REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Effects
of
lidocaine
and
esmolol
infusions
on
hemodynamic
changes,
analgesic
requirement,
and
recovery
in
laparoscopic
cholecystectomy
operations
Serpil
Dagdelen
Dogan,
Faik
Emre
Ustun,
Elif
Bengi
Sener,
Ersin
Koksal
∗,
Yasemin
Burcu
Ustun,
Cengiz
Kaya,
Fatih
Ozkan
OndokuzMayısUniversity,MedicineFaculty,AnesthesiologyDepartment,Samsun,Turkey
Received10July2014;accepted7August2014 Availableonline27November2014
KEYWORDS
Lidocaine; Esmolol; Recovery; Laparoscopic cholecystectomy
Abstract
Objective: Wecomparedtheeffectsoflidocaineandesmololinfusionsonintraoperative
hemo-dynamic changes,intraoperative andpostoperativeanalgesic requirements,andrecovery in laparoscopiccholecystectomysurgery.
Methods:Thefirstgroup(n=30)receivedIVlidocaineinfusionsatarateof1.5mg/kg/minand
thesecondgroup(n=30)receivedIVesmololinfusionsatarateof1mg/kg/min.Hemodynamic changes,intraoperativeandpostoperativeanalgesicrequirements,andrecoverycharacteristics wereevaluated.
Results:In thelidocainegroup,systolicarterialbloodpressuresvalueswerelowerafterthe
inductionofanesthesiaandat20minfollowingsurgicalincision(p<0.05).Awakeningtimewas shorterintheesmololgroup(p<0.001);RamsaySedationScalescoresat10minafterextubation werelowerintheesmololgroup(p<0.05).ThemodifiedAldretescoresatallmeasurementtime pointsduringtherecoveryperiodwererelativelylowerinthelidocainegroup(p<0.05).The time to attainamodified Aldrete score of≥9pointswas prolongedinthe lidocainegroup (p<0.01).PostoperativerestinganddynamicVASscoreswerehigherinthelidocainegroupat 10and20minafterextubation(p<0.05,p<0.01,respectively).Analgesicsupplementswere lessfrequentlyrequiredinthelidocainegroup(p<0.01).
Conclusion: In laparoscopic cholecystectomies, lidocaine infusion had superiorities over
esmololinfusionsregardingthesuppressionofresponsestotrachealextubationand postopera-tiveneedforadditionalanalgesicagentsinthelongrun,whileesmololwasmoreadvantageous withrespecttorapidrecoveryfromanesthesia,attenuationofearlypostoperativepain,and modifiedAldreterecovery(MAR)scoresandtimetoreachMARscoreof9points.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](E.Koksal).
http://dx.doi.org/10.1016/j.bjane.2014.08.005
PALAVRAS-CHAVE
Lidocaina; Esmolol; Recuperac¸ão; Colecistectomia laparoscópica
Efeitosdasinfusõesdelidocaínaeesmololsobreasalterac¸õeshemodinâmicas, necessidadedeanalgésicoserecuperac¸ãoapóscolecistectomialaparoscópica
Resumo
Objetivo:Comparamososefeitosdeinfusõesdelidocaínaeesmololsobreasalterac¸ões
hemod-inâmicasnoperíodointraoperatório,anecessidadedeanalgésicosintra-epós-operatoriamente earecuperac¸ãoapóscolecistectomialaparoscópica.
Métodos: O primeiro grupo (n=30) recebeu infusões IV de lidocaína a uma taxa de
1,5mg/kg/mineosegundogrupo(n=30)recebeuinfusõesIVdeesmololaumataxade1mg kg/min.Alterac¸õeshemodinâmicas, necessidadedeanalgésicosnointra-epós-operatórioe característicasdarecuperac¸ãoforamavaliadas.
