www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Sound
generator
associated
with
the
counseling
in
the
treatment
of
tinnitus:
evaluation
of
the
effectiveness
夽
Andressa
Vital
Rocha
a,∗,
Maria
Fernanda
Capoani
Garcia
Mondelli
baFaculdadedeOdontologiadeBauru,UniversidadedeSãoPaulo(USP),Bauru,SP,Brazil bDepartmentofAudiologyandSpeechPathology,FaculdadedeOdontologiadeBauru,
UniversidadedeSãoPaulo(USP),Bauru,SP,Brazil
Received23December2015;accepted18March2016 Availableonline11November2016
KEYWORDS Tinnitus; Hearingloss; Hearingaid
Abstract
Introduction:Therelationsbetweenthetinnitusandthehearinglossareduetothesensory deprivationcausedbyhearingloss,sincethisisfollowedbythefunctionalandstructural alter-ationoftheauditorysystemasawhole.Thecochlearlesionsareaccompaniedbyareduction intheactivityofthecochlearnerve,andtheneuralactivitykeepsincreasedinmainlyallthe centralauditorynervoussystemtocompensatethisdeficit.
Objective: Thisstudyaimedtoverifytheeffectivenessofthesoundgenerator(SG)associated withthecounselinginthetreatment ofthetinnitusinindividualswithandwithouthearing lossregardingtheimprovementofthenuisancethroughTinnitusHandicapInventory(THI)and VisualAnalogueScale(VAS).
Methods:Thesampleconsistedof30individualsofbothgendersdividedintotwogroups:Group 1(G1)wascomprisedof15individualswithtinnitusandnormalhearing,adaptedtoSG;Group 2(G2)wascomprisedof15individualswithcomplaintsofhearingacuityandtinnitus,adapted withSGandanindividualhearingaiddevice(HA).Bothgroupsunderwentthefollowing proce-dures:anamnesisandhistoryofcomplaint,highfrequencyaudiometry(HFA),imitanciometry, acuphenometrywiththesurveyofpsychoacousticpitchandloudnessthresholdsandapplication ofthetoolsTHIandVAS.AllofthemwereadaptedwithHAandSiemensSGandparticipated inasessionofcounseling.Theindividualswereassessedinthreesituations:initialassessment (before theadaptationoftheHAandSG),monitoringandfinalassessment(6months after adaptation).
Results:Thecomparisonofthetinnitusnuisanceandhandicapinthethreestagesofassessment showedasignificantimprovementforbothgroups.
夽 Pleasecitethisarticleas:RochaAV,MondelliMF.Soundgeneratorassociatedwiththecounselinginthetreatmentoftinnitus:evaluation
oftheeffectiveness.BrazJOtorhinolaryngol.2017;83:249---55.
∗Correspondingauthor.
E-mail:[email protected](A.V.Rocha).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.03.021
Conclusion:TheuseoftheSGwassimilarlyeffectiveinthetreatmentofthetinnitusin indi-vidualswithandwithouthearingloss,causinganimprovementofthenuisanceandhandicap. © 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Zumbido;
Perdaauditiva; Aparelhoauditivo
Geradordesomassociadoaaconselhamentonotratamentodezumbido:avaliac¸ão daeficácia
Resumo
Introduc¸ão:Asrelac¸ões entreozumbidoeaperdadeaudic¸ãoadvêm daprivac¸ãosensorial causadapelaperdaauditiva,umavezqueestaéseguidapelaalterac¸ãoestruturalefuncional dosistemaauditivonoseuconjunto.Aslesõescoclearessãoacompanhadasporumareduc¸ão daatividadedonervococleareaatividadeneuronalmantém-seaumentadaemprincipalmente todooSistemaNervosoAuditivoCentralparacompensarestedéficit.
Objetivo:EsteestudotevecomoobjetivoverificaraeficáciadoGeradordeSom(GS)associado ao aconselhamentonotratamentodozumbido emindivíduos comesemperdaauditiva em relac¸ãoàmelhoradoincômodopormeiodoTinnitusHandicapInventory(THI)eEscalaAnalógica Visual(VAS).
