The
Brazilian
Journal
of
INFECTIOUS
DISEASES
w w w . e l s e v i e r . c o m / l o c a t e / b j i d
Original
article
Pharmacodynamic
profiling
of
commonly
prescribed
antimicrobial
drugs
against
Escherichia
coli
isolates
from
urinary
tract
Gabriel
Trova
Cuba
∗,
Antonio
Carlos
Campos
Pignatari,
Katya
Silva
Patekoski,
Lucimila
Jorge
Luchesi,
Carlos
Roberto
Veiga
Kiffer
LaboratórioEspecialdeMicrobiologiaClínica,DepartmentofInfectology,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP, Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16August2013 Accepted23January2014 Availableonline13April2014
Keywords:
Pharmacodynamics MonteCarlomethod Escherichiacoli Urinarytractinfection
a
b
s
t
r
a
c
t
Sinceantimicrobialresistanceamonguropathogensagainstcurrentfirstlineagentshas affectedthemanagementofsevereurinarytractinfection,wedeterminedthelikelihood thatantibiotic regimensachieve bactericidalpharmacodynamicexposuresusingMonte Carlosimulationforfiveantimicrobials(ciprofloxacin,ceftriaxone,piperacillin/tazobactam, ertapenem,andmeropenem)commonlyprescribedasinitialempiricaltreatmentof inpa-tients with severe community acquired urinary tract infections. Minimum inhibitory concentrationdeterminationbyEtestwasperformedfor205Braziliancommunityurinary tractinfectionEscherichiacolistrainsfrom2008to2012and74E.colibloodstreamstrains recoveredfromasurveillancestudy.Pharmacodynamicexposurewasmodeledviaa5000 subjectMonteCarlosimulation.Allisolatesweresusceptibletoertapenemandmeropenem. Piperacillin/tazobactam,ceftriaxoneandciprofloxacinshowed100%,97.5%and83.3% sus-ceptibilityamongoutpatientisolatesand98.6%,75.7%and64.3%amonginpatientisolates, respectively.Againstoutpatientisolates,alldrugsexceptciprofloxacin(82.7%inaggressive and77.6%inconservativescenarios)achievedhighcumulativefractionofresponse: car-bapenemsandpiperacillin/tazobactamcumulativefractionofresponseswerecloseto100%, andceftriaxonecumulativefractionofresponsewas97.5%.Similarresultswereobserved againstinpatientsisolatesforcarbapenems(100%)and piperacillin/tazobactam(98.4%), whereasceftriaxoneachievedonly76.9%bactericidalcumulativefractionofresponseand ciprofloxacin61.9% (aggressivescenario)and56.7% (conservativescenario)respectively. Basedonthismodel,standarddosesofbeta-lactamswerepredictedtodeliversufficient pharmacodynamicexposureforoutpatients.However,ceftriaxoneshouldbeavoidedfor inpatientsandciprofloxacinempiricalprescriptionshouldbeavoidedinbothinpatients andoutpatientswithcomplicatedurinarytractinfection.
©2014ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mailaddress:[email protected](G.T.Cuba).
