Brazilian
Journal
of
OTORHINOLARYNGOLOGY
www.bjorl.org
ORIGINAL
ARTICLE
Effects
of
the
reduction
of
caffeine
consumption
on
tinnitus
perception
夽
Ricardo
Rodrigues
Figueiredo
a,b,c,∗,
Marcelo
José
Abras
Rates
c,d,e,
Andréia
Aparecida
de
Azevedo
c,f,
Ronaldo
Kennedy
de
Paula
Moreira
g,
Norma
de
Oliveira
Penido
aaPost-GraduatePrograminOtorhynolaryngology,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil bFaculdadedeMedicinadeValenc¸a,RiodeJaneiro,RJ,Brazil
cTinnitusResearchInitiative,Regensburg,Germany
dUniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil eCentrodeTratamentoePesquisaemZumbido,BeloHorizonte,MG,Brazil fOtorrinolaringologiaSul-Fluminense(OTOSUL),VoltaRedonda,RJ,Brazil gSantaCasadeMisericórdiadeBeloHorizonte,BeloHorizonte,MG,Brazil
Received3September2013;accepted17November2013 Availableonline12June2014
KEYWORDS Tinnitus; Caffeine; Coffee
Abstract
Introduction:Formany years,excessivecaffeineconsumptionhasbeentoutedasan aggra-vatingfactor fortinnitus.The pathophysiologybehindthiseffectisprobablyrelatedtothe blockageofadenosinereceptorsbytheactionofcaffeineonthecentralnervoussystem.
Objective:Toevaluatetheeffectsofreductionofcoffeeconsumption ontinnitus sensation andtoidentifysubgroupsmorepronetobenefitfromthistherapeuticstrategy.
Studydesign:Prospective.
Methods:Twenty-sixtinnituspatientswhoconsumedatleast150mLofcoffeeperdaywere selected.Allwereaskedtoreducetheircoffeeconsumption.TheTinnitusHandicapInventory (THI)questionnairewascompletedby thepatientsbeforeandafterthereductionofcoffee consumption,aswellasavisual-analogscale(VAS)graduatedfrom1to10.
Results:THIandVASscoresweresignificantlyreduced(p<0.05).Inthesubgroupslessthan60 yearsold,bilateraltinnitusanddailycoffeeconsumptionbetween150and300mLshoweda significantlygreaterreductionofTHIandVASscores.
夽
Pleasecitethis articleas:Figueiredo RR, Rates MJ,deAzevedo AA, Moreira RK,PenidoNO. Effects ofthe reductionof caffeine consumptionontinnitusperception.BrazJOtorhinolaryngol.2014;80:416---21.
∗Correspondingauthor.
E-mail:[email protected](R.R.Figueiredo).
http://dx.doi.org/10.1016/j.bjorl.2014.05.033
1808-8694/©2014Associac¸ãoBrasileiradeOtorrinolaringologia eCirurgiaCérvico-Facial. PublishedbyElsevierEditoraLtda.All rights
Conclusion: Patientsunder60yearsofagewithbilateraltinnitusanddailycoffeeconsumption between 150and300mLaremorepronetobenefitfromconsumptionreduction. Thirty-day observationperiodsmaybehelpfulforabettertherapeuticaldecision.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Zumbido;
Cafeína; Café
Efeitosdareduc¸ãonoconsumodecafeínasobreapercepc¸ãodozumbido
Resumo
Introduc¸ão: Oconsumoabusivo decafeínavemsendodescritocomo fatordepiora ecausa dozumbidohámuitosanos.Afisiopatologiadesteefeitoestáprovavelmenterelacionadaao bloqueiodosreceptoresinibitóriosadenosínicospelacafeínanosistemanervosocentral.
Objetivo: Avaliarosefeitosdareduc¸ãodo consumode cafeínanapercepc¸ãodozumbidoe identificarsubgruposdepacientesmaispropensosabenefícioscomestaproposta.
Tipodeestudo:Prospectivo.
