Abstract
Introduction: Auditory Steady State Response (ASSR) is an objective method for determining the auditive threshold, applicable and necessary especially in chil-dren. The test is extremely important for recommending cochlear implant in children. The aim of the study was to compare pure tone audiometry responses and auditory steady-state thresholds.
Materials and method: The study was performed on a group including both patients with normal hearing and with hearing loss. The main inclusion criteria accepted only patients with normal otomicroscopic aspect, normal tympanogram, capable to respond to pure tone audiom-etry, and with ear conduction thresholds between 0 and 80 dB NHL. The patients with suppurative otic processes or ear malformations were excluded. The research proto-col was followed, the tests being performed in sound-proofed rooms, starting with pure tone audiometry fol-lowed, after a pause, by ASSR determinations at frequencies of 0.5, 1.2 and 4 KHz. The audiological in-struments were provided by a single manufacturer. ASSR was recorded at least two times for both borderline intensities, namely the one defining the auditory thresh-old and the first no-response intensity. The recorded re-sponses were stored in a database and further processed in Excel. Discussion: The differences observed between pure tone audiometry and ASSR thresholds are impor-tant at 500 Hz and insignificant at the other frequencies. When approaching the PTA-ASSR relation, whatever the main characteristic between the PTA and ASSR thresh-olds in one ear, the profile of the lines gap maintains the same shape on the opposite ear. Conclusions: ASSR is a confident objective test, maintaining attention to low fre-quencies, where some differences might occur.
Keywords: Auditory Steady State Response (ASSR), pure tone audiometry, auditory thresholds
INTRODUCTION
Auditory Steady State Response (ASSR) is an audiological test used for the evaluation of audi-tive tonal thresholds, permitting plotting of a valid audiogram for patients who cannot or do not want to participate to classical audiometric tests (tonal audiometry), or for those incapable
VALIDATION OF THE ASSR TEST THROUGH COMPLEMENTARY
AUDIOLOGYICAL METHODS
C. Mâr]u1, Oana Manolache1, D. Rusu1, Raluca Olariu1, S. Cozma2
1. Ph.D. student, ENT, Clinical Recovery Hospital ,“Gr. T. Popa” U.M.Ph Ia[i 2. Lecturer, ENT Clinical Recovery Hospital “Gr. T. Popa” U.M.Ph Ia[i, Corresponding author: Cristian Mâr]u e-mail: [email protected]
The objective of the study was to validate the audiometric profile and the auditive thresholds obtained through ASSR, by comparative analy-sis with the subjective auditive thresholds ob-tained by tonal liminal audiometry in both chil-dren and adults.
MATERIALS AND METHOD
The study was developed in the Department of Audiology and Vestibulogy of the Clinical Recovery Hospital of Ia?i, the patients being se-lected from those who came to the ENT Clinic to treat the hearing loss they were suffering from. All patients were evaluated both otomicroscopically and tympanometrically, se-lected for the study being those with integer, normal tympan, the excluded ones being those with average otites or malformative anomalies. The total number of patients under analysis was of 7, which means 14 units of study (14 ears). Age represented one of the criteria for patients’ selection, so that those incapable of participating to tonal audiometry were excluded.
A protocol of the study was elaborated, in-volving realization of the tonal liminal audio-gram, followed, after some pause, by recording of the estimative audiogram by ASSR. For both audiological samples, a standard sound-proof room was used. ASSR was performed with the patient in decubitus position, as the test is a long-time one (2 hours, on the average), thus requir-ing a correspondrequir-ing muscular relaxation.
the establishment of the auditive threshold on frequencies of 500, 1000, 2000, 4000 Hz. Supra-aural phones were used. Stimulation was ob-tained with the warbled sound, testing first the high frequencies, followed by the low ones. Test-ing began at a frequency of 1000 Hz, endTest-ing at the same value. Of interest were only the tonal thresholds in aerial conduction, if considering their subsequent comparison with the thresholds estimated by ASSR (also obtained by aerial stimulation).
