tratadodeortopedia. Roca:SãoPaulo;2007.p.401–11.
10.NemecU,OberleitnerG,NemecSF,GruberM,WeberM, CzernyC,KrestanCR.MRIversusradiographyof acromioclavicularjointdislocation.AJRAmJRoentgenol. 2011;197(4):968–73.