http://dx.doi.org/10.1016/j.bjid.2014.01.008
Introduction
Urinarytract infection(UTI) isthe mostcommonbacterial infectionandacutepyelonephritisisasevereformofUTIwith symptomsthatrangefrommilddiscomforttolifethreatening illness or death.1,2 The incidence of pyelonephritis requir-inghospitalizationis3–4casesper10,000populationamong womenand1–2casesper10,000populationamongmen,with anestimation ofdirectandindirect costsofUS$2.1billion andinhospitalmortalityof7.3per1000hospitalizationsfor femalesand16.5 per1000formales.2–4 Thebacteriologyof pyelonephritisissimilar tothe other UTIs, themajority of thembeingcausedbyEscherichiacoli.3,5
Themanagement ofUTIs isusuallyempirical,basedon thepredictable spectrumofetiologicagents andtheir sus-ceptibilitypatterns.Due tothe emergence ofantimicrobial resistanceamonguropathogens,thesafetyandeffectiveness ofempirical therapyhave been affected.6 Recently,ex vivo pharmacodynamic(Pd)models(basedonMonte Carlo sim-ulation)havebeenusedtohelpdeterminethebestregimens ordosagesforaspecificpatientpopulation,byintegratingan agent’sinvitropotencydistribution(i.e.,minimuminhibitory concentrations[MICs])withthepharmacokinetic(Pk)profile ofadrug.7
Regional surveillance studies show that antimicrobial resistance against currently prescribed first line agents (trimethoprim/sulfamethoxazoleandciprofloxacin)for treat-mentofcommunityacquiredUTIsinBrazilisincreasing.8,9 Since the resistance patterns of E. coli strains caus-ing UTI vary considerably between regions and countries, specific treatment regimens based on local susceptibil-ity patterns are necessary.5,9 The aim of this study was to compare the pharmocodynamic profiles of five antimi-crobials(ciprofloxacin, ceftriaxone, piperacillin/tazobactam, ertapenemandmeropenem)commonlyprescribedasinitial empirical therapy in hospitals for the treatment of inpa-tientswithcommunityacquiredUTIs,usuallycomplicatedor pyelonephritis.
Materials
and
methods
Microbiology
Bacterialisolates
Thepresentstudyincludedatotalof279bacterialisolates;100 isolatesofoutpatientsstoredattheculturecollectionofthe SpecialLaboratoryofClinicalMicrobiology(LEMC)since2008, 105isolates ofoutpatientsprospectively collected between AugustandNovember2012,and74nosocomialisolatesfrom thefirstbacteremiaat16 hospitalsinBrazilparticipantsof theBrSCOPEstudy.10AllisolateswereidentifiedwiththeBD Phoenix 5.1TM (BectonDickinson, Sparks, MD 21152, USA) and/orbiochemicalidentificationmethods.Onlyoneisolate perpatientwasincludedinthestudy.
Minimalinhibitoryconcentration(MIC)testing
The MIC was determined by epsilometric test (Etest®, BioMérieux,Marcyl’Etoile,France)forertapenem(0.002–32),
meropenem (0.002–32), ciprofloxacin (0.002–32), ceftriaxone (0.016–256)andpiperacillin/tazobactam(0.016–256),following the recommendations ofthe manufacturer.Qualitycontrol wasperformedbytestingE.coliATCC25,922®andP.aeruginosa ATCC®27,853,withallresultswithinexpectedranges.
Samplesweresubculturedontobloodagarandthenonto MacConkey agar to ensure viability and purity. Individual colonieswerepickedfrom18to24hplatesandsuspendedin 0.85%salinetoaturbidityofa0.5McFarlandstandard.Cotton swabswereusedtotransfertheinoculumtotheplateswith MuellerHinton agar(Oxoid,Basingstoke, Inglaterra), which were driedbefore the Etest® strips were applied. For each strain, the fiveantibiotics were arranged ina singleplate. Plateswereincubatedfor18–24hat35◦C.Readingsand
inter-pretationswereperformedaccordingtoNationalCommittee forClinicalLaboratoryStandards(NCCLS).11
PkandPddata
Pkdata
Pkdatawereobtainedfrompreviouslypublishedstudiesin healthyvolunteers.12–14Forstudiestobeconsidered,theyhad to beconductedinatleast 10 healthy volunteers, describ-ing the assay used to determinedrug concentrations, and presentmeanandstandarddeviationresultsforthetotalbody clearanceinlitersperhour(CL),volumeofdistributionofthe centralcompartment(Vc)andotherpertinentPkparameters. Becausepublishedreportswiththeabovecharacteristicswere notidentifiedforpiperacillin/tazobactamandceftriaxone,Pk dataforthesedrugsweretakenfrompublishedstudies15,16in criticalpatients(nostudiesdescribingthecovariancematrix inhealthyvolunteers).ThePkdatawasthenusedintheMonte Carlosimulationmodels.A5000patientMonteCarlo simula-tion(OracleCrystalBallFusionEdition,2010)wasconductedto calculateestimatesoftheamountoftimeinwhichthefreeor non-protein-bounddrugconcentrationexceedstheMICofthe organism(fT>MIC)ortheAUC/MICratioforeachantibiotic regimen/bacterialpopulation combination.Thesimulations were conductedas previouslypublished.17,18 Drugdosages chosen were based on the following commonlyprescribed regimens,administeredas30-minintravenous(IV)infusions: ertapenem 1g every 24h (q24h), meropenem 1g every 8h (q8h),piperacillin/tazobactam4.5gevery8h(q8h),ceftriaxone 1gevery12h(q12h)andciprofloxacin400mgevery12h(q12h). Pdexposures,asmeasuredbyfT>MIC,weresimulatedforall beta-lactamregimensagainstallpathogengroups.Atwo com-partmentIVbolusequationwasusedtocalculate%fT>MIC forthebetalactams.Forciprofloxacin,thetotaldrugAUCwas calculatedasthedailydosedividedbythetotalbodyclearance (ClT).