Métodos: Selecionados26pacientescomzumbidoneurossensorialeconsumodiáriosuperiora 150mLdecafé.Osefeitosdareduc¸ãodoconsumoforamavaliadosatravésdoTinnitusHandicap Inventory(THI)edaescalavisual-análoga(EVA).
Resultados: Houvereduc¸ãoestatisticamentesignificativa(p<0.05)nosescoresdoTHIeEVA. Nossubgruposcomidadeinferiora60anos,zumbidobilateraleconsumodiáriodecaféentre 150e300mLapresentarammaiorreduc¸ãodosescoresTHIeEVA.
Conclusão:Empacientescomidadeinferiora60anos,zumbidobilateraleconsumodiáriode caféentre150e300mLapresentarambenefícioscomareduc¸ãonoconsumodiáriodecafeína. Períodosobservacionaisde30diaspodemserúteisparaadecisãoterapêutica.
©2014Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
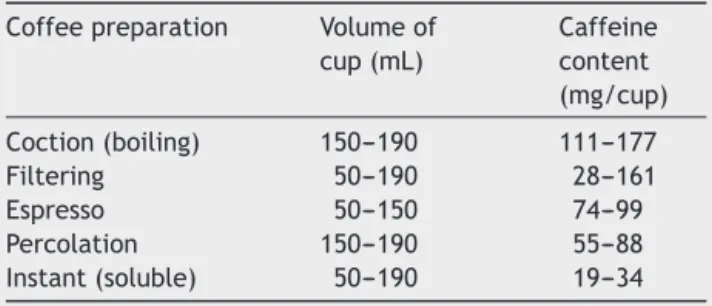
Caffeine,also knownasmethyltheobromin, is part of the groupofmethylxanthines,andisconsideredthemostwidely usedpsychoactivesubstanceintheworld.Themajorityof itsconsumptionisderivedfromdietarysourcessuchas cof-fee,tea,colasoftdrinks,andchocolate;themoststriking behavioral effects are increasesin alertness, energy, and concentration skills. These effects are more pronounced afteringestionofsmalltomoderateamounts(50---300mg).1 The caffeinecontent by coffee cup varies depends on theformofpreparation(Table1).1InBrazil,thepercapita consumption, according to the Associac¸ão Brasileira de IndústriasdoCafé(ABIC),is currentlyabout73Lperyear, andthefiltrationmethod ofpreparationisthemost com-monly used.2 A worldwide trend toward increased coffee consumptionhasbeennoted.Thecaffeinecontentofother beverages varies, on average, from 32 to 42mg/150mL (tea), 32 to70mg/330mL (cola beverages), and approxi-mately4mg/150mL(chocolateflavoredmilk).1
The absorptionof caffeineinthe gastrointestinaltract israpid,reaching99%after45min.Peakplasmalevelsare achievedbetween15and120minafteroralingestion,and thehalf-lifeisabout 2.5---4.5h.Caffeineismetabolizedby theliver.1
Currently, most authors believe that the main mecha-nismofaction ofcaffeineistheantagonismofadenosinic
receptors.1,3---5Adenosinereducesthefiringrateofneurons, exertingan inhibitoryeffect onsynaptictransmissionand inthe releaseof various neurotransmitters. In1993, Daly observed increased brain levels of norepinephrine, gluta-mate,andadrenalineaftercaffeineintake.3Theadenosinic receptorsinvolvedwiththeeffectsofcaffeineareA1and A2.Neurostimulanteffects of caffeinehave been demon-stratedinfunctionalimagingstudies.6
A2 adenosinic receptors interact with dopaminergic receptors in the nucleus striatum and nucleus accum-bens by modulating them. Therefore, the blockage of thesereceptors,exertedbycaffeine,couldpotentiatethe dopaminergicneurotransmission.1
Table 1 Amount of caffeine in various forms of coffee preparation.