Resultados: Nogrupolidocaína,osvaloresdapressãoarterialsistólicaforammenoresapósa
induc¸ãodaanestesiae20minutosapósaincisãocirúrgica(p<0,05).Otempoatéodespertar foimenornogrupoesmolol(p<0,001),osescoresnaescaladeSedac¸ãodeRamsay10minutos apósaextubac¸ãoforammenoresnogrupoesmolol(p<0,05).OsescoresdeAldretemodificados emtodosostemposmensuradosduranteoperíododerecuperac¸ãoforamrelativamentebaixos nogrupolidocaína(p<0,05).OtemponecessárioparaatingirumescoredeAldrete≥9 pon-tosfoiprolongadonogrupolidocaína(p<0,01).OsescoresEvaemrepousoeemmovimento nopós-operatório forammaioresno grupolidocaína nosminutos 10 e20 apósaextubac¸ão (p<0,05,p<0,01,respectivamente).Analgésicossuplementaresforamnecessárioscommenos frequêncianogrupolidocaína(p<0,01).
Conclusão:Emcolecistectomialaparoscópica,ainfusãodelidocaína foisuperioràsinfusões
deesmololquantoasuprimirasrespostasàextubac¸ãotraquealenecessidadedeanalgésicos adicionaisnopós-operatório,enquantoesmololfoimaisvantajosoquantoàrápidarecuperac¸ão daanestesia,àatenuac¸ãodadornopós-operatórioimediatoeaosescoresderecuperac¸ãode Aldretemodificado(RAM)eotempoatéatingiroescoreRAMde9pontos.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
During the perioperative period, as a hemodynamic response to laryngoscopy, intubation, and surgical exci-sion, complications including tachycardia, hypertension, myocardial ischemia, arrhythmia, myocardial infarction, andcerebral hemorrhagescan beseen. To prevent devel-opmentoftheseunwantedeffects,variousmeasuressuch asincreasingthedepthofanesthesiaandtheadministration oftopicalanesthesia,IVlidocaine,vasodilators,alfa2 ago-nists,beta-adrenergicblockers,opioids,andprecurarizaton procedureshavebeenimplemented.1---4
In the control of unfavorable hemodynamic changes developedsecondarytointubation,lidocainecanbe admin-isteredintravenouslybeforetheinductionofanesthesiaand severalstudieshavedemonstrateditspreventiveeffectson postoperativepain.5---7
Esmolol is effective in the suppression of adrener-gicresponsesagainstlaryngoscopicprocedures,intubation, and many other perioperative stimulations.8,9
Further-more, some studies have indicated that beta adrenergic receptor blockers decrease the need for anesthetics and postoperativeanalgesicconsumption.10---12Eventhoughpain
scores are lower in laparoscopic colecystectomy relative to conventional open chlecystectomy, multimodal anal-gesicregimensshouldbeperformed,includingpreoperative treatment.13
Though many studies have compared the effects of both drugs onhemodynamicresponses, comparative stud-iesrelated totheir effectsonrecovery and analgesiaare lacking. In our study, we have aimed to compare the effectsoflidocaineandesmololinfusionsonintraoperative hemodynamic changes, intra-and postoperativeanalgesic requirements,andrecovery.
Materials
and
methods
Thisdouble-blindstudywasperformedon60ASAI-IIpatients aged18---65 yearsscheduled for laparoscopic cholecystec-tomyafterobtaininginformedconsentfromofthepatients. Patientswithallergiestolocalanestheticsandopioids, mor-bidobesity,oradvancedrespiratory,renal,hematological, hepatic or cardiovascular diseases; chronic use of opiate, betaadrenergicreceptorantagonists,oralcohol;anddrug addicts,pregnantwomen,andmentallyretardedcaseswere excludedfromthestudy.Forpremedication,patientswere given 40mg famotidine and 10mg diazepam orally. The patients underwent electrocardiographic (EKG) examina-tions,pulseoxymetricmeasurementsofperipheraloxygen saturation (SpO2), and noninvasive monitoring of arterial pressure.Thepatientswererandomizedinto2groupsusing thesealedenvelopemethod.
2mg/kg/h 3min before the induction of anesthesia. The secondgroup(groupE)wasgivenIVesmololinfusionslowly atarateof1mg/kg/minforatotaldoseof 15g/kg/min 3min before induction of anesthesia. Lidocaine and esmolol infusions were terminated immediately after extubation.
