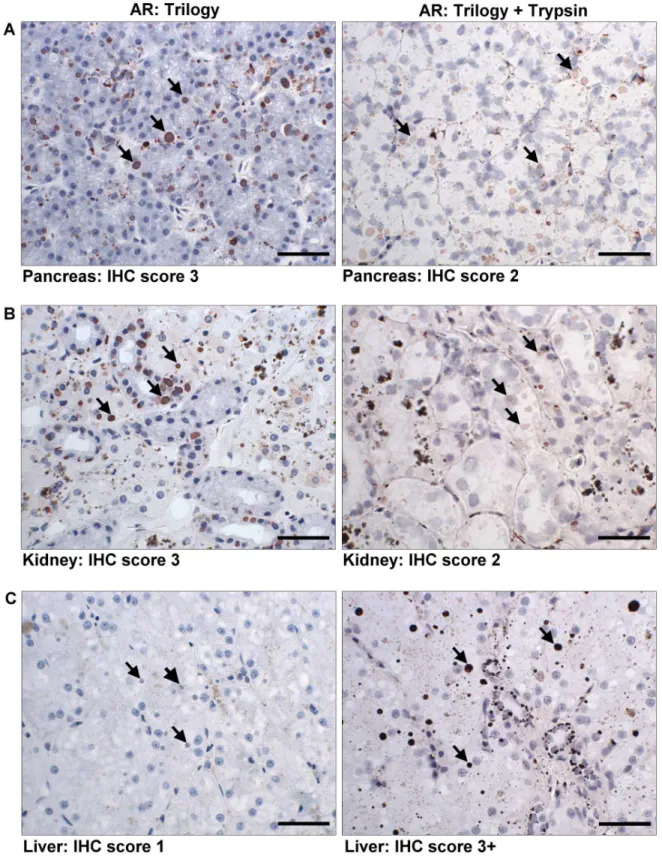
Immunohistochemical detection of a unique protein within cells of snakes having inclusion body disease, a world-wide disease seen in members of the families Boidae and Pythonidae.
Texto
Imagem
Documentos relacionados
Neste trabalho o objetivo central foi a ampliação e adequação do procedimento e programa computacional baseado no programa comercial MSC.PATRAN, para a geração automática de modelos
Ousasse apontar algumas hipóteses para a solução desse problema público a partir do exposto dos autores usados como base para fundamentação teórica, da análise dos dados
Peça de mão de alta rotação pneumática com sistema Push Button (botão para remoção de broca), podendo apresentar passagem dupla de ar e acoplamento para engate rápido
A justificativa para a utilização dos modelos de média móvel é pelo motivo dos mesmos serem aplicados quando na série não há ocorrência de sazonalidade,
Quando ligar um televisor Sony, a entrada pode ser seleccionada automaticamente carregando no botão de entrada após a configuração (Entrada SYNC) - avance para o passo 5.. 4
The fourth generation of sinkholes is connected with the older Đulin ponor-Medvedica cave system and collects the water which appears deeper in the cave as permanent
Despercebido: não visto, não notado, não observado, ignorado.. Não me passou despercebido
A proposta de oferta dos cursos Técnicos Integrados prevista para 2017 vem acompanhada da preocupação da comunidade do Campus Piracicaba em oferecer condições adequadas para o