Pdmodel
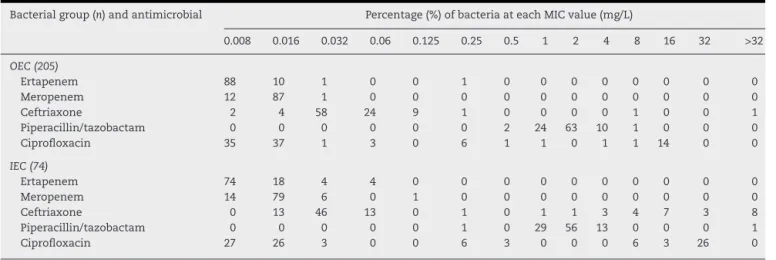
Table1–MICdistributionforoutpatientE.coli(OEC)andinpatientE.coli(IEC)includedinthisstudy.
Bacterialgroup(n)andantimicrobial Percentage(%)ofbacteriaateachMICvalue(mg/L)
0.008 0.016 0.032 0.06 0.125 0.25 0.5 1 2 4 8 16 32 >32
OEC(205)
Ertapenem 88 10 1 0 0 1 0 0 0 0 0 0 0 0
Meropenem 12 87 1 0 0 0 0 0 0 0 0 0 0 0
Ceftriaxone 2 4 58 24 9 1 0 0 0 0 1 0 0 1
Piperacillin/tazobactam 0 0 0 0 0 0 2 24 63 10 1 0 0 0 Ciprofloxacin 35 37 1 3 0 6 1 1 0 1 1 14 0 0
IEC(74)
Ertapenem 74 18 4 4 0 0 0 0 0 0 0 0 0 0
Meropenem 14 79 6 0 1 0 0 0 0 0 0 0 0 0
Ceftriaxone 0 13 46 13 0 1 0 1 1 3 4 7 3 8
Piperacillin/tazobactam 0 0 0 0 0 1 0 29 56 13 0 0 0 1 Ciprofloxacin 27 26 3 0 0 6 3 0 0 0 6 3 26 0
previouslyproposed as Pd thresholdfor UTI. Microbiologi-calcurewereachievedattainingacumulativefT>MICabove 30h.19 The probability for achieving a total AUC/MIC ratio greaterthanorequalto62.5,75,100,125,and150were cal-culatedforciprofloxacin.ThePdtarget ofAUC/MICatleast 62.5(conservativescenario,halfofthetargetforbloodstream infection)and125(aggressivescenario,similartothetarget forbloodstreaminfection)werechosenasaPdbreakpointfor ciprofloxacin.These probabilitiesoftarget attainmentwere appliedtotheMICdistributionsfortheabovepathogensto calculatethecumulativefractionofresponse(CFR).