Heart rates (BPM); systolic (SBP), diastolic (DBP), and mean (MABP) arterial blood pressures; and the SpO2 of the patients weremeasured, andadverse effectssuch as bradycardia, hypotension, andarrhythmiaswere recorded preoperatively (t1), after induction (t2), after the intu-bation at 1 (t3) and 5 (t4)min and, during the surgical incision(t5),afterthesurgicalincisionat5(t6),10(t7),15 (t8),20(t9),30(t10),40(t11),50(t12),and60(t13)min, beforeextubation(t14),andaftertheextubationat1(t15) and 5 (t16)min. During induction, 2---2.5mg/kg iv propo-fol, 1g/kg iv fentanyl, and0.1mg/kg iv vecuronium for muscular relaxation were used. For the maintenance of anesthesia, amixtureof 65%N2O and35%O2,desflurane, and IV vecuronium at a dose of 0.01mg/kg for muscular relaxation were administered at 30min intervals. Twenty minutesbefore the estimated end timeof the operation, 75mgIMdiclofenacsodiumand10mgIVmetochlopramide wereadministered. Dosagesof all anestheticagents were tapered 50% at the start of skin suturing and discon-tinued at the last skin suture. The effects of muscular relaxantswerereversedusing0.04mg/kgneostigmineand 0.02mg/kg atropine. The time interval between the dis-continuationofanestheticagentsandthespontaneouseye opening of the patients was recorded asthe ‘‘awakening time.’’
Thepatientswerebroughtintothepost-anesthesiacare unit (PACU) after extubation, and fentanyl was delivered using a patient-controlled analgesia device (PCAD). The PCADwasadjustedtodeliveraninitialbolusdoseof3cm3 (15g)fentanyl (5g/cm3) witha lockouttimeof 20min and a 1-h limit of 45g. A loading dose was not admin-istered. SBP, DBP, MABP, SS, Ramsay Sedation Score, and restinganddynamicVASscoreswererecordedat 10(t17), 20(t18),30(t19),and40(t20)minoftheirPACUstay.The firstdemandfor ananalgesic, totalrequirementfor anes-thesia, modifiedAldretescores at 10,20,30, and40min, andthetimetoachieveaMASof≥9pointswererecorded. The patientsweretransferredtoaservice whentheyhad attainedamodifiedAldretescoreof≥9points.Heartrates (HRs); systolic(SBPs), diastolic (DBPs),and mean arterial (MABPs) blood pressures; respiratory rates; Ramsay seda-tionscores(RSS);maximalrestinganddynamicVASscores; numberofdemands forPCA; amountof analgesics admin-istered; and adverse effects, including nausea, vomiting, pruritus,andconstipation,amongotherswererecordedat 2 (t21), 6 (t22), 12 (t23), and 24 (t24)h of hospital stay intheservice. RestingVASscoresof≥4pointsatanytime duringthepostoperativeperiod,despitepatient-controlled analgesia,necessitated75mgdiclofenacsodiumIM adminis-teredat12hintervals,whichwasrecordedasanadditional needfor analgesia.Thenauseaandvomitingscores ofthe patients were as follows: 0=absence of nausea, 1=mild nausea, 2=moderate nausea and vomiting, 3=frequent vomitingand4=severe vomiting.Metochlopramide(10mg IV)wasadministeredwhen thenauseaand vomitingscore was≥2points.
Statistical
analysis
Thestatisticalanalysisofthedataobtainedwasperformed using the SPSS for Windows 16.0 statistical package pro-gram.The data wereexpressed asarithmetic means±SD (standard deviation), numbers, and percentages. Normal-itytestsfor the distributionof datawere performed. For intergroupcomparisons,thechi-squareandMann---Whitney U tests were used. The Friedman test was employed in intragroupcomparisons.Forparametersshowingintergroup differences,theWilcoxont-testwithBonferronicorrection wasused.Valueswithp<0.05wereacceptedasstatistically significant.
Results
Intergroup difference was not detected for demographic characteristics, age, gender, body weight, or height (p>0.05).
Heartrates (bpm)measured at anytimedidnotdiffer betweenthegroups(p>0.05).Bradycardiadevelopedinthe lidocaine(n=1)andesmolol(n=2)groupsandrespondedto theadministrationof0.5gatropine.