Coffeepreparation Volumeof cup(mL)
Caffeine content (mg/cup)
Coction(boiling) 150---190 111---177 Filtering 50---190 28---161 Espresso 50---150 74---99 Percolation 150---190 55---88 Instant(soluble) 50---190 19---34
Otherdemonstratedactionsofcaffeineincludeincreased releaseof intracellularcalciumandinhibitionof phospho-diesterases;seemingly,thesemechanismsareunrelatedto thecentraleffectsofcaffeine.1
In addition to the neuroexcitatory effects, caffeine also has a vasoconstrictor effect, and this is the pre-dominant effect at higher doses.6 Studies with blood oxygenation level-dependant (BOLD) functional magnetic resonance imaging demonstrated a reduction in cerebral perfusionaftercaffeineintake.Some authorsbelievethat the neurostimulant effects of caffeine are due primarily toitsactiononA1receptors,whereasthevasoconstrictor effectsarerelatedtoitseffectsonA2receptors.6
Basedontheseneurostimulanteffectsofcaffeine, sev-eralstudiesaddressedtheeffectsofthissubstanceonthe centralauditory pathways.4---8 Loristetal. found improve-ment of the central auditory processing after caffeine intake5andKawamuraetal.6foundincreaseinthe ampli-tudeandareaofP300approximately30minaftercaffeine ingestion.
Dixit et al.4, also studying the effects of caffeine on P300,observed an increase in P3amplitude and reduced reactiontime,indicatingfacilitationofauditoryprocessing andaccelerationofmotorresponses.Inanotherstudy,the sameauthors found asignificant reductionin latencies of wavesIVandVinauditorybrainstempotentials(ABR),and asignificantdecreaseintheI---Vinterval.9
In the cochlea, it was demonstrated that caffeine inducedshorteningofouterhaircells (OHC).10---12 Thisfact wouldhavesomebearingontherapidcontractionofOHC, increasingtheexcitabilityoftheperipheralauditory path-waysThereisdisagreementabouttheeventsinvolvedinthis shortening. Slepecky et al.10, in a 1988 study, suggested thattheshorteningofOHCoccursbymechanismsassociated withrianodinicreceptors.Conversely,Yamamotoetal.11,in 1995,suggested thatOHC depolarizationoccursby potas-siumchannelblockage.Finally,Skellett etal.12,inastudy from1995,suggestedanosmoticmechanism.
Mostclinicalstudiesontheeffectsofcaffeinein otoneu-rologyrefertochangesinthevestibularsystem.13---15Several authors suggest a daily intake of up to three small cups (50mL) of filtered coffee asa beneficial practice for the treatment,andmayevenpotentiatethetherapeuticeffects ofsomemedications.15Abovethisdose,thevasoconstrictor effectswouldpredominate.
Withregardtotinnitus,severalauthorssuggestreducing theintake of caffeine asa supplementary treatment,16,17 butintheonlycontrolledstudyeverconducted,18beneficial effectsofcaffeinereductionontinnituswerenotobserved. Themainobjectiveofthisstudywastoassesswhether sen-sorineuraltinnituspatientscanobtainsomebenefitfromthe reductionofcaffeineintake.The secondaryobjectivewas totrytoidentifythe subgroupsof patientsmost likelyto benefitwiththisstrategy.
Methods
Thiswasacontemporarylongitudinalcohortstudy.The sam-plesizewasinitiallydeterminedconsideringassignificanta differenceof20pointsinTHI scoreandof2 pointsinVAS score(Fig.1)intheintervalfromthebeginningtotheendof
Visual analogue scale (VAS)
0
1
2
3
4
5
6
7
8
9
10
Figure1 VisualAnalogScale(VAS).
thestudy.Consideringastatisticalpowerof0.80,the min-imumsamplesizewassetat16patients(fordifferencesin THIscoresandVSAinferiorto20and2points,respectively, therequiredsamplesizewouldbeevensmaller).
Thisstudyincluded26patientswithsensorineural hear-ingloss,aged24---76yearsold,15males,treatedincenters participatinginthestudybetweenJanuary2008and Decem-ber2009.