Results
Invitroactivity
Table 1 summarizes the results of the in vitro
suscepti-bility testing. The resistance profile of outpatient isolates from2008to2012wassimilar.Allisolatesweresusceptible toertapenemandmeropenem(MICrange 0.008–0.25g/mL and MIC range 0.008–0.032g/mL, respectively); 100% of outpatient isolates (MIC range 0.5–8g/mL) and 98.6% of inpatient isolates (MIC range 0.25–256g/mL) showed sus-ceptibilitytopiperacillin/tazobactam.Higherresistancerates against ceftriaxone were observed for inpatient E. coli
(75.7%susceptibility,MICrange0.016–256g/mL)when com-pared to outpatient E. coli (97.5% susceptibility, MIC range 0.008–256g/mL).Amongtheantibioticstested,ciprofloxacin had the lowest susceptibility rates against the outpatient E.coli(83.3%,MICrange0.008–0.032g/mL)andinpatientE.coli (64.3%,MICrange0.008–32g/mL).
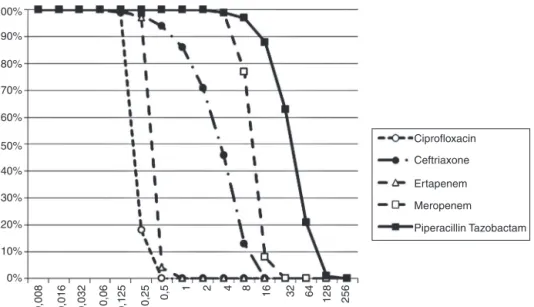
Pdtargetattainment
TheProbabilityofTargetAttainment(PTA)forbeta-lactams andciprofloxacinoverarangeofMICsisindicatedinFig.1. TheCFRsforeachbeta-lactamatvaryingtargetsfor%fT>MIC arelistedinTable2andtheCFRforciprofloxacinatAUC/MIC target of 62.5–150 is presented in Table 3. Carbapenems demonstrated high likelihood ofachieving the bactericidal breakpointof40%fT>MICandpiperacillin/tazobactamat50% fT>MICinbothscenarios.Incontrast,ceftriaxoneachieved a CFR superior to 95% only against outpatient isolates. CiprofloxacinhadpoorCFRagainstoutpatient(82.7%,77.6%) andinpatient(61.9%,56.7%)isolatesatthetargetexposureof totalAUC/MIC>62.5andAUC/MIC>125,respectively.
Considering a treatment duration of seven days, the cumulative fT>MIC superior to 30h was achieved at MIC concentration of 8g/mL for ceftriaxone, 8g/mL for meropenem, 1g/mL for ertapenem and 64g/mL for piperacillin/tazobactam.
Table2–Cumulativefractionofresponse(CFR)atvarying%fT>MICforbeta-lactamsagainstoutpatientE.coliand
inpatientE.coliisolatesfromBrazil.
Isolates(no.)/antimicrobial CFRatvarying%fT>MICexposures
20% 30% 40% 50% 60% 70% 80% 90% 100%
OutpatientE.coliisolates(205)
Ertapenem1gq24h 100% 100% 99.99% 99.75% 99.53% 99.51% 99.27% 98.42% 98.81% Meropenem1gq8h 100% 100% 100% 100% 100% 100% 100% 100% 100% Ceftriaxone1gq12h 98.03% 97.91% 97.72% 97.50% 96.09% 92.49% 86.64% 79.37% 74.24% Piperacillin/tazobactam4.5gq8h 100% 100% 99.99% 99.87% 98.87% 97.88% 95.27% 93.05% 90.11%
InpatientE.coliisolates(74)
100%
90%
80%
70%
60%
40% 50%
30%
20%
10%
Ciprofloxacin
Ceftriaxone
Ertapenem
Meropenem
Piperacillin Tazobactam
0%
0,008 0,016 0,032 0,06 0,125 0,25
0,5 1 2 4 8 16 32 64 128 256
Fig.1–ProbabilityofTargetAttainment(PTA)forbeta-lactamsandciprofloxacinoverminimuminhibitoryconcentration
(MIC).