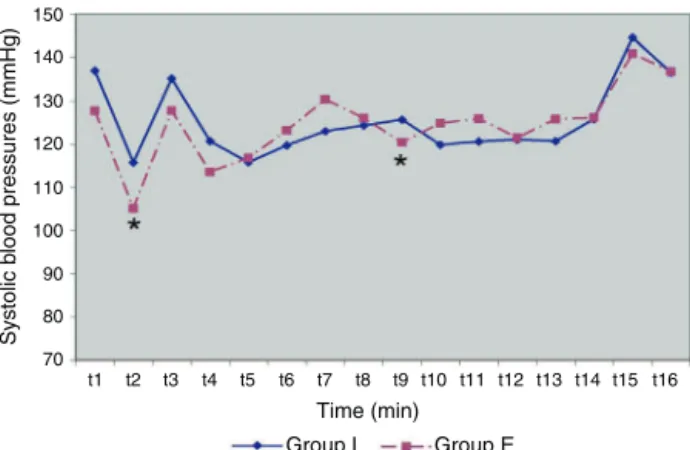
In intergroup comparisons, systolic blood pressures (mmHg) measured following the induction of anesthesia (t2) and 20min (t9) after surgical incision were found to be significantly lower in the esmolol group (respectively, p=0.041;p=0.045)(Fig.1).Inthelidocainegroup, hyper-tensiondevelopedintwopatients,andwastreatedwithiv 100gnitroglycerine.
Themeanarterialbloodpressure(mmHg)intheesmolol groupmeasured aftertheinductionofanesthesia(t2) was lowerrelativetothelidocainegroup(p=0.006)(Fig.2).
Inallofthemeasurementperiods,intergroupdifferences werenotdetectedfordiastolicbloodpressureand periph-eraloxygensaturation(p>0.05).
No intergroup difference was encountered regarding intraoperative fentanyl consumption (group L: 94.66±45.08g; group E: 82.50±28.36g) (p=0.298). Additional fentanyl was required in both the lidocaine (n=10)andesmolol(n=9)groups.
Postoperative systolic blood pressures (mmHg) did not differbetweengroupsinallmeasurementperiods(p>0.05). Hypotensiondevelopedinonepatientinthelidocainegroup,
150
140
130
120
110
100
90
80
70
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12 t13t14 t15 t16 Time (min)
Group L Group E
Systolic b
lood pressures (mmHg)
t1 t2 t3 t4 t5 t6 t7 t8 t9 t10 t11 t12 t13t14 t15t16 Time (min)
Group L Group E
Mean b
lood pressures (mmHg)
110
100
90
80
70
60
50
40
Figure2 Meanbloodpressures(mmHg).*p<0.05.
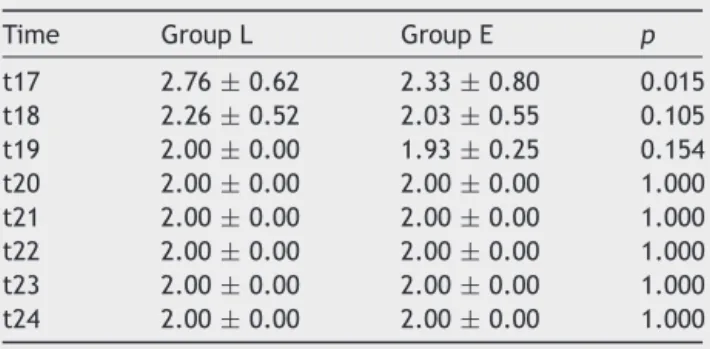
Table1 RamsaySedationScores(mean±SD).
Time GroupL GroupE p
t17 2.76±0.62 2.33±0.80 0.015
t18 2.26±0.52 2.03±0.55 0.105
t19 2.00±0.00 1.93±0.25 0.154
t20 2.00±0.00 2.00±0.00 1.000
t21 2.00±0.00 2.00±0.00 1.000
t22 2.00±0.00 2.00±0.00 1.000
t23 2.00±0.00 2.00±0.00 1.000
t24 2.00±0.00 2.00±0.00 1.000
whilehypertensionoccurredinboththelidocaine(n=1)and esmolol(n=2)groups.
Postoperative diastolic, mean arterial blood pressures andheartrates werenotdifferent betweenthegroups in allmeasurementperiods(p>0.05).
Therecoverytimes(min)ofthecasesweresignificantly shorterintheesmololgroup(groupL:6.55±1.84andgroup E:4.56±1.40)(p=0.0001).
Inintergroup comparisons,theRamsay SedationScores estimated10min afterextubation(t17)werelowerinthe esmololgroup(p=0.015)(Table1).