Thefollowingcriteriawereused: Inclusioncriteria
• Patientswithtinnitusformorethansixmonths • Non-useofcentrallyactingdrugsinthelastsixmonths
• TympanogramtypeA-n
• Dailycoffeeintakeexceedingthreesmallcups/day (cor-respondingto150mL/day)
• Ageover18yearsold.
Exclusioncriteria:
• THI<16points
• Tinnitusofmuscularandvascularorigin
• Audiogramswithconductiveandmixedhearingloss
• Association with disorders of the temporomandibular joint.
At first visit, patients underwent a complete otorhi-nolaryngological exam. In the same consultation, tonal andvocalaudiometryandimitanciometrywereperformed. PatientsincludedinthestudycompletedtheTinnitus Hand-icap Inventory (THI), in itsversion validated for Brazilian Portuguese,19 andalsoquantifiedthetinnituswithrespect tothediscomfortandintensity,accordingtoaVisualAnalog Scale(VAS)gradedfrom1(minimalannoyance/intensity)to 10(maximumannoyance/intensity).
Table2 Generalcharacterizationofsample.
Characteristics Frequency
n %
Coffeeintake(mL)
≤300 9 40.9
>300 13 59.1
Age(years)
<60 12 54.5
≥60 10 45.5
Laterality
Bilateral 14 63.6
Unilateral 8 36.4
Aweeklycontactbyphonecallwasestablishedtoconfirm thereductionofconsumption.AnewreassessmentwithTHI andVASwasperformedafter30days,andallpatientswho did not achieve the aforementioned reduction goal were excluded.
The absolute change of the situation before/after the treatmentwasgivenbythefollowingformula:
THI/VSA=(finalTHI/VSA−initialTHI/VSA
AsthemaincriterionforreductionofTHI,thelevelofseven pointswasused,i.e.areductionofsevenpointsinthescore wasconsideredasanimprovement,accordingtothestudy byZemanetal.20Symptomsrelatedtocaffeinewithdrawal wereregistered.
Thestatisticalanalysisconsistedofthefollowingtests: Comparisons betweenthe characteristics and improve-ment of THI wereperformed usingFisher’sexact test (at leastoneexpectedfrequency<5).
Then. the adjustment of the logistic model containing thecharacteristicswithp-value<0.25wasperformed.Only those characteristics with p-value <0.05 remained in the finalmodel.Allinteractionsweretested.
Finally,theSpearmancorrelationcoefficientwasapplied toassessthedegreeofassociationbetweennumerical varia-blesandTHI/VAS.
Thecriterionfordeterminingthesignificancewassetat 5%. The statistical analysis wasperformed by SAS version 6.11(SASInstitute,Inc.---Cary,NorthCarolina),Rversion 2.7.1,and EpiInfoversion 6.04.The latter twoarepublic domainprograms.
The study was approved by the Ethics Committee for MedicalResearchunderCAAEnumber---0002.0.334.000-08.
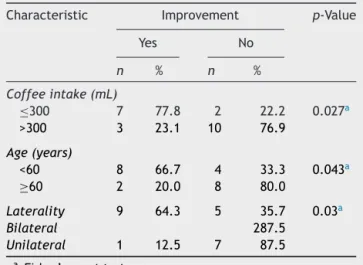
Table3 Descriptionofcoffeeintakelevels,age,and lat-eralityofthesample.
Characteristic Improvement p-Value
Yes No
n % n %
Coffeeintake(mL)
≤300 7 77.8 2 22.2 0.027a
>300 3 23.1 10 76.9
Age(years)
<60 8 66.7 4 33.3 0.043a
≥60 2 20.0 8 80.0
Laterality 9 64.3 5 35.7 0.03a
Bilateral 287.5
Unilateral 1 12.5 7 87.5
a Fisher’sexacttest.
Results
Ofthe26patientsinitiallyincluded,fourdidnotreturnfor thesecond evaluation. Table2 shows general dataof the sample,andTable 3liststhesubcategories distributionof the22patientswhocompletedthestudy.