Método: Aamostraconsistiuem 30indivíduosdeambos ossexos,divididosemdoisgrupos: Grupo 1(G1)foicompostopor15 indivíduoscomzumbido eaudic¸ãonormal, adaptados ao GS;oGrupo2(G2)consistiuem15indivíduoscomqueixasdeacuidadeauditivaezumbido, adaptadocomGSeumaparelhoauditivoindividual(AA).Ambososgruposforamsubmetidosaos seguintesprocedimentos:anamneseehistóriadaqueixa,AudiometriadeAltaFrequência(AAF), imitanciometria,acufenometriacomolevantamentodelimiarespsicoacústicosdeFrequência eAlturaeaplicac¸ãodasferramentasTHIeVAS.Todoselesreceberamadaptac¸ãodeAAeGS Siemenseparticiparamdeumasessãodeaconselhamento.Osindivíduosforamavaliadosem trêssituac¸ões:Avaliac¸ãoInicial(antesdaadaptac¸ãodoAAeGS),MonitoramentoeAvaliac¸ão Final(6mesesapósaadaptac¸ão).
Resultados: Acomparac¸ãodoincômododozumbidoedeficiêncianastrêsfasesdeavaliac¸ão mostrouumamelhorasignificativanosdoisgrupos.
Conclusão:OusodeGSfoiigualmenteeficaznotratamentodozumbidonosindivíduoscome semaperdadeaudic¸ão,causandoumamelhoradaperturbac¸ãoedadeficiência.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
creativecommons.org/licenses/by/4.0/).
Introduction
Therelationsbetweenthetinnitusandthehearinglossare duetothesensorydeprivationcausedbyhearingloss,since thisis followedbythefunctionalandstructuralalteration oftheauditorysystemasawhole.Thecochlearlesionsare accompaniedbyareductionintheactivityofthecochlear nerve, and the neural activity keeps increased in mainly alltheCentralAuditoryNervousSystem(CANS)to compen-satethis deficit. The increase inthe activity of theCANS characterizesahyperactivityofthenervousstructuresthat resultin a ‘‘neural noise’’. This noise can becodified by theownnervoussystem generating the perceptionof the tinnitus.1
Thetheoriessuggestthetinnitusiscausedbyasequence ofcentralchangesthataretriggeredbythedecreaseinthe afferentofthesoundstimulus.Apredictionresultingfrom thistheoryisthat thecompensationof suchafferentmay beawayofpreventingorreversingthechangesintheCANS
badlyadapted, which underlies thetinnitus.The acoustic stimulation,forexample,couldcompensatethisdecreased afference.2
Theacoustictherapyisperformedwiththeinsertionof soundenrichmentintheindividual’sdailylife,anditaims toproviderelieffromtinnitus.Inlessspecificinterventions, the individual may be advised touse strategies, suchas: insertbackgroundmusic duringdailyactivities,usesounds of relaxation, listento music withearphones,use pillows with speakers, use water cascades, use sound generators in the tinnituslevel and conventionalHearing Aids (HA).3
TheHAconsistsoftheamplificationofenvironmentalsounds ---both maskthetinnitusandhelpinhabituationbysound enrichment,theSGproducesthewidebandnoise,songsor anyotherspectrallymodifiedtypeofsound.4
interventional approaches in individuals withand without hearingloss.
Thisstudyaimedtoverifytheeffectivenessofthesound generator(SG)associatedwiththecounselinginthe treat-mentofthetinnitusinindividualswithandwithouthearing lossregardingtheimprovementofthenuisanceand handi-cap.
Methods
The study was designed as a prospective cohort non-randomized clinical trial, and it was carried out at the Speech-LanguagePathology andAudiologyClinic,withthe approval of the Institution Research Ethics Committee, underthen◦18001213.4.0000.5417.
A numberof 30subjects ofboth genders wereeligible fortheinclusioninthesampleofthestudy.Theyreported acomplaint ofbilateral chronictinnitusandwere divided intotwogroups.Group1(G1)wascomprisedof15 individ-ualswithnormal hearingandGroup 2(G2)wascomprised of 15individuals witha diagnosis ofsymmetricalbilateral sensorineuralhearinglossfromamildtomoderatedegree.
Group1
G1 was comprisedof 15 individuals of both genders (80% femaleand20%male),withoutacomplaintofauditory acu-ity. The average age was of 55.87 years,witha standard deviationof10.27.Themostfrequenttinnituswerewhistle (n=3),pressurecooker(n=1),mosquito(n=1),bell(n=1), cricket(n=2),grasshopper(n=1),waterfall(n=1), wheez-ing(n=2),feedback(n=1),bee(n=1)andbutterfly(n=1). Allsymptomswerereferredtobilaterally(n=15).
Regardingthehearing,themeanofthehearing thresh-oldsobtainedforthisgroupwasof15.33dB---withastandard deviationof5.33fortherightear,andmeanof15.50dB ---withastandarddeviationof5.08fortheleftear.
