232 volume 1 • issue 3 July / September 2011 • Abstract
The renin-angiotensin-aldosterone system (RAAS) is a hormonal system which contributes to the regulation of both arterial pressure and extra cellular fluids volume. The increase of RAAS, especially at angiotensin II (Ang II) level, affects the target organs and increases the risk of cardio-vascular issues, by increasing arterial pressure and through the direct effect of Ang II upon the vascular en-dothelium and the renal and cardiac tissue. Ang II re-duces the renal capacity of sodium excretion and initiates a set of events which increase arterial pressure. Increase of arterial pressure is necessary for re-establishing so-dium excretion, being realized by the pressure-natriure-sis relationship. Arterial hypertension affects the target organs (heart, kidneys) and leads to a vicious circle which contributes to maintaining a high arterial pressure.
Materials and Method: Male Wistar rats subjected on a normal diet, received either a sham operation (n=9) or continuous angiotensin II (Ang II) infusion (300ng/kgc/ min) subcutaneously, via mini pumps. Water ingestion and systolic blood pressure were measured for 14 days, after which the animals were sacrificed under anesthesia with ketamin, and the xylasin body weight, water inges-tion, heart mass, right and left ventricular mass, right and left kidney mass were measured.
Results: After 14 days of Ang II infusion, bodily weight decreased, systolic blood pressure increased, heart and left ventricular mass indexed to body weight were significantly enhanced compared with the sham group, and kidneys mass indexed to body weight was similar in the two groups.
Keywords: angiotensin II, hypertension, heart, kidney
INTRODUCTION
Traditionally, the renin-angiotensin complex is a circulating hormonal system in which the final and bioactive result, Ang II, is produced by two important enzymes, renin and the angi-otensin-converting enzyme (ACE) (1). RAS is a complex hormonal system with paracrine,
HEMODYNAMIC AND STRUCTURAL MODIFICATIONS IN
CONTINUOUS INFUSION WITH ANGIOTENSIN. II. AN EXPERIMENTAL
STUDY
Minela Aida Maranduca1, Elena Cojocaru2, P. Plamadeala3 Doina Mihaila,4 E. Carasevici5
1. Assist. Prof.,Dept. Physiology, Faculty Medicine,“Gr. T. Popa” U.M.Ph. Iasi 2. Assist. Prof.,Dept.Histology, Faculty Medicine, “Gr. T. Popa” U.M.Ph. Iasi 3. Lector, Dept. Pathology, “Apollonia” University Iasi
4. Senior Pathologist, “Sf. Maria” Children Hospital Iasi
5. Prof. Dr., Dept.Immunology, Faculty Medicine,“Gr. T. Popa” U.M.Ph. Iasi Corresponding author: [email protected]
autocrine and intracrine properties. Angio-tensines are formed by the action of renin over its specific sub-layer, the angiotensinogen, through a series of enzymatic reactions. Renin, the glycosylated carboxopeptidasis released from renal juxtaglomerular cells, acts upon the angiotensinogen (a proteic macro-molecular complex produced by hepatoctes) and forms Ang I (decapetid, apparently inactive). Ang I is transformed into a biologically-active principle, Ang II (8 amino-acids), by the action of a glyco-protein released by the pulmonary tissue, the angiotensin-converting enzyme. Recently, a novel enzyme similar to ACE, called ACE2, has been identified in the heart, kidney, liver and intestine. ACE2 is a monocarboxypeptidase which generates Ang (1-9) from Ang I and Ang (1-7) from Ang II (2). ACE2 has a role on both degradation of Ang II, a peptide with vasocon-strictor effect, and production of Ang (1-7), which is a vasodilatatory peptide. Moreover, Ang (1-7) antagonizes the cell signals mediated by Ang II and restricts in this case the effects of Ang II. This approach may be considered as an anti-regulation mechanism of the classical RAS. Ang II can be also generated from Ang I, by the action a great number of peptidases, named chemises (alternative pathways for the genera-tion of Ang II) (3). Like other peptide hormones, to perform their actions, angiotensines bind to the membrane receptors of target cells (angio-tensinic type 1 receptors – AT1 and type 2 – AT2). Classically, the most important function of RAS is to maintain arterial pressure through vasocon-striction induced by Ang II and retention of
so-Medical interventions
International Journal of Medical Dentistry 233 dium mediated by aldosteron into the renal
col-lecting tube (4).
Local RAS, which acts independently on the systemic RAS, has been described (5). A com-plete delimitation of the systemic and local con-tribution of angiotensinic peptides is difficult to be done in terms of the actual experiments. Every system within a body contains elements of RAS.