Ofthe22patientswhocompletedthestudy,therewas improvement in the THI scores (reduction of at least 7 points)intenofthem(45.5%).Theobservedmeandecrease was10.2pointsforTHIand0.86pointsforVSA;bothwere statisticallysignificant (p=0.030and 0.017,respectively). Table4presentsthedescriptionofinitialandfinalTHIand thevariation(final−initial).
Table 5 shows the comparison of coffee intake, age, andlateralitywithimprovementof THI.Allfeatureswere selectedforinclusionintheinitialmultivariatemodel.
Interpretingoneoftheintersections,forinstance,among the nine patients who consumed up to 300mL of coffee perday,seven(77.8%)showedimprovementinTHI.Among the13patientswhoconsumedmorethan300mL/day,three (23.1%)showedimprovementinTHI.Withap-valueof0.027, thisfeaturewasselectedtobeincludedintheinitial multi-variatemodel.
Table6showstheadjustmentsoftheregressionmodels. Threelogisticregressionmodelswereelaborated.
Thus, itwas observed thatthose whoconsumed up to 300mLofcoffeehadapproximately12timesthechanceof improvementinTHIversuspatientswhoconsumemorethan 300mLofcoffee(95%CI:1.5---89.1).
In addition, patients younger than 60 years had eight timesthechanceofimprovementinTHIversusthoseaged
Table4 DescriptionofinitialandfinalTHI,andvariation(THI=finalTHI−initialTHI).
Characteristics n Mean SD Minimum 1stQ Median 3rdQ Maximum
THI,initial 22 46.6 19.9 16.0 27.0 51.0 63.0 78.0
THI,final 22 36.4 18.4 14.0 16.0 34.0 52.5 66.0
THIvariation 22 −10.2 19.4 −56.0 −19.0 −6.0 4.0 12.0
Table5 Comparisonbetweencoffeeintake,ageandlateralityandimprovementofTHIscores.
Variable n Mean SD Median Minimum Maximum
Age(years) 26 56.9 14.1 58.5 24 76
Tinnitustime(years) 26 6.44 6.30 5 0.5 20
Totalcoffeeintake/day(mL) 26 509.6 292.6 400 150 1200
THI,initial 26 48.8 21.9 53 16 100
VAS,initial 26 6.88 1.84 6.5 5 10
SD,standarddeviation.
Table6 Logisticregressionmodel.
Models Coefficient Standarderror p-Value OR 95%CI
Inferior Superior
ModelI
Constant −1.2 0.7 0.067
Coffeeintake(mL)
≤300 2.5 1.0 0.018 11.7 1.5 89.1
>300 1.0
ModelII
Constant −1.4 0.8 0.008
Age(years)
<60 2.1 1.0 0.038 8.0 1.1 56.8
≥60 1.0
ModelII
Constant −1.9 1.1 0.069
Laterality
Bilateral 2.5 1.2 0.036 12.6 1.2 133.9
Unilateral 1.0
OR,oddsratio.
over 60 years (95% CI 1.1---56.8). Patients with bilateral tinnitushadapproximately13timesthechanceof improve-mentin THI versus thosewithunilateral tinnitus (95% CI, 1.2---133.9).
Analyzingthequantitativevariable‘‘coffeeintake’’(in mL)bythe Spearmancoefficient relativetoTHI,Fig.2 wasobtained,confirmingpreviousdata(thehigherthe cof-feeintake,thelowertheobserveddecreaseinTHIandVAS). Ofthe22patientswhocompletedthestudy,onlyone(4.54%) showedasideeffect(anxiety),possiblyassociatedwiththe
80
60
40
20
–20
–40
–60
–80
–100
r1 = 0.581: p=0.005
Total daily coffee intake (mL)
Δ
TH
I
queda
aumento
0 100 200 300 400 500 600 700 800 900 10001100 12001300 0
Figure2 AnalysisofTHI,accordingtodailycoffeeintake (Spearmancoefficient).
caffeine reduction. This patient consumed an average of 1200mLofcoffeedaily.