Group2
G2wascomprisedof15individualsofbothgenders(53.33% female and 46.66% male), with a complaint of auditory acuity. The average age was 63.6 years, with a standard deviationof7.61.
The mean of the hearing thresholds obtained was of 37.77dB---withastandarddeviationof7.52fortherightear, andmeanof35.83dB---withastandarddeviationof11.21for theleftear.Figs.1and2bringthethresholdsobtainedfor theconventionalaudiometryandhighfrequencyaudiometry fortherightandleftears.
Regardingthedegree ofhearingloss,9individuals pre-sentedmild degreeand6 moderatedegree,equivalentto 60%and40%,respectively.
The studywascomprisedofthreestages:initial assess-ment---stageinwhichthepatienthadacomplaintoftinnitus withoutintervention.Monitoring(3months)andfinal assess-ment(6months).
After the otorhinolaryngological evaluation, the indi-vidualsunderwent anamnesisand Visual Inspectionof the ExternalAcousticMeatus(EAM)toverifytheoccurrenceof
0 0.25 kHz
Group 1 Group 2
0.50 kHz 0.75 kHz 1 kHz 1.5 kHz 2 kHz 3 kHz 4 kHz 6 kHz 8 kHz 9 kHz 10 kHz 11.2 kHz 12.5 kHz 14 kHz 16 kHz 20
40
60
80
Figure 1 Values of mean, maximum and minimum audio-metric thresholds of the right ear (RE) in the stages initial assessment,monitoringandfinalassessmentofthegroupsG1 andG2.
some impediment of the middle and/or outer ear. After-wards, they underwent the hearing assessment including conventionalpuretoneaudiometryandHFA.Theextended frequenciesevaluatedfrom8kHzwere9,10,12.2,12.5,14 and16kHz.
ThequestionnaireTinnitusHandicapInventory(THI)was appliedinallstagesofthestudy;itwastranslatedand vali-datedfortheBrazilianPortuguese5andassessesthetinnitus
handicap bymeasuring itsgeneral nuisance and domains: functional, emotional and catastrophic.The highest total scorepossiblecorrespondsto100points,anditisbelieved toshowa maximumimpairmentofthe patient’sdailylife duetothetinnitus.
The VAS canalso measurethe nuisance of thetinnitus for the individual. The scale consists of a ‘‘ruler’’ with graphicrepresentationsequivalenttothegrades0---10.The useoftheimageproducesavisualreinforcementthatcan berememberedbythepatient.
The measuring of the tinnitus was performed through theacuphenometry,withthesurveyofPitchandLoudness similartotheindividual’ssensation.Thismethodis subjec-tiveandcomprises aset ofaudiological techniques totry tofinda psychoacoustic thresholdthe closest possible to
0
20
40
60
80
0.25 kHz Group 2
Group 1
0.50 kHz 0.75 kHz 1 kHz 1.5 kHz 2 kHz 3 kHz 4 kHz 6 kHz 8 kHz 9 kHz 10 kHz 11.2 kHz 12.5 kHz 14 kHz 16 kHz
thepatient’s tinnitus at themomentthe symptom occur-renceis.Thepatientsweretoldtosignalraisingoneofthe handswheneverthesignpresentedwastheclosesttotheir tinnitus.
Initially,thePitch (sensationoffrequency) ofthe tinn-itus wasinvestigated througha pure tone or narrowband noise,depending onthe characterizationof the symptom presented by the individual. The stimuli were presented 5dB higher than the audiometric thresholds. Afterwards, the Loudness (sensation of intensity) was investigated in thepreviouslyestimatedfrequencyofthetinnitusandinits audibilitythreshold.Thesignalwasincreasedinstepsof5dB untilthepatientreportedtobeequivalenttothesystem. Thethresholdswereretested,andwefoundthemeanofthe valuesobtainedinthetwotimesinwhichthe‘‘selected’’ stimuliintensitieswerepresented.Intheoccurrenceofthe tinnitussuppression(partialortotal),therepetitionswere notmeasured,throughtheabsenceofthesymptom.
TheindividualswereadaptedtotheHAmini retroauric-ularopenfitting,Life,Siemens,withsiliconeeartipsanda thintube,accordingtoeachparticipant’saudiological char-acteristics,physicalandacousticneeds.
The HApresented theconventionalresources of ampli-fication associated with the SG (Programmable Tinnitus Controlalgorithm)withwidebandnoise(whitenoise),from 250Hz to8kHz,which canbeusedasan amplifier,sound generatororboth.