Discussion
Increasing rates of resistance to antimicrobials commonly usedfortreatingUTIscausedbyE.coliamongoutpatientshas been reportedinrecent years.20 Inthis context,this study compared the antimicrobial susceptibility of community-acquiredUTIE.colistrainsbetweentwoperiods,sincelocal susceptibilitypatternsareessentialforappropriate antimicro-bialprescribing.Thestudyalsoincludednosocomialisolates fromthefirstbacteremiaepisode.Despitehighvariabilityin theorigin ofbacteremiareportedin theliterature,the uri-nary tract is one of the most frequent sources for E. coli bacteremia.21 For this reason, the authors considered the inclusionoftheseisolatesinthestudyasrelevant.
The sensitivity profile of outpatient E. coli was similar between 2008 and 2012. For ciprofloxacin, local surveil-lance studies on uropathogens in community-acquired infections9,22 also found decreased susceptibility pattern of outpatient E. coli, especially since the year 2000. Our present results are similar to those described locally by Rochaetal.,22 whichobtained82.2%inisolatesof2009.For otherantimicrobialstested,our studyshowedresults simi-lartotheSENTRYstudy:lowprevalenceofceftriaxoneand piperacillin/tazobactamresistanceandnoresistanceagainst carbapenems.9
The Monte Carlo Simulation has already been used to forecast the efficacy of different therapeutic regimens
in multiple scenarios, such as bloodstream infections, community-acquired pneumonia and ventilator-associated pneumonia.17,23,24Tothebestofourknowledge,ourstudyis thefirstreporttoapplytheMonteCarloSimulationevaluating thelikelihoodofachievingbactericidalPdtargetsinUTIs.
AsforthePdtargetsadopted,fewstudieshaveestablished specificPdthresholdsforUTI.Deguchietal.,25determinedthe Pdtargetoflevofloxacinformicrobiologicalcureinpatients withcomplicatedUTIbasedontheplasmaconcentrationof thedrugandthethresholdofAUC/MICforpredicting microbi-ologicalcurewaslowerthanthoseinotherkindofinfections. NostudiescorrelatingaPdtargetofciprofloxacinplasma concentration andmicrobiological cureforUTIwere found inourreview.Sinceciprofloxacinand levofloxacinare fluo-roquinolonesandtargetswithinantibioticclassestendtobe similar,weproposedthetwoscenariospreviouslydescribed: anaggressiveandaconservativeoneforciprofloxacin.
With respect to beta-lactam antibiotics, a cumulative fT>MICaround 30hwas correlated tomaximumcurerate forserumaminopenicillinconcentration.19Unfortunately,no study correlating microbiological cureforUTI and fT>MIC ratio for meropenem, ertapenem, piperacilin/tazobactam and ceftriaxone were found. Considering the target for aminopenicillinsimilartothe drugsincludedinthisstudy, those resultsmight not beapplicable on real lifescenario sincean 8g/mL MIC formeropenem and a64g/mL MIC for piperacillin/tazobactam would be considered interme-diate based on CLSI breakpoints, and a 16g/mL MIC for
Table3–Cumulativefractionofresponse(CFR)forvaryingtotalAUC:MICforciprofloxacin400mgq12hagainst outpatientE.coliandinpatientE.coliisolatesfromBrazil.
Isolates(no.) CFRatvaryingtotalAUC:MICexposures
62.5 75 100 125 150
OutpatientE.coli(205) 82.71% 82.32% 80.05% 77.63% 76.76%
ceftriaxone,resistant.Forrenaltissueinfection,theserumor plasmaconcentrationisausefulmarkerfortheantibiotic con-centrationsintherenaltissue.19AsPdtargetsforbeta-lactams insevereUTIarenotwellelucidated,forthepresent simu-lationweconsideredtheestablishedtargetsforbloodstream infections.
