Sexual function after anterior vaginal wall prolapse surgery
Texto
Imagem

Documentos relacionados
Introduction and hypothesis Little information is available on the recurrent coexistence of pelvic organ prolapse (POP), urinary (UI) and/or anal (AI) incontinence and
The aim of this study was to evaluate defecatory dysfunction, fecal incontinence, and quality of life as assessed by standardized questionnaires in relation to presence of
Quando escrevo as duas cartas partindo de dois certificados de cursos de formação que fiz que foram, de fato, cursos em que as discussões partiram da escola, dos problemas que
O estudo bibliográfico nos pro- porcionou condições para construirmos um aporte teórico sobre o sen do social da educação escolar, as especifi cidades da profi ssão docente,
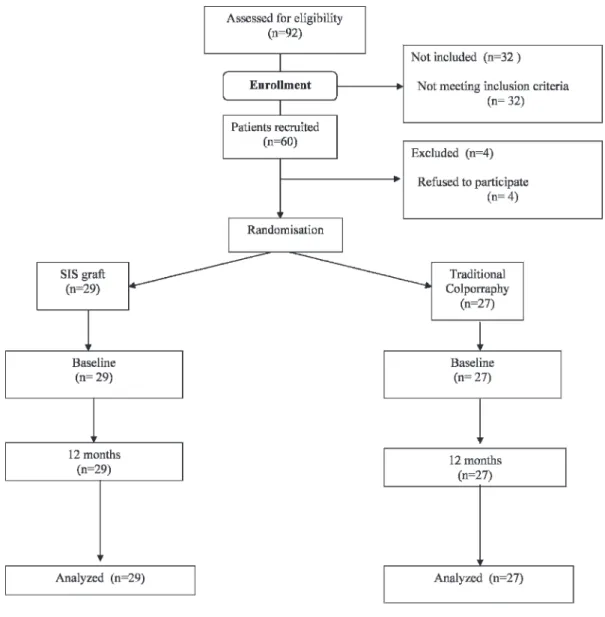
Materials and Methods: A total of 30 female patients with stress urinary incontinence (SUI), anterior and posterior vaginal wall prolapse, or both underwent surgical repair
FDA Public Health Notification: Serious complications associated with transvaginal placement of surgical mesh in repair of pelvic organ prolapse and stress urinary incontinence
Inclusion criteria were symptomatic primary or recurrent anterior and/or apical com- partment prolapse stage 3 or greater, according to pelvic organ prolapse quantitative
O patrimônio espeleológico, por sua vez, amparado inicialmente pela Constituição Federal em seus artigos 20, inciso X, e 216, inciso V, teve sua regulamentação por meio do