ASSR determinations were performed on the Eclipse (auditory evoked potentials system) Pro-duced by Interacoustics. Following the explana-tions given to the patient, the skin was cleaned with an abrasive conducting cream and 4 con-tact electrodes were mounted on the scalp, ac-cording to an ipsilateral FPZ – mastoide proce-dure. The tone-burst stimuli applied were presented by means of insert ear phones, at an initiation intensity of 65 dB HL. In a subsequent study, the stimulation intensity was either de-creased or inde-creased, from one case to another, up to the determination of thresholds on each frequency, while intrinsic intensity was checked twice, both for the accepted and the rejected stimulus. The curves were registered with a waiting time of 5 to 15 min on each frequency and intensity, which prolongued to a consider-able extent the test time, while increasing sig-nificantly the quality and precision of the test. The recordings were stocked in the data base and subsequently processed with the Excel pro-gram.
RESULTS AND DISCUSSION
The observation made during the ASSR tests was that the duration of recordings was shorter for mean and high frequencies and longer, re-spectively, for low frequencies, the testing time for each curve becoming longer and longer as the stimulation intensity gets close to the audi-tive threshold. The mean time given to each pa-tient included in the study exceeded 2 hours.
The age of the patients ranged between 6 and 60 years (fig. 1)
Fig. 1. Distribution according to age
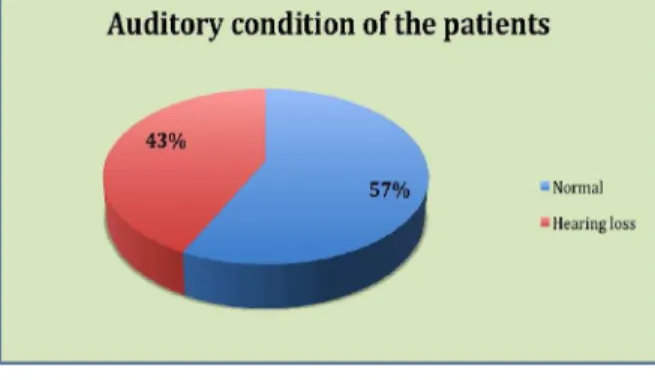
Fig. 2. Auditory condition of the patients under analysis
4 subjects presented liminal tonal auditive thresholds characteristic to normal hearing, while 3 of the tested patients suffered by hear loss (fig 2).
The individual results of the study are pre-sented by comparative graphical representation of the auditive thresholds obtained by the two methods, the subjective one, i.e. the tonal limi-nal audiogram, and the objective one, ASSR.
Comparison of the auditive thresholds for patient I shows a close relationship between the low and average frequencies, the only difference, of 10-15 dB, appearing at 4000 Hz. The audio-metric profile is similar left-right, for both ATL and ASSR (fig. 3).
Fig. 3. Comparative auditive thresholds ATL –ASSR for the study units 1 and 2
Fig. 4. Comparative auditive thresholds ATL –ASSR
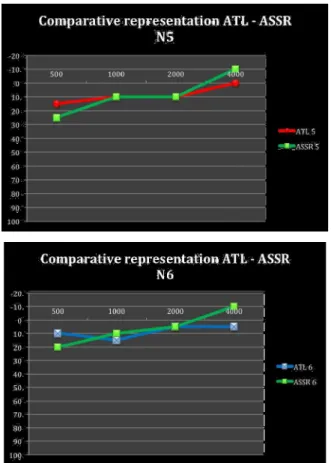
Fig. 5. Comparative auditive thresholds ATL –ASSR for the study units 5 and 6
In the case of patient (III), with normal hear-ing, a good relationship exists between the ATL and ASSR thresholds, on all frequencies, with a small difference of 10 dB in the extreme points, on 500 and, respectively, 4000 Hz. On both ears, at frequencies of 1000 and 2000 Hz, the ATL au-ditive thresholds are similar to the ASSR ones (fig. 5).