Initially,weestimatedthevariabilityforthePkparameters derivedfromhealthyvolunteers.Pkdatafromcriticalpatients werechosenforpiperacillin/tazobactamandceftriaxonedue toalackofpublishedreportswhichmettheinclusion crite-riaforourstudy.DeRykeetal.,18foundCFRlargelysimilar forpiperacillin/tazobactam whetherPkofpatientsorthose ofhealthyvolunteerswereused.Concerningceftriaxone,in spiteofaweakincreaseofVcandwideinter-patient variabil-ityobservedincriticalpatients,totalserumconcentrations weresimilartothatobservedinnormalpatients.26
Current recommendation advises not to prescribe ciprofloxacinasempiricaltreatmentforUTIiflocalresistance exceeds 10%.5 Surveillance studies had already demon-strated that ciprofloxacin resistance in Brazil overcomes suchpercentage.18,19Ourstudycorroboratesepidemiological findings,whichimpactsonalowprobabilityofachievinga bactericidalexposure(CFRof77.6%foroutpatientsand56.7% forinpatientsconsideringanAUC/MICtargetofatleast125). EveniflowerPdtargetswerechosen,CFRstayedconsistent (≤5%decreases).
BasedonthesimulatedPTAsciprofloxacinshouldbe pre-scribedonlywhenMICwasequalorbelow0.25g/mL,despite the susceptibility thresholdcurrently considered. Inconsis-tency between susceptibility and the predicted efficacy of antimicrobialshasalreadybeenreportedsinceCLSI-defined breakpointsforGramnegativebacillimightoverestimate sus-ceptibilityintwotofourfoldgreaterthanthoseestimatedby Pdsimulations.27
CeftriaxoneisagoodoptiontotreatsevereUTIinfectionin outpatientsbasedonoursimulations.Although dissemina-tionofclonesproducingESBLofcommunity-acquiredE.coli infectionswerealready reportedintercontinentally,8almost all outpatient isolates were susceptible to ceftriaxone. We observedahighpercentageofnon-susceptibilityagainst cef-triaxone (25.7%) in inpatientisolates, which decreases the probabilityofachieving bactericidal exposures(76.9%)with thisregimen.
Inthisanalysis, piperacillin/tazobactam,ertapenemand meropenemachievedthehighestCFRsinbothscenarios. Pre-viousPk/Pdstudiesalsofoundahighlikelihoodofachieving optimal Pd target exposure for meropenem against E. coli isolates.17,18,27
Similar to the derived result from Pd simulation of ciprofloxacin, ertapenem presented a fourfold discrepancy between CLSI defined breakpoint and those derived from stochastic determination. Althoughertapenem had similar invitroactivitytomeropenem,itsabilitytoachievehigh bac-tericidalPdexposurewilldependonthepresenceofahighly susceptiblepopulation,17whichwasreportedinthisstudy.
InspiteofhighCFRobservedinpresentstudy,lowerCFRsof piperacillin/tazobactamagainstE.coliisolateswaspreviously demonstrated.24Beta-lactam/beta-lactaminhibitor combina-tionisaneffectiveoptiontotreatESBL–E.colibloodstream infection originating from the urinary tract and should be
consideredareasonablealternativetocarbapenemsifactive invitro.21
Certainassumptionsaremadeforanalysesperformedwith MonteCarlosimulations.First,althoughtheresistancerates inourstudyweresimilartoprevioussurveillancestudies,it maynotreflectisolatefrequencyand/orsusceptibilitiesatall institutions.Second,weusedPkmodelsderivedfromhealthy andinfectedadultpatients,mostofwhomhadnormalrenal function.Doseadjustmentsmightbenecessarytoattain sim-ilar resultsforpatientswithrenalinsufficiencyorpediatric population.Finally,furtherstudiesare requiredtoelucidate thePdthresholdforciprofloxacinandbeta-lactamsnecessary toprovidemicrobiologicalcureinUTIs.
Onthebasisofthismodelusingmicrobiologydatafrom outpatientandinpatienturinaryisolates,standarddosesof beta-lactamswerepredictedtodeliversufficientPdexposure foroutpatients.Incontrast,thelowprobabilitypredictedfor ceftriaxonesuggeststhatthisdrugshouldnotbeprescribed inpatientswhohavehistoryofrecenthospitalization,early onsetofin-hospitalE.colibacteremiaorareinclose relation-shipwithhealthcareunits.Ciprofloxacinprescriptionshould bediscouragedevenincommunity-acquiredsevereITU.