Themodified Aldretescores duringtherecovery period were significantly lower in the lidocaine group (p<0.05)
(Table2).
ThemodifiedAldretescoresof≥9pointswereattainedin asignificantlyshortertime(min)intheesmololgroup(group L:14.76±3.82andgroupE:12.46±4.80)(p=0.006).
PostoperativeVASvaluescalculatedatrestand10(t17) and20(t18)minafterextubationwerefound tobe signifi-cantlyhigherinthelidocainegroup(p=0.017andp=0.006, respectively).
Table2 ModifiedAldretescores(mean±SD).
Time GroupL GroupE p
t17 8.23±0.43 8.53±0.51 0.018
t18 9.00±0.00 9.27±0.52 0.006
t19 9.30±0.46 9.70±0.46 0.002
t20 9.7±0.46 9.93±0.25 0.002
PostoperativedynamicVASvaluesdetected10(t17)and 20(t18)minafterextubationweresignificantlyhigherinthe lidocainegrouprelativetotheesmololgroup(p=0.021and
p=0.003,respectively).
The number of demands for postoperative PCA, the amount of analgesics administered, and the time to the firstrequirementofanalgesiaestimatedinallmeasurement periodswerenotstatisticallysignificantlydifferentbetween thegroups(p>0.05).
Fewer patients in the lidocaine group required addi-tionalanalgesics[groupL:2(6.7%)andgroupE:11(36.7%)] (p=0.005).
Anystatisticallysignificantintergroupdifferencewasnot detected regarding intra- and postoperative side effects (p>0.05). During the operation, one patient in the lido-cainegroupandtwopatientsintheesmololgroupdeveloped bradycardia responsive to 0.5mg atropine. In the lido-caine group, two patients developed hypertension, which responded to100gnitroglycerine. Duringthe postopera-tive period, hypotension developed in one patientin the lidocaine(n=1)group,whilehypertensionwasnotedinthe lidocaine(n=1)andesmolol(n=2)groups.Nauseaand vomi-ting wereseenin fourpatientsin eachgroup andtreated with10mgmetochlopramide.
Discussion
Thoughlaparoscopiccholecystectomyoffersthepossibility ofrelatively earlydischargefromthehospital, postopera-tive pain, nausea, and vomiting induced by opioids are frequent complaints.13,14 Multimodal analgesic techniques
and adjuvant agents employed todecrease the incidence ofthesesideeffectsmightbeusefulinreducingdosagesof systemicopioids.13,14
Chiaetal.15 administeredesmololinfusionsatarateof
50g/kg/minfollowingaloadingdoseof0.5mg/kgbefore theinduction ofanesthesiain49patientswhohad under-gone abdominalhysterectomy, while 48 patients received normal saline infusions. They also demonstrated that the response of the heart rate and blood pressure to surgi-calincisionandextubationwassignificantlysuppressed in the esmolol group. White et al.16 administered esmolol
infusionsatarateof5g/kg/minfollowingaloadingdose of50mgbeforetheinductionofanesthesiain15 patients undergoing gynecologic laparoscopic surgeries, while 15 patients receivedonly 50mg esmolol IVand thenesmolol infusions(5g/kg/min)followingtheadministrationof1mg nicardipine.Still,15patientsreceivedsalineinfusions.They concludedthatesmolol infusionsperseor incombination withnicardipine were sufficientlyeffective in suppressing intraoperativeacutehemodynamicresponses.Keskinetal.17
hemodynamic responses that developed duringintubation butfailedtoadequatelysuppress hemodynamicresponses thatevolvedduringextubation.