Thus,thegroupswereadaptedasfollows:
Group1(normalhearingandtinnitus):bilateraladaptation with‘‘soundgenerator’’activated,consideredas‘‘only’’ adaptation.
Group 2 (hearingloss and tinnitus): bilateral adaptation with the ‘‘sound generator’’ and ‘‘amplification’’ acti-vated to overcome hearing loss, and considered as a ‘‘combined’’adaptation.
TheSGadjustmentsforthegroupswereperformedinan ascendantway.Thus, theintensity ofthenoise was grad-uallyincreaseduntilthepatientsignaledthecomfortand audibilitypointwasmet.The‘‘mixingpoint’’wasverified inseveralsituationsassomepatientsreportedthemixture ofbothsounds.
ToensuretheeffectiveuseoftheHAandverifythe effec-tivenessofthesoundtherapy,onlysoftwarewasactivated: ‘‘universal’’.G1withonlytheSGandG2withtheHAand theSGassociatedprovidingstimuliconcomitantly.The indi-vidualweretoldtousetheHAforaminimumperiodof8ha day,takingitouttoshowerandsleep.Theeffectiveusewas verifiedthroughtheactivationofthedataloggingalgorithm. To verify the amplifications, patients of the G2 had themeasures taken withprobe microphone,an objective method that expresses the real quantity of amplification providedby the HAin the patient’s conduit.We selected theprescriptivemethoddevelopedbytheNational Acous-ticLaboratories ---NALNL1, fornon-linearHA,compatible withtheequipmentrule,inwhichthemeasurementswere performedtoverifytheeffectivenessoftheamplification.
AtthetimeofadaptingtheHA,acounselingsessionwas carriedout.Thissessionaddressedissuesregardinghearing physiology,pathophysiology of tinnitus and hearing, using simplelanguageanddigitalmaterialwithsomeillustrative
images proposed6 --- authors responsible for the scientific
basis of the counseling associated with the fitting of the SiemensHAusedinthisstudy.
Fromtheseguidelinesandawareness,theresearch par-ticipants obtainedthe audibilityandcomfort pointof the SG,basedontheauditoryperceptionofthepatient, finish-ingtheprogrammingofthehearingaids.
Methods
and
statistical
analysis
The analysis of the results was carried out based on the inductiveorinferentialstatistics.Allstatisticalprocedures wereperformedinthesoftware5.1Statistica(StatSoftInc., Tulsa,USA), witha significancelevelequal to5%.Forthe descriptive analysis,we usedthe mean and the standard deviationofallnumericalvariables.Fortheinferential anal-ysis,weperformedtheanalysisofvarianceofthemeasures repeatedinbothcriteria(ANOVA)toverifythepossible sig-nificanceinthetreatmentofthegroupsisolated.Afterthe ANOVAandthefindingofa significantdifferencebetween treatments, we usedthe test of multiple comparisons to verifythemagnitudeofsuchdifferences:Tukey’stest.
Results
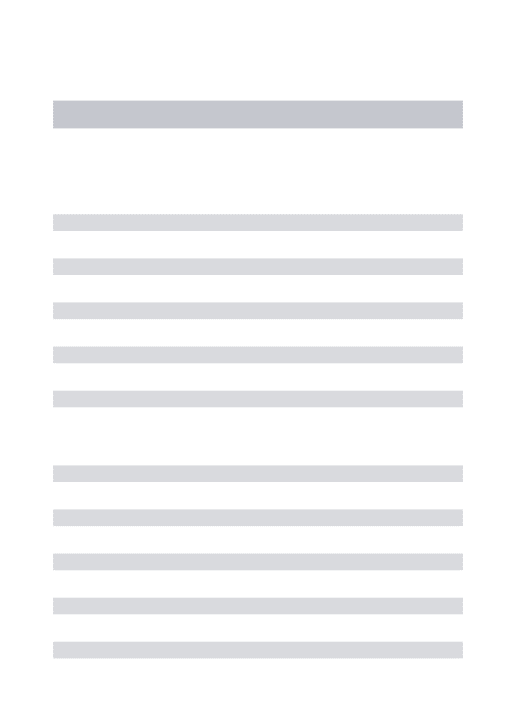
ResultsoftheTHIinthestagesinitialassessment, monitor-ing and finalassessment for both groups are described in
Table1.
Table1 ValuesofmeanandSDoftheanswersobtainedfor theTHI---totalscore,functional,emotionalandcatastrophic categoriesinthethreestagesofassessment.