Funding
This study was supported by Merck Sharp & Dohme. The pharmaceuticalcompanywasneitherinvolvednorhadany interferencewithdatacollection,interpretationoffindingsor preparationofthemanuscript.
Ethical
approval
ThisstudywasapprovedbytheEthicsCommitteeof Univer-sidadeFederaldeSãoPaulo(UNIFESP).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Thisstudywaspartiallypresentedasanabstractatthe23rd European Congress of Clinical Microbiology and Infectious Diseases,2013(abstract2872).
r
e
f
e
r
e
n
c
e
s
1.FoxmanB.Epidemiologyofurinarytractinfections:
incidence,morbidity,andeconomiccosts.AmJMed.2003;113
Suppl1A:5S–13S.
2.CzajaCA,ScholesD,HootonTM,StammWE.
Population-basedepidemiologicanalysisofacute
pyelonephritis.ClinInfectDis.2007;43:273–80.
3.BrownP,KiM,FoxmanB.Acutepyelonephritisamongadults:
costofillnessandconsiderationsfortheeconomic
4. FoxmanB,KlemstineKL,BrownP.AcutepyelonephritisinUS
hospitalsin1997:hospitalizationandin-hospitalmortality.
AnnEpidemiol.2003;13:144–50.
5. GuptaK,HootonTM,NaberKG,etal.Internationalclinical
practiceguidelinesforthetreatmentofacuteuncomplicated
cystitisandpyelonephritisinwomen:a2010updatebythe
InfectiousDiseasesSocietyofAmericaandtheEuropean
SocietyforMicrobiologyandInfectiousDiseases.ClinInfect
Dis.2011;52:e103–20.
6. GuptaK,HootonTM,StammWE.Increasingantimicrobial
resistanceandthemanagementofuncomplicated
community-acquiredurinarytractinfections.AnnIntern
Med.2001;135:41–50.
7. NicolauDP.Optimizingoutcomeswithantimicrobialtherapy
throughpharmacodynamicprofiling.JInfectChemother.
2003;9:292–6.
8. SchitoGC,NaberKG,BottoH,etal.TheARESCstudy:an
internationalsurveyontheantimicrobialresistanceof
pathogensinvolvedinuncomplicatedurinarytract
infections.IntJAntimicrobAgents.2009;34:407–13.
9. AndradeSS,SaderHS,JonesRN,PereiraAS,PignatariACC,
GalesAC.Increasedresistancetofirst-lineagentsamong
bacterialpathogensisolatedfromurinarytractinfectionsin
LatinAmerica:timeforlocalguidelines.MemInstOswaldo
Cruz.2006;101:741–8.
10.MarraAR,CamargoLFA,PignatariACC,etal.Nosocomial
bloodstreaminfectionsinBrazilianhospitals:analysisof
2,563casesfromaprospectivenationwidesurveillancestudy.
JClinMicrobiol.2011;49:1866–71.
11.ClinicalandLaboratoryStandardsInstitute(CLSI).2013
ClinicalandLaboratoryStandardsInstituteperformance
standardsforantimicrobialsusceptibilitytesting:23rd
informationalsupplement(M100-S23).Wayne,PA:CLSI;2013.
12.KlepserME,PatelKB,NicolauDP,QuintilianiR,Nightingale
CH.Comparisonofthebactericidalactivitiesofofloxacinand
ciprofloxacinaloneandincombinationwithceftazidimeand
piperacillinagainstclinicalstrainsofPseudomonas.
AntimicrobAgentsChemother.1995;39:2503–10.
13.WiskirchenDE,HousmanST,QuintilianiR,NicolauDP,Kuti
JL.Comparativepharmacokinetics,pharmacodynamics,and
tolerabilityofertapenem1gram/dayadministeredasarapid
5-minuteinfusionversusthestandard30-minuteinfusionin
healthyadultvolunteers.Pharmacotherapy.2013;33:266–74.