Discussion
Severalarticlesontinnitushave recommendedthe reduc-tionofcaffeineconsumpion,16butuntilrecently,therewere nospecificstudiesonthissubject.Theoretically,the stimu-latingactionofcaffeineonthecentralnervoussystemcan playaroleintheexcitabilityoftheauditorypathwaysand, therefore,canmodifysomeclinicalaspectsoftinnitus.9
Inarecentstudy(2010)18,theeffectsoftheremovalof caffeineontinnitusin patientswhoconsumed >150mg of caffeinedailywereevaluated.Inthispseudo-randomized, crossed-over, placebo controlled study of 66 patients, no evidencetojustifyareductionincaffeineintakewasfound. Conversely, some side effects caused by withdrawal from caffeinewerenoted.Accordingtotheauthors,theseeffects couldalsoleadtoaworseningoftinnitus.
difficult, sincechroniccaffeineuserscan easily recognize the removalof this substance, regardless of theflavor of thebeverage.1
Despitethestatisticalsignificanceofdatafound inthis study(areductionof10.2pointsinTHIand0.86pointsin VAS),itwasobservedthattheeffectsofreducingcaffeine intakeonatinnituspopulationasawholewouldbesmall, accordingtothecriteriausedbyNewman,whichrequireas significantvariations≥20pointsforTHI.21Onlyfour(18.4%) of22patientsshowedsuchreduction.Conversely,thestudy byZemanetal.demonstratedthatdifferencesof6---7points in THI scores are clinically relevant.20 In this case, ten patients (45.5% of the total sample) of this study fit into thisprofile. Inthesubgroup analysis,itwasfound thatin subgroupswith<60years,bilateraltinnitus,andinitialdaily intake up to300mL, the reduction in THI scores reaches closeto20points.As apossibleexplanationfor these dif-ferences,itmaybesurmisedthatelderlypatientsprobably presentagreaternumberoffactorsinvolvedinthe percep-tionoftinnitus,suchaspresbycusisanduseofmultipledrugs totreatvariousmedicalconditions.
Patientswithhighercoffeeintakemaybemore suscepti-bletosymptomsafterwithdrawalfromcaffeine,asreported bySt.Claireetal.18Althoughonlyoneofthepresentstudy’s patientshaveshownsignscompatiblewithwithdrawal,the possibilitythattheworseningofthetinnitusisasymptom relatedtoabstinencecannotberuledout,whichcould out-weighanypotentialbenefitofareductionincaffeineintake. Furthermore, the present study did not examine the percentage of caffeine reduction in each patient. Thus, consideringthemethodologyused,thegreatertheamount ofcaffeineconsumed,thegreatertheimpactcausedbythe reductionofintake,whichcouldberesponsiblefora possi-bleworseningoftinnitus,relatedtocaffeinewithdrawal.
Consideringthedata,theauthorsbelievethatthis repre-sentsanappropriatemanagementstrategyforeachpatient. Whiletherearenodatasupportingthebeneficialeffectsof reducingcaffeineforalltinnituspatients,somesubgroups, suchasyoungpatientswithbilateraltinnitusandthosewith moderatecaffeineintakearemorelikelytoimprove.
Muchliketheproceduresforvestibulardisturbances,and considering thepossible effectsof an abruptreductionof caffeineintake,perhapsthebestoptionisagradual reduc-tion,ratherthanthecompletesuppressionofthissubstance. Periodsof30daysofobservationappeartobesufficientto evaluateapossiblebeneficialeffectandshouldberoutinely usedintherapeutictests.
Conclusion
Theresultsobtainedinthisstudysuggestthatthereisno jus-tificationfortheuniversalrestrictionofcaffeineintakeasa treatmentforallpatientswithtinnitus.However,patients youngerthan60years,withbilateraltinnitus,andwithdaily coffeeintakebetween150and300mLpresentgreater ben-efits.Theobservationperiodof30daysmaybeusefulfor thetherapeuticdecision.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Nehlig A. Are we dependent upon coffee and caffeine? A review on human and animal data. Neurosci Biobehav Rev. 1999;23:563---76.