We think that differences among these outcomes are relatedtotheapplicationofpremedication(ifany),drugs usedininduction,anddosesofthestudydrugs.Inaddition, inourstudy,lidocaineandesmololequallydepressed hemo-dynamicresponsestointubation.Eventhoughhemodynamic responsestoextubationweresuppressedmoreeffectivelyin thelidocainegrouprelativetotheesmololgroup,dosesof bothagentsweusedcouldnotcompletelyattenuate hemo-dynamic responses to extubation. Chia et al.15 delivered
esmololinfusionsatarateof50g/kg/minfollowinga load-ingdoseof 0.5mg/kg inpatientsscheduledfor abdominal hysterectomyand found significantly lowerintraoperative opiateand volatileagentconsumption comparedwiththe controlgroup.Topc¸uetal.18statedthatthetotal
consump-tion of remifentanil and propofol was significantly lower in the group of patients scheduled for elective abdomi-nal surgery under total intravenous anesthesia who also receivedosmololinfusionat arateof250g/kg/min com-paredwiththecontrolgroup.Lauwicketal.7investigated
theeffectsof intraoperativelidocaineinfusioninpatients scheduled forlaparoscopic cholecystectomyandindicated lesser consumption of intraoperative fentanyl and desflu-raneinthegroupthatreceivedlidocaineinfusionatarateof 2mg/kg/hfollowingaloadingdoseof1.5mg/kgcompared withthecontrolgroup.Theyalsostatedthatesmolol and lidocaineinfusions ledtolesserintraoperative opiate and volatile agent consumption relative to the control group. However,no study has compared both of these agents in thisrespect.Inourstudy,we couldnotdetect any signifi-cantdifferencebetweenthetotalamountsofintraoperative fentanylconsumedbythegroups.
Koppertetal.19investigatedtheeffectsofperioperative
lidocaine infusion in major abdominal surgeries and initi-atedlidocaineinfusionatarateof1.5mg/kg/hfollowinga loadingdoseof1.5mg/kglidocaineIV30minbeforesurgical incisionin20patientsundergoingmajorabdominal surger-ies.Infusionwasdiscontinued1haftertheterminationof surgery.Theauthorsalsostatedthat,whentheyhadinfused thesamevolumeofphysiologicsalinetothecontrolgroup, they couldnot find any intergroup differencein sedation scores.Collardetal.11analyzedtheeffectsofintraoperative
esmololinfusiononthepostoperativeconsumptionof fen-tanyl inlaparoscopic cholecystectomies.The investigators deliveredesmololto30patientsatarateof5---15g/kg fol-lowingaloadingdoseof1mg/kg,whileanother30patients receivedesmolol infusionsata rateof 0.1---0.5g/kg/min aftera loadingdose of 1g/kg. Furthermore,30patients weregivenphysiologicalsalinesolutions,andshorter recov-ery times were detected in the esmolol group compared withtheothergroups.Manystudieshavedemonstratedthat beta adrenergic blockers thatexert depressiveeffects on thecentralnervoussystemalsodecreasetheneedfor intra-operativeanestheticagents,leadingtorapidrecoveryfrom anesthesia.11,16,20Intheliterature,weencounterednostudy
comparingesmololandlidocaineregardingawakeningtimes and recovery scores. In our study, awakeningtimes were shorterintheesmololgroup.RamsaySedationScores esti-mated10minafterextubationwerefound tobehigherin thelidocainegrouprelativetotheesmololgroup.However,
nosignificantintergroupdifferencewasfoundatother mea-surementtimepoints.ModifiedAldreterecoveryscores in theesmololgroupweresignificantlyhigherinall measure-mentperiods.Similarly, thetimetoachieveascoreof≥9 pointswasalsoshorterintheesmololgroup.