THI Mean±SD
G1 G2
Totalscore
IA 66.66±12.27a 66.4±13.79a
MO 22.13±16.96b 18.66±12.45b
FA 11.6±10.03c 10.6±12.88b
Functional
IA 36.66±10.32a 34.2±7.38a
MO 9.86±8.33b 10.8±6.53b
FA 5.46±5.26b 6.4±6.97b
Emotional
IA 16.66±6.17a 18.8±6.36a
MO 5.6±5.19b 3.6±4.61b
FA 2.53±3.81b 2.93±4.58b
Catastrophic
IA 12±3.46a 14.13 ±5.47a
MO 4.8±3.76b 4.26±2.49b
FA 2.53±2.35b 2.93±3.01b
Differentsuperscriptlettersinthesamecategoryindicate statis-ticallysignificantdifferenceinthecomparisonbetweengroups (repeatedmeasuresANOVAandTukey,p<0.05statistically sig-nificant).
Table2 ValuesofmeanandSDoftheanswersobtainedfor theVASinthethreestagesofassessment.
VAS Mean±SD
G1 G2
IA 8.66±1.34a 8.0±1.19a
MO 2.93±1.79b 3.4±2.02b
FA 1.8±1.78b 1.66±1.95c
Differentsuperscriptlettersinthesamecategoryindicate statis-ticallysignificantdifferenceinthecomparisonbetweengroups (repeatedmeasuresANOVAandTukey,p<0.005statistically sig-nificant.
SD,standarddeviation;IA,initialassessment;MO,monitoring; FA,final.
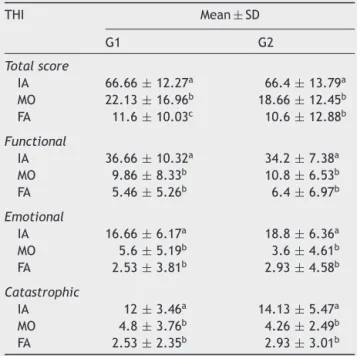
Table3 ValuesofmeanandSDoftheanswersobtainedin theacuphenometryintheinitialassessment.
Acuphenometry Mean±SD
G1 G2
Pitchofthetinnitus
RE 8.16±2.92 6.73±1.94 LE 8.44±2.71 6.86±1.95
Loudnessofthetinnitus(dBSL)
RE −1.33±14.69 1.33±13.07 LE −2.66±14.86 7.66±10.66
SD,standarddeviation;RE,rightear;LE,left ear;Hz,hertz; dBSL,decibelsensationlevel.
ResultsoftheVASinthestages:initialassessment, mon-itoringandfinalassessmentforbothgroupsaredescribedin
Table2.
The psychoacoustic thresholds of the acuphenometry results in thefirst stage of thestudy for both groups are described in Table 3.The psychoacoustic thresholds were not assessed in thestages of monitoring andfinal assess-mentofthepatientswithouttinnitusatthemomentofthe care,fromapartialortotalsuppressionofthesymptom.
Discussion
Professionalswhoworkinthehearingareahaveexperienced anincreaseinthenumberofindividualswithtinnitus---with orwithouthearingloss---thatlookforaneffective interven-tion.
The configuration of the audiometric curves varied (Figs.1 and2) due totheproposal of comprisinga group withhearingthresholdswithinthenormalrange(G1),based ontheconventionalaudiologicaldiagnosis,andagroupwith loweredhearingthresholdsfrom26dBHLtoapproximately 60dBHL(G2).TheresultsoftheHFAshowedtheoccurrence ofaudiometriccurveswithloweredthresholdsfrom8kHzfor bothgroups, suggestingthebeginning ofacochlearlesion even in the individuals diagnosed witha normal hearing. Suchdatacorroboratesthestudiesthatindicatetheorigin ofthetinnitusfromthereductionorabsenceofafferentin theCANS.1,2,7
The performance of the HFA occurs in the hearing monitoringinindividualsatriskofdevelopinghearing alter-ationscausedbyendogenousor exogenousfactors.Study8
observed thefrequencies from4kHz to 6kHz in the con-ventionalaudiometry,and14kHzand16kHzintheHFAare moreaffected. The authors alsosuggest the HFA wasthe mostsensitive test for detecting the hearingloss induced bynoisecomparedtootherexams.TheHFAisanimportant audiologicalexamfortheearlydetectionofhearinglosses duetobaselesionsofthecochlearduct.9
In the clinical practice, it is possible to observe the need of monitoring patients with normal hearing associ-atedwithtinnitus.Datafoundinthisstudyemphasizesthe needofcomplementaryexamsaspatientswithnormal hear-ing,basedontheconventionalprotocol,aredischargedand referredtocounter-referralservices.