14.DreetzM,HamacherJ,EllerJ,etal.Serumbactericidal
activitiesandcomparativepharmacokineticsofmeropenem
andimipenem–cilastatin.AntimicrobAgentsChemother.
1996;40:105–9.
15.LodiseT,LomaestroB.Pharmacodynamicprofilingof
piperacillininthepresenceoftazobactaminpatients
throughtheuseofpopulationpharmacokineticmodelsand
MonteCarlo.AntimicrobAgentsChemother.2004;48:4718–24.
16.JoyntGM,LipmanJ,GomersallCD,YoungRJ,WongEL,GinT.
Thepharmacokineticsofonce-dailydosingofceftriaxonein
criticallyillpatients.JAntimicrobChemother.2001;47:
421–9.
17.KifferCRV,KutiJL,EagyeKJ,MendesC,NicolauDP.
Pharmacodynamicprofilingofimipenem,meropenemand
ertapenemagainstclinicalisolatesofextended-spectrum
beta-lactamase-producingEscherichiacoliandKlebsiellaspp.
fromBrazil.IntJAntimicrobAgents.2006;28:340–4.
18.DeRykeCA,KutiJL,NicolauDP.Pharmacodynamictarget
attainmentofsixbeta-lactamsandtwofluoroquinolones
againstPseudomonasaeruginosa,Acinetobacterbaumannii,
Escherichiacoli,andKlebsiellaspeciescollectedfromUnited
Statesintensivecareunitsin2004.Pharmacotherapy.
2007;27:333–42.
19.Frimodt-MøllerN.Correlationbetween
pharmacokinetic/pharmacodynamicparametersandefficacy
forantibioticsinthetreatmentofurinarytractinfection.IntJ
AntimicrobAgents.2002;19:546–53.
20.SanchezGV,MasterRN,KarlowskyJA,BordonJM.Invitro
antimicrobialresistanceofurinaryEscherichiacoliisolates
amongU.S.outpatientsfrom2000to2010.AntimicrobAgents
Chemother.2012;56:2181–3.
21.Rodríguez-Ba ˜noJ,NavarroMD,RetamarP,PicónE,PascualÁ.
-Lactam/-lactaminhibitorcombinationsforthetreatment
ofbacteremiaduetoextended-spectrum
-lactamase-producingEscherichiacoli:aposthocanalysisof
prospectivecohorts.ClinInfectDis.2012;54:167–74.
22.RochaJL,TuonFF,JohnsonJR.Sex,drugs,bugs,andage:
rationalselectionofempiricaltherapyforoutpatienturinary
tractinfectioninaneraofextensiveantimicrobialresistance.
BrazJInfectDis.2012;16:115–21.
23.KifferCR,PignatariAC.Pharmacodynamicevaluationof
commonlyprescribedoralantibioticsagainstrespiratory
bacterialpathogens.BMCInfectDis.2011;11:286.
24.KimA,KutiJL,NicolauDP.Probabilityofpharmacodynamic
targetattainmentwithstandardandprolonged-infusion
antibioticregimensforempirictherapyinadultswith
hospital-acquiredpneumonia.ClinTher.2009;31:2765–78.
25.DeguchiT,NakaneK,YasudaM,etal.Microbiological
outcomeofcomplicatedurinarytractinfectionstreatedwith
levofloxacin:apharmacokinetic/pharmacodynamicanalysis.
IntJAntimicrobAgents.2010;35:573–7.
26.GarotD,RespaudR,LanotteP,etal.Population
pharmacokineticsofceftriaxoneincriticallyillseptic
patients:areappraisal.BrJClinPharmacol.2011;72:
758–67.
27.DeRykeC,KutiJ,NicolauD.Reevaluationofcurrent
susceptibilitybreakpointsforGram-negativerodsbasedon
pharmacodynamicassessment.DiagnMicrobiolInfectDis.