Chiaetal.15investigatedtheeffectsofbetablockerson
postoperativepaininpatientswhohadundergone abdomi-nalhysterectomiesandfoundthattheVASscoresofpatients whoreceivedIVesmololinfusionatarateof50g/kg/min followingaloadingdose of0.5mg/kgbeforetheinduction of anesthesia were similar to those of the control group withsignificantlylowerrequirementsforpostoperative mor-phinesupplementationsintheesmololgroup.Öztürketal.21
administeredesmololinfusionsatarateof5---15g/kg/min following a loading dose of 1mg/kg, while their control group receivedequal volumes of ringer lactateinfusions. Intheesmololgroup,thepostoperativeneedforanalgesics wassignificantlylowerrelativetothecontrolgroup.Collard etal.11 investigatedtheeffects of intraoperative esmolol
infusionsonpostoperativefentanylconsumptioninpatients undergoinglaparoscopiccholecystectomyandadministered esmololinfusionsto30patientsatarateof5---15g/kg/min following a loading dose of 1mg/kg. Whereas 30patients receivedremifentanilinfusion(0.1---0.5g/kg/min)aftera loadingdoseof1g/kg,another30patientsweregivenonly physiological saline infusions. The authors demonstrated that the group that received esmolol infusion during the postoperativeperiodrequired lesseramounts offentanyl. Koppertetal.19analyzedtheeffectsofperioperative
lido-caineinfusioninmajorabdominalsurgeriesandfoundthat, inpatientswhohadreceivedlidocaineinfusionatarateof 1.5mg/kg/hfollowing a loading dose of 1.5mg/kg 30min beforesurgicalincisionuptotheendofsurgerydemanded fewernumbers ofPCAandlessmorphineadministeredvia PCA,andthetotalconsumptionofmorphinewasrelatively lowercompared withthe control group. In ourstudy, we found no difference between groups in the time to the firstrequirementforananalgesic,thenumberofdemands forPCA, andtheamount of fentanyldeliveredbyPCA. In bothgroups,eventhoughthetotalamountofpostoperative opioid consumption wasnearly equal, we detected lower requirementsforadditionalanalgesicsinpatientswhohad receivedlidocaineinfusion.Earlypostoperativerestingand dynamicVASscoresintheesmololgroupwerecomparatively lower,butinthelongterm,theVASscoresdeterminedinall measurement periodsdid not differ between the esmolol andlidocainegroups.Ithasbeenrecognizedthatthe intra-venousadministrationof sodiumchannel blockerssuch as lidocainehasantinociceptiveeffectsviaitsimpactondorsal spinalhornneurons.22However,somestudieshaverevealed
that esmolol decreased the requirement for anesthetic agentsandensuredrapidrecoveryfromanesthesiathrough itsdepressiveeffectsonthecentralnervoussystem.11,16,20
Sympathomietic drugs acting on the central nervous sys-tem are known to alter the need for anesthetic agents. The detectionof lower VASscores at 10 and 20min after extubationcanbeexplainedbytheantagonisticeffectsof esmololoncatecholaminesynthesisinthebrainandspinal cord.
Nauseaand vomiting,residual effectsof anesthetic drugs andopioids,andgastricdistensionmightbecomeapparent withambulationandhypotension.23Opioidscaninduce
nau-seaandvomitingnotonlybystimulatingthechemoreceptor triggerzoneinthebrainstembutbydelayinggastric emp-tying and their hypotensive effects.23 In comparison with
theremifantilgroup,Colomaetal.12 detectedsignificantly
lowerincidenceofnauseaandvomitingintheesmololgroup undergoinglaparoscopicgynecologicsurgeries.Similarly,in astudyinvestigatingtheeffectsoflidocaineinlaparoscopic cholecystectomies,Lauwicketal.7observedlowerratesof
nauseaandvomiting relative tothecontrol group. Inour study,wealsonotedtreatment-requiringnauseaand vomi-ting withsimilar degrees of severity in the lidocaineand esmololgroups.
Conclusion
Wefoundthatintraoperativelidocaineandesmololinfusions inlaparoscopiccholecystectomiesexertcomparatively sim-ilar suppressive effects on hemodynamic responses to trachealintubationandsurgicalincision,andtheyarenot superiortoeachotherregardingtheneedforintraoperative andpostoperativeopioidanalgesicsandthedevelopmentof sideeffects.Wealsonotedthatlidocaineinfusionwas com-parativelysuperior in the suppression of the response to trachealextubationandpostoperativeneed for additional analgesia; however, esmolol infusion was more advanta-geousregarding awakeningtime,earlypostoperative pain score,modified Aldreterecovery (MAS)score,andtimeto achieveaMASof9points.Inthecomparisonoftheefficacy ofthesetwoadjuvant agents,in varioustypesof surgery, wethinkthatfurthercontrolledstudiestoevaluatethe con-sumptionofanestheticagentsusingdifferentdrugdosages shouldbeconducted.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MinJH,ChaiHS,KimYH,etal.Attenuationofhemodynamic responsestolaryngoscopyandtrachealintubationduringrapid sequenceinduction: remifentanil vs. lidocaine with esmolol. MinervaAnestesiol.2010;76:188---92.
2.Cook TM, MacDougall-Davis SR. Complications and failure of airwaymanagement.BrJAnaesth.2012;109Suppl.1:i68---85.