Severalauthorsobservedthat,inhighfrequencies, indi-viduals with tinnitus presented hearing thresholds worse than individuals without tinnitus,10---12 corroborating this
studydata,whichindicatestheimpairmentofthehearing acuityathighfrequencies.
Inthisstudy,G2patientsweresatisfiedwiththe adjust-ments from the monitoring, programming and individual specific needs. The HA is usually beneficial for patients withtinnitusthatalsohaveasignificanthearingloss.Some patientsconfuse theoriginsof thedeficitsand blamethe tinnitusfortheircommunicationdifficulties,whichare ini-tiallycausedbyhearinglossand,possibly,withtheaddition ofthetinnitus.Thatis understandableasthehearingloss often progresses slowly over time and people not always realizetheyarelosingacuity.Inthiscontext,studyaffirm thetinnitusistheadditionofanunpleasantperceptionwith asubtlebeginning,andthatmostpatientspaymore atten-tiontothetinnitusindailylifethantotheirgradualhearing loss.3
Therefore,theprofessionalwillbequestionedand con-frontedabout theinterventionin severalsituations. Many patientswillfocusonthetinnitusasthisiswhatreally both-ersthem,notgivingimportancetothehearingtreatment. Thus,theprofessionalhastoknowthecase indetailsand clarifythefactsbeforehand.Thepatientsmustunderstand therelationbetweenthehearinglossandthetinnitus,once theprognosistendstobepositivefromthisunderstanding.
ThequestionnaireTHIisakeytoolforcheckingthe nui-sancecaused by tinnitus and assessing the benefitof the intervention.5 In this study,the THI helped to assess the
impactoftinnitusintheindividual’squalityoflife,enabling theobservationoftheclinicalstatusevolutionofthegroups studied.
Theoverallsampleofgroupsassessedinthisstudy pre-sented an average THI of 66.66 points for G1 and 66.40 for G2, which corresponds to a moderate degree of nui-sance, motivating the individual to look for intervention regardlessthehearingloss.Thesamplesshowedveryclose nuisanceindexes,excludingthepossibilityofnormally hear-ingpatientspresentingagreaternuisancewiththesymptom (Table1).
from the fulfillment of acoustic and sensory needs using the HA, with an enrichment of the environmental sound associatedwiththeSG. Thatdoes notoccurinindividuals withpreserved hearing thresholds as their possible hear-ingdeficitsareinareasmoredistantfromtheSGstimulus, demandingmoretimeforthehabituationandbreakofthe viciousbehavioralcycledue tothenuisance generatedby thesymptom.
The sameinterpretationoccursfor theuse oftheVAS, whichenablestheverificationofthetinnitusinterventionin amoreobjectiveway,oncethepatientnoticesthe improve-mentinasuccinctandtimelymannerwithvisualaid.The groups presented a decrease of the scores in the three assessmentsituationsduringthestudy(Table2).
Intheresults obtainedbythe THI,thenuisance ofthe Groups1and2wasmodifiedfrommoderatetodiscreet,with areductiongreaterthan20pointsfor100%ofthepatients. TheresultsfoundintheVASindicatedareductionfrom8.66 to2.93,andthen 1.80 inG1, andfrom8.00 to3.40,and then1.66inG2,whichreinforcestheeffectivenessofthe treatmentforthegroupswiththesamepattern:aninitial highimprovementandthemaintenanceofthebenefitwith adiscreetimprovementuntilthefinalassessment.
BasedontheTHI,attestedthatmostpatientspresented aninsignificantormildnuisance,andthissymptomdidnot interfereinthedailyactivities.However,intheclinical rou-tine,itispossibletofindcasesinwhichthesymptomisvery uncomfortableanddisabling.13
The researchof the tinnitus frequency indicates acute psychoacousticthresholds(Table3),notextendingtohigher frequencies, a factor that contributed tothe satisfactory resultsafterintervention.Theprognosisispositivewhenthe frequencyofthetinnitusiswithinthelimitsofthefrequency rangeoftheHAselectedfortheadaptation.14Corroborating
thisfinding,thetotalsamplewasbenefitedwiththeuseof theHAandSG,withafrequencyrangeupto8kHz,favoring thesymptomimprovement.