MATERIALS AND METHOD
All protocols were reviewed and approved by the Institutional Animal Care and Use Com-mittee at the “Gr.T. Popa”University of Medi-cine and Pharmacy, Iasi. Male Wistar rats (~ 250g, Cantacuzino Institute, Bucuresti), maintained on a normal diet, received either a sham operation (n=9) (sham rats underwent identical surgical and implantation procedures) or continuous Ang II infusion (300ng/kgc/min) subcutane-ously, via mini-pumps (Alzet). The mini-pump was implanted subcutaneously at the dorsum of the neck. The rats were maintained on a 12h/ 12h light/dark cycle, being monitored up to 14 days of Ang II infusion, with free access to a regular diet and water. Systolic blood pressure (BP) was measured in conscious rats using tail-cuff plethysmography every 3 days. During the 14 days of the experiment, water ingestion was also measured. Bodily weight was measured ini-tially and after 14 days.
The animals were sacrificed under anesthesia with ketamin and xylazin. Using a mild-abdomi-nal incision, the heart, right and left ventricle, and the right and left kidney were cut and meas-ured.
The results are expressed as mean ± SEM. Comparisons within groups were performed using paired Student’s t-test. Statistical signifi-cance was accepted for p=0.05.
RESULTS AND DISCUSSION
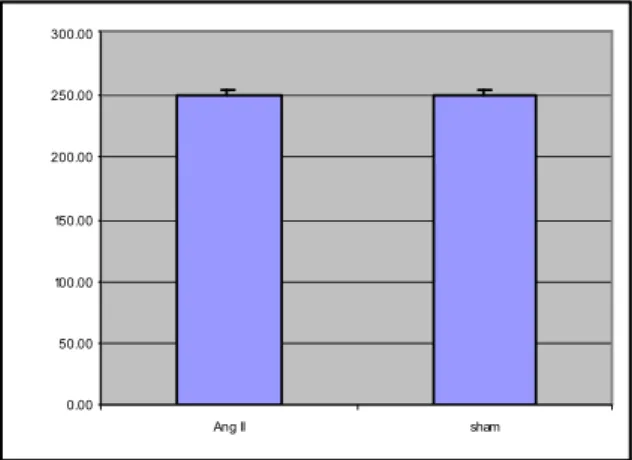
Before the treatments, bodily weight was similar in the two groups (Fig. 1A). Chronic Ang II infusion in rats, which significantly decreases
bodily weight (p<0.05) (Fig. 1B), may be due to increased peripheral metabolism.
0.00 50.00 100.00 150.00 200.00 250.00 300.00
Ang II sham
Fig. 1A. Initial bodily weight
275. 00 280. 00 285. 00 290. 00 295. 00 300. 00 305. 00 310. 00
A ng I I s h am
Fig. 1B. Bodily weight after 14 days
Ingestion of water progressively and signifi-cantly increased, p<0.05, in rats with Ang II chronic infusion (Fig.2).
0 5 10 15 20 25 30 35
1 2 3 4 5 6
W
a
te
r
in
g
e
s
ti
o
n
,
m
l
Ang II
Sham
Fig. 2. Ingestion of water
234 volume 1 • issue 3 July / September 2011 • Before the treatments, systolic BP was similar
in the two groups. However, systolic BP pro-gressively and significantly increased in rats with Ang II chronic infusion (Fig.3)
0 50 100 150 200 250
1 2 3 4 5 6
S
ys
to
li
c
B
P
,
m
m
H
g
Ang II Sham
Fig. 3. Systolic BP
Heart mass versus bodily weight (cardiac index)
Chronic Ang II infusion in rats significantly increased the heart mass versus bodily weight (p<0.05) (Fig.4). The role of angiotensin II on the heart is not limited to vasoconstriction. Ang II has also cardiovascular and non-cardiovascular effects. Angiotensin II not only stimulates con-traction, but also enhances growth and extra cel-lular matrix deposition (particularly collagen and fibronectin), and stimulates apoptosis and the production of cytokines (6).
0.0 0 0.0 5 0.1 0 0.1 5 0.2 0 0.2 5 0.3 0 0.3 5 0.4 0
Ang I I Sham
Fig. 4. Heart mass versus bodily weight
Ang II promotes cardiac hypertrophy via paracrine release of TGF-ß and endothelin-1 fibroblasts in a neonatal rat cell culture model (7).
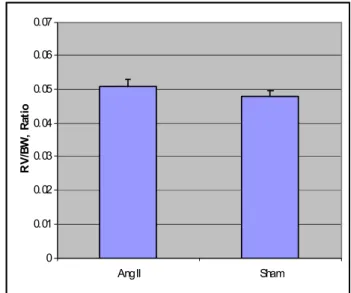
Right ventricle mass versus bodily weight
Right ventricle mass versus bodily weight was similar in the two groups after 14 days (Fig.5).