3.Kaplan JD, Schuster DP. Physigolic consequencesof tracheal intubation.ClinChestMed.1991;12:425---32.
4.Benumof JL, Saidman LJ. Management of the airway complications.In:Anesthesiaandperioperativecomplications. 2nded.London:Mosby;1999.p.1---21.
5.CapuzzoM,VerriM,AlvisiR.Hemodynamicresponsesto laryn-goscopyandintubation:etiologicalorsymptomaticprevention? MinervaAnestesiol.2010;76:173---4.
6.WuCT,BorelCO,LeeMS,etal.Theinteractioneffectof peri-operativecotreatmentwithdextromethorphanandintravenous lidocaineonpainreliefandrecoveryofbowelfunctionafter laparoscopiccholecystectomy.AnesthAnalg.2005;100:448---53.
7.LauwickS,KimDJ,MichelagnoliG,etal.Intraoperative infu-sionoflidocainereducespostoperativefentanylrequirements in patients undergoing laparoscopic cholecystectomy. Can J Anesth.2008;55:754---60.
8.MenigauxC,GuignardB,AdamF,etal.Esmololprevents move-mentandattenuatestheBISresponsetoorotrachealintubation. BrJAnaesth.2002;89:857---62.
9.Tas¸yuz T, Topc¸u I, Ozaslan S, et al. Effects of esmolol on hemodynamicresponsestolaryngoscopyandtracheal intuba-tionindiabeticversusnon-diabetic patients.TurkJMedSci. 2007;37:289---96.
10.WiestDB,HaneyJS.Clinicalpharmacokineticsandtherapeutic efficacyofesmolol.ClinPharmacokinet.2012;51:347---56.
11.CollardV,MistralettiG,TaqiA, etal.Intraoperativeesmolol infusionintheabsenceofopioidssparespostoperativefentanyl inpatients undergoing ambulatory laparoscopic cholecystec-tomy.AnesthAnalg.2007;105:1255---62.
12.ColomaM, ChiuJW, White PF, et al. The useof esmolol as analternativetoremifentanylduringdesflurananesthesiafor fast-trackoutpatientgynecologiclaparoskopicsurgery.Anesth Analg.2001;92:352---7.
13.BisgaardT.Analgesictreatmentafterlaparoscopic cholecystec-tomy: acritical assessmentof theevidence. Anesthesiology. 2006;104:835---46.
14.WerawatganonT, CharuluxanananS. Patientcontrolled intra-venousopioidanalgesiaversus continuousepidural analgesia forpainafterintraabdominalsurgery.CochraneDatabaseSyst Rev.2013;28:CD004088.
15.ChiaYY,ChanMH,KoNH,etal.Roleof-blockadein anaesthe-siaandpostoperativepainmanagementafterhysterectomy.Br JAnaesth.2004;93:799---805.
16.WhitePF,WangB,TangJ,etal.Theeffectofintraoperative useofesmololand nicardipineonrecoveryafterambulatory surgery.AnesthAnalg.2003;97:1633---8.
17.TopcuI,OzturkT, TasyuzT,et al.Theeffects ofesmololon anestheticandanalgesicrequirement.TurkJAnaesthReanim. 2007;35:393---8.
18.Keskin E, Bilgin H. Comparing the effects of lidocaine and esmololforthecontrolofhemodynamicresponsesduring laryn-goscopy, intubation and extubation. TurkJ Anaesth Reanim. 2005;33:463---70.
19.KoppertW,WeigandM,NeumannF,etal.Perioperative intra-venouslidocainehaspreventiveeffectsonpostoperativepain and morphine consumption after major abdominal surgery. AnesthAnalg.2004;98:1050---5.
20.Smith I,Hemelrijck JV, White PF. Efficacyof esmolol versus alfentanilasasupplementtopropofol-nitrousoxideanesthesia. AnesthAnalg.1991;73:540---6.
21.OzturkT,KayaH,AranG,etal.Postoperativebeneficialeffects ofesmololintreatedhypertensivepatientsundergoing laparo-scopiccholecystectomy.BrJAnaesth.2008;100:211---4.
22.PypendopBH, Ilkiw JE. The effects ofintravenous lidocaine administrationontheminimumalveolarconcentrationof isoflu-raneincats.AnesthAnalg.2005;100:97---101.