Weobservedintheclinicalpracticethat,afterthe par-tial or total suppression of the symptom, some patients requestedtobedischargedfromtreatment, astheywere satisfied and unaware that the hearing difficulties would continue the same without the rehabilitation, and there could be recurrence of tinnitus due to the lack of sen-sorystimulation.Inthesesituations,theprofessionalmust resume the initial guidance and alert the communication difficultieswillcontinueiftheydonotusetheHAandthe tinnituswillbebackitthereisnosoundstimulationtothe brain.Studyagreewiththisassumption,reportingtheuse oftheHAtostimulatethehearingsystemmaycontribute withthepermanentreductionoftheneuralactivities sug-gestivelyresponsiblefor thegenerationandperceptionof thetinnitus.3
Inthepresentstudy,itwaspossibletoshowthe effective-nessoftheSGinthetinnitustreatmentinthetwogroups. Thisfindingwasobservedintheresultsthatwerepositive andsimilarinbothgroups,measuredbytheTHIandtheVAS asareferenceof themodificationofthe handicap.These findingscorroboratethestudythatverifiedanimprovement inthetinnituswiththeHA,HAassociatedwithSGandthe SG,withnosuperiorityamongthedevices.15
Regardingthestimulususedforthegroups,thenoise pro-videdwasthe‘‘WhiteNoise’’,characterizedbythesample
asacomfortablewheezing.Studysuggestedthewideband noiseismoreeffectivethanthenarrowbandnoise.16Authors
indicatedthe‘‘SpeechNoise’’asmoretolerableandmore likelytosuppressthetinnituswithmoreeffectiveness; how-ever, the objective of the study was not the comparison betweenthesestimuli.17
Thisresearch found theleast intensity capableof pro-viding the relief of the symptom, assuggested in study.6
However, there is evidence the therapeutic approaches interfereintheresultobtainedbytheintervention.Study comparing the effect of the tinnitus management with the mixing-pointmasking (total)proposed by theTinnitus Retraining Therapy(TRT),reportedthe maskingwasmore effectiveinthefirstthreemonthsandthatbothapproaches equaledinthesixthmonth.TRTshowedtobemore effec-tiveinthetwelfthmonth.Thisaspectissimilartotheresults ofthepresentstudy,inwhichtherewereamoresignificant improvementinthefirstthreemonthsofintervention.16Itis
worthtohighlightthat,regardlesstheclinicalsound ther-apeuticapproachselected,the interventionhasitseffect primarilyassociatedwithcounseling.6,18Counselinghelpsin
breakingthe viciouscycle caused bythetinnitus, suppor-tingthepatients’decision-making,aswellasthecopingand thebehaviorchange,wasobservedthataffirmedagreater effectivenessofthetreatmentfromtheuseoftheHAwith counselingcomparedtothecounselingonly.19
The associated approach used in this study was very effective,andwemeasuredthetreatmentsuccess numeri-cally.ThevaluesobservedintheTHIwere22.13and18.66 forGroups1and2,respectively,asatisfactoryimprovement inthefirstthreemonthsofintervention.Thesamepatterns continuedinthenext6months,andtheindexesobtainedin the6-monthreassessmentwere11.6pointsand10.6points. Aproportionalitywasachievedbetweenthegroupswitha qualitative leap of the first assessment in relation to the second, and a morediscreetone in relation tothe third, suggestingtheeffectiveinterventionmaybeverifiedinthe firstthreemonths.
Accordingtotheresults,3monthswereenoughtoverify thebenefitoftheHAassociatedwiththeSGandSGisolated. Study obtained the reduction of the nuisance in the first monthsofinterventionwiththegrouptheyanalyzed.20
Authors, on the other hand, compared the benefit of usingtheHAandtheSG(isolated)inthereductionofthe nuisance generatedby thetinnitusduring12 months,and observed the improvement of the symptom occurred in a progressive way from the three months of intervention, withoutanydifferenceamongthegroups.15
Specifically,theG2analysisshowstheHA,besideshelping intheamplificationoftheenvironmentalsoundsandspeech recognition,favorsthestimulationofthe centralauditory system,providingthereductionofthetinnitusperception.
ThepresentstudyverifiedtheuseoftheSGforpatients with or without hearing loss wasequally effective in the reductionofthenuisancecaused bythetinnitus.Thus,its effectivenessandneedofindicationforpatientswith nor-malhearingisemphasizedintheabsenceofthesymptom.
promotionofbenefitresultsinasymptomwithasignificant subjectivityandindividuality.