0 0.01 0.02 0.03 0.04 0.05 0.06 0.07
Ang II Sham
R
V
/B
W
,
R
a
ti
o
Fig. 5. Right ventricle mass versus bodily weight
Left ventricle mass versus bodily weight
As demonstrated in Fig. 6, chronic Ang II in-fusion significantly increased the left ventricle mass versus bodily weight. In patients with hy-pertension, one of the early and most common consequences of chronic hypertension is left ven-tricular hypertrophy (LVH), while the presence of LVH is associated with significant cardiovas-cular risk (8, 9). Clinical evidence suggests that RAS contributes to the development of LVH in hypertension (10-12). In addition, clinical
stud-0.00 0.05 0.10 0.15 0.20 0.25 0.30
Ang II Sham
Fig. 6. Left ventricle mass versus bodily weight Minela Aida Maranduca, Elena Cojocaru, P. Plamadeala, Doina Mihaila, E. Carasevici
International Journal of Medical Dentistry 235 ies demonstrated that the actions of ACE
inhibi-tors and ARBs cause regression of LVH more effectively then other classes of antihypertensive agents with similar levels of blood pressure con-trol (10-12).
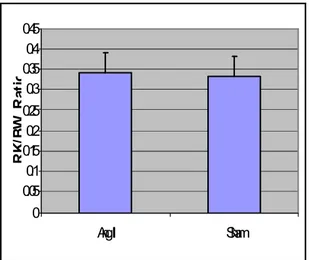
Right kidney mass and left kidney mass
Figure 7A and 7B demonstrates that the right kidneys mass versus bodily weight was similar in the two groups after 14 days.
0 0.05 0.1 0.15 0.2 0.25 0.3 0.35 0.4 0.45
Ang II Sham
R
K
/B
W
,
R
a
ti
o
Fig. 7A. Right kidney mass versus bodily weight
0 0.1 0.2 0.3 0.4 0.5
Ang II Sham
L
K
/B
W
,
R
a
ti
o
Fig. 7B. Left kidney mass versus bodily weight
CONCLUSIONS
In our experiments, rats with Ang II infusions developed LVH, which was the effect of hyper-tension. The hypertension issues activate the ren-nin angiotensin system (angiotensin II). Ang II
has a direct effect on the structure/function of kidney and heart, their excessive affection lead-ing to renal and heart injury.
References
1. John E. Hall. The Kidney, Hypertension, and Obesity.Hypertension.2003;419( 2):625-633. 2. Ion Haulica, Walther Bild, Dragomir N Serban .
An-giotensin Peptides and their Pleiotropic Actions Journal of Renin-Angiotensin-Aldosterone Sys-tem; 2005;6(3):121-131
3. Monteiro de Resende and Jose Geraldo Mill. Alterna-tive AngiotensinII – Forming Pathways and Their Importance in Physiological or Physiopathologi-cal Conditions. Arq Bras Cardiol.2002;78(4):432-8 4. Paola Cassis, Giuseppe Remuzzi. Angiotensin II revis-ited: new roles in inflammation, immunology and aging.Embo Molecular Medicine.2010;2:247-257. 5. Rosendorff C. The renin-angiotensin system and vas-cular hypertrophy. J Am Coll Cardiol. 1996; 28:803–812.
6. Mary O. Graya, Carlin S. Longa, Judith E. Kalinyakb, Hong-Tai Lia, Joel S. Karline.Angiotensin II stimu-lates cardiac myocyte hypertrophy via paracrine release of TGF-b and endothelin-1 from fibroblasts. Cardiovascular Research 1998; 40:352–363 7. Ernesto L. Schiffrin and Rhian M. Touyz.Multiple
actions of angiotensin II in hypertension benefits of AT1 receptor blockade.J Am Coll Cardiol.2003; 42:911-913
8. Koren MJ, Devereux RB, Casale PN, Savage DD, Laragh JH. Relation of left ventricular mass and geometry to morbidity and mortality in uncom-plicated essential hypertension Ann Intern Med. 1991;114:345–352
9. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardio-graphically determined left ventricular mass in the Framingham Heart Study N Engl J Med. 1990;322:1561–1566
10. Schmieder RE, Martus P, Klingbeil A. J Am Med Assoc. 1996;275:1507–1513.
11. Mathew J, Sleight P, Lonn E, Johnstone D, Pogue J, Yi Q, Bosch J, Sussex B, Probstfield J, Yusuf S. Reversal of left ventricular hypertrophy in essential hyper-tension. A meta-analysis of randomized double-blind studies. Circulation. 2001;104:1615–1621. 12. Devereux RB, Dahlof B, Gerdts E, Boman K, Nieminen
MS, Papademetriou V, Rokkedal J, Harris KE, Edelman JM, Wachtell K. Reduction of Cardio-vascular Risk by Regression of Electrocardio-graphic Markers of Left Ventricular Hypertrophy by the Angiotensin-Converting Enzyme Inhibi-tor Ramipril Circulation. 2004;110:1456–1462. HEMODYNAMIC AND STRUCTURAL MODIFICATIONS IN CONTINUOUS INFUSION WITH ANGIOTENSIN. II.