2.(ABIC) Associac¸ãoBrasileira de Indústrias do Café. Available
from:http://www.abic.com.br[cited08.20.10].
3.DalyJM.Mechanismofactionofcaffeine.In:S.G.,editor. Caf-feine, coffee, and health. New York: Raven Press; 1993. p. 97---150.
4.DixitA, Vaney N,Tandon OP.Effect ofcaffeineingestion on cognitivebrainfunction.IndianJPhysiolPharmacol.2004;48: 79.
5.LoristMM,SnelJ,KokA.Influenceofcaffeineoninformation processingstagesinwellrestedandfatiguedsubjects. Psyco-physiology.1994;113:411---21.
6.Koppelstaeter F, Poeppel TD, Siedentopf CM, Ischebeck A, VeriusM,HaalaI,etal.Doescaffeinemodulateverbal work-ing process memory? An fMRI study Neuroimage. 2008;39: 492---9.
7.KawamuraN, Maeda H, NakamuraJ, Morita K, Nakazawa Y. Effectsofcaffeineonevent-relatedpotentials:comparisonof oddballwithsingletoneparadigms.PsychiatryClinNeurosci. 1996;50:217---21.
8.NehligA,BoyetS.Dose---responsestudyofcaffeineeffectson cerebralfunctioningactivitywithaspecificfocuson depend-ence.BrainRes.2000;858:71---7.
9.Dixit A, Vaney N, Tandon OP. Effect of caffeine on cen-tralauditorypathways:anevokedpotentialstudy.HearRes. 2006;220:61---6.
10.SlepeckyS,UlfendahlM,FlockA.Effectsofcaffeineand tetra-caineonouterhaircellsshorteningsuggestintracellularcalcium involvment.HearRes.1988;32:11---22.
11.YamamotoT,KakehataS, YamadaT,SaitoT, SaitoH, Akaike N. Caffeine rapidly decreases potassium condutance of dis-sociated outer hair cells of guinea pig cochlea. Brain Res. 1995;677:89---96.
12.Skellett RA, Crist JR, FallonM, Bobbin RP.Caffeine-induced shorteningofisolatedouterhaircells:anosmoticmechanism ofaction.HearRes.1995;87:41---8.
13.Desmond ALD.Vestibular function: evolutionand treatment. NewYork:Thieme;2004.p.97---8.
14.FelipeL,SimõesLC,Gonc¸alvesDU,ManciniPC.Evaluationof thecaffeineeffectinthevestibulartest.BrazJ Otorhinolaryn-gol.2005;71:758---62.
15.Gananc¸aMM,VieiraR,CaovillaHH.Princípiosemotoneurologia. RiodeJaneiro:Atheneu;1998.
16.AzevedoAA, FigueiredoRR. Atualizac¸ãoem zumbido.BrazJ Otorhinolaringol(CadernodeDebates).2004;70:27---40.
17.GoodeyR.Tinnitustreatment-stateoftheart.In:LangguthB HG,KleinjungT,CacaceA,MollerA,editors.Tinnitus: patho-physiologyandtreatment.166ed.London:Elsevier;2007.p. 237---46.
18.Claire St, Stothart L, Mc Kenna G, Rogers LPJ. Caffeine abstinence:anineffectiveandpotentiallydistressingtinnitus therapy.IntJAud.2010;49:24---9.
19.SchmidtLP,Teixeira VN,Dall’IgnaC,DallagnolD,Smith MM. BrazilianPortugueselanguageversionofthe‘‘TinnitusHandicap Inventory’’:validityandreproducibility.BrazJ Otorhinolaryn-gol.2006;72:808---10.
20.ZemanR,KollerM,FigueiredoR,AzevedoA,RatesM,Coelho C,etal.Tinnitushandicapinventoryforevaluatingtreatment effects:whichchangesareclinicallyrelevant?OtolaryngolHead NeckSurg.2011;145:282---7.