Conclusion
The present study enabledus toconcludethe sound gen-eratorassociatedwiththecounselingwaseffectivein the treatment of the tinnitus in individuals withand without hearingloss,providingtheimprovementofthenuisanceand handicap.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
TheSãoPauloResearchFoundation(Fundac¸ãodeAmparoà
PesquisadoEstadodeSãoPaulo---FAPESP)fortheresearch grantprovidedfortheaccomplishmentofthestudy,process number2013/12697-6.
References
1.Nore˜naAJ.Anintegrativemodeloftinnitusbasedona cen-tralgaincontrollingneuralsensitivity.NeurosciBiobehavRev. 2011;35:1089---109.
2.MoffatG,AdjoutK,GallegoS,Thai-VanH,ColletL,Nore˜naAJ. Effectsofhearingaidfittingontheperceptualcharacteristics oftinnitus.HearRes.2009;254:82---91.
3.Folmer RL, Carroll JR. Long-term effectiveness of ear-level devices.OtolaryngolHeadNeckSurg.2006;134:132---7. 4.SantosGM,BentoRF,MedeirosIRT,OiticcicaJ,SilvaEC,
Pen-teado S. The influence of sound generator associated with conventional amplification for tinnitus control: randomized blindclinicaltrial.TrendsHear.2014;18:1---9.
5.FerreiraPEA,CunhaF,OnishiET,BrancoFCA,Gananc¸aFF. Tinn-itusHandicapInventory:adaptac¸ãoculturalparaoportuguês brasileiro.Pró-Fono.2005;17:303---10.
6.TylerRS.Neurophysiologicalmodels,psychologicalmodelsand treatmentsfortinnitus.In:TylerRS,editor.Tinnitustreatment: clinicalprotocols.NewYork:Thieme;2006.p.1---22.
7.Nore˜naAJ,TomitaM,EggermontJJ.Neuralchangesincat audi-torycortexafteratransientpure-tonetrauma.JNeurophysiol. 2003;90:2387---401.
8.MehrparvarAH,MirmohammadiSJ,DavariMH,MostaghaciM, Mollasadeghi A, Bahaloo M, et al. Conventional audiometry, extendedhigh-frequencyaudiometry,andDPOAEforearly diag-nosisofNIHL.IranRedCrescentMedJ.2014;16:e9628. 9.KleinbergKF,OlivaFC,Gonc¸alvesCGO,LacerdaABM,Garofani
VG,ZeigelboimBS.High-frequencyaudiometryinaudiological complementarydiagnosis:arevision.RevSocBrasFonoaudiol. 2011;16:109---14.
10.AzevedoLL,IórioMCM.Estudodoslimiaresdeaudibilidadenas altasfrequênciasemindivíduosde12a15anoscomaudic¸ão normal.ActaAWHO.1999;18:78---85.
11.FiguerêdoRBS,CoronaAP.Tinnitusinfluenceonhigh-frequency hearingthresholds.RevSocBrasFonoaudiol.2007;12:29---33. 12.ShimHJ,KimSK,ParkCH,LeeSH,YoonSW,KiAR,etal.Hearing
abilitiesatultra-highfrequencyinpatientswithtinnitus.Clin ExpOtorhinolaryngol.2009;2:169---74.
13.Carvalho RC, Souza RT, Silva MS, Souza JA. Uso do ques-tionárioTinnitusHandicapInventoryadaptadoparaoportuguês paraavaliac¸ãodaqualidadedevidadospacientescomqueixa dezumbido atendidosnoAmbulatórioAraújoLima. Revhugv. 2010;9:35---41.
14.McNeillC,Tavola-VieiraD,AlnafjanF,SearchfieldG,WelchD. Tinnituspitch,masking,andtheeffectivenessofhearingaids fortinnitustherapy.IntJAudiol.2012;51:914---9.
15.ParazziniM,DelBoL,JastreboffM,TognolaG,RavazzaniP.Open ear hearingaidsin tinnitustherapy:an. efficacycomparison withsoundgenerators.IntJAudiol.2011;50:548---53.
16.Henry JA, Schechter MA, Zaugg TL, Griest S, JastreboffPJ, Vernon JA, et al. Clinicaltrial to compare tinnitus masking andtinnitusretrainingtherapy.ActaOtolaryngolSuppl.2006;6: 4---9.
17.ItoM,SomaK,AndoR.Associationbetweentinnitusretraining therapy and tinnituscontrol instrument.Auris NasusLarynx. 2009;36:536---40.
18.Jastreboff PJ. Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci Res. 1990;8:221---54.
19.Searchfield G. A commentary on the complexity of tinnitus managementclinicalguidelinesprovideapaththroughthefog. EvalHealthProf.2011;34:421---8.