Fig. 6. Comparative auditive thresholds ATL –ASSR for the study units 7 and 8
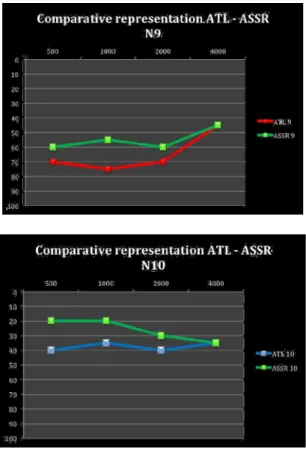
Fig. 7. Comparative auditive thresholds ATL –ASSR for the study units 9 and 10
Fig. 8. Comparative auditive thresholds ATL –ASSR for the study units 11 and 12
The case presented in Figure 8 evidences a significant discrepancy at a frequency of 500 Hz, even if, at the other frequencies, the ATL values are very close, being even overlapped with the ASSR ones (fig 8).
Fig. 9. Comparative auditive thresholds ATL –ASSR for the study units 11 and 12
Fig. 10. ASSR –ATL correspondence for frequency
Another objective of the study was to appre-ciate, for each frequency, the correspondence extent between the two auditive thresholds.
Figures 10 and 11 illustrate the ASSR-ATL relation between the values of the auditive thresholds obtained by the two methods.
The weakest relation between the subjective and objective audiometric thresholds (ASSR) occurs at a frequency value of 500 Hz, meaning that the objective threshold is frequently higher than the subjective one, which brings about an objective over-estimation of the real threshold.
However, on the other frequencies, the agree-ment is good, the closest subjective and objec-tive audiobjec-tive thresholds being obtained on 2000 and 4000 Hz.
Fig. 11. ASSR –ATL correspondence for frequency values of 2000 Hz and 4000 Hz
with the data published by other authors, since the apparition of ASSR up to now (1-3).
CONCLUSIONS
Establishment of the auditive thresholds by means of objective methods is especially impor-tant in the case of children who do not collabo-rate to tonal liminal audiometry, as well as for those with severe handicaps or in simulants.
Determination of the objective audiometric thresholds is especially important in the audi-tive recovery of babies or little children, as a timely intervention may assure a good auditive-verbal performance.
Auditory Steady State Response represents a modern objective method for the determination of the tonal auditive threshold, the absolute ad-vantage of which is the multifrequential re-sponse, its shortcoming being the long time it requires and the relaxation or sleep condition it assumes.
The differences observed, in the present study, between the ATL and ASSR thresholds are important for a frequency of 500 Hz, being insignificant for the other frequency values, and permitting, when indicated, a quite reliable au-ditive prosthesizing operation, meeting the needs of the child.
An important observation to be made is that, whichever the main characteristic of the ATL –
ASSR relation on one ear, the morphology of the ratio of the two curves is the same on the oppo-site ear, as well. Such a situation might suggest that, apart from the known parameters on which such differences depend, the ones for which the corrections had been already included in the measuring equipments, there also exists an ele-ment related to the individual structures, the presence of which explains why the same type of differences between the two types of audiograms appears on both ears.
To conclude with, ASSR represents an objec-tive and reliable method of audiobjec-tive testing, pay-ing special attention to low frequencies, where some discrepancies may occur.
References
1. Ozdek A., Karacay M., Saylam G., Tatar E., Aygener N. Comparison of pure tone audiometry and au-ditory steady-state responses in subjects with normal hearing and hearing loss. Eur Arch Otorhinolaryngol 2010; 267: 43–49
2. Ahn JH, Lee HS, Kim YJ, Yoon TH, Chung JW. Com-paring pure tone audiometry and auditory steady state response for the measurement of hearing loss. Otolaryngol Head Neck Surg 2007; 136: 966– 971