Vol-7, Special Issue-Number4-June, 2016, pp530-537 http://www.bipublication.com
Research Article
ACT effectiveness in reducing aggressive behavior consent from patients
treated with MMT
Soosan Bahrami Kohshahi
Department of Behavioral Science,
Karad University, Tehran,Iran
ABSTRACT
The aim of this study was to determine the effectiveness of ACT on reducing aggressive behavior and improving the quality of the marital relationship and satisfaction with treatment in patients treated with the MMT. The type of the research was Quasi-experimental with a pre-test - post-test plan with the control group.The study population included all patients treated with MMT, in Tehran who have referred voluntary in 2015 for a period of six months to addiction treatment centers in Tehran and have treated.30 people were selectedamong the target population, by random sampling and then people randomly were replaced in two groups of 15 people, including experimental and control groups. The two groupswere evaluated in two steps of pre-test and post-test by questionnaire of the study, and the experimental group has received the treatment based on acceptance and commitment between two steps.Data were analyzed by analysis of covariance. Results showed that scores on aggressive behavior and satisfaction of patients treated with MMT participating in the training group of ACT, has significant difference compared to the group (0.05> P). Therefore, teaching ACT will help the aggressive behaviors and satisfaction of treating patients with MMT.
Keywords: Acceptance and Commitment Therapy, aggressive, treatment satisfaction
INTRODUCTION
Dependence and drug abuseare considered as a chronic and relapsing disorder with environmental, cultural, psychological, social, behavioral and intellectual influences and antecedents. In addition, drug abuse disorders are the most common psychiatricproblems that arise from the interaction of genetic and environmental factors such as abnormal growth and unfavorable psychosocial situation. This disorder can be caused by alcohol, opiates, cannabis, methamphetamine and cocaine, and so on and show themselves in the form of intoxication, dependence and abuse (Ghorbani, Kazemi and Ghorbani, 2011).
Consumption of addictive substances and its dependency is a chronic and recurring phenomenon that is along with serious physical, financial, social and family damages. Less phenomenon can be found that, like addiction, is threatening the human societies. Despite the
risks and complications of addiction, every day the number of victims of this deadly trap will be added (Rooke and Thorsteinsson, 2008).Long chronic diseases and disorders, such as drug abuse and drug dependence will create crisis constantly in the lives of patients, could lead to reduced quality of their life in different aspects of mental and physical, and will cause aggressive behaviors (Emamipoor, Shams, Sadrossadat and Nejad, 2008).
such as humiliation, insults and swearing. In fact, the violenceis considered, including intentional attempted to create physical injury to others (TalaKar, 2010) and aggressiveness can have an adverse impact on a wide range of social functions (Flannery et al., 2012).
Treatment satisfaction refers to patient satisfaction to receive appropriate health-service care to provide the health and meet his inner needs and desires. Patient satisfaction is a cognitive and emotional reaction, in which the patient announces his satisfaction with their needs and at the same time, it is considered as one of the measurement and evaluation methods of care quality,and is the concept that is especially important today in medical care.Patient satisfaction, conditions, process and outcome of treatment effect onfollowing the directions provided, and ultimately, improving the situation and controlling the disease and the patients who have more satisfaction from physicians are better following his orders. (ZahedNejad, Poursharifi and Babapour, 2011) Dissatisfied patients will less use the medical prescriptions, will less follow their current track of treatment, and as a result, will show less signs of improvement. It is also more likely to change their doctor or health system (Rao, 2000). For treating addiction and its complications,many treatments have been studied. One of the treatments that have been used in recent years in this field is the treatment based on acceptance and commitment. In the third wave of psychotherapies that are known as postmodern psychotherapy, it is believed that recognitions and emotions should be considered in the conceptual context of phenomena.For this reason, rather than approaches such as cognitive-behavioral therapy, which modify the recognitions and dysfunctional beliefs so that emotions and behaviorswill be modified, here, the patient is taught that, in the first step, accept their emotions and living in here and now provide more psychological flexibilitythat including these treatments is therapy based on acceptance and commitment (Hayes and Luoma and Bond, 2006; Vilardaga et al., 2014).
In treatment based on acceptance and commitment, it is assumed that humans find a
lot of their emotions, excitements or inner thoughts disturbing and constantly, they try to change their inner experiences orget rid of them.These efforts were ineffective to control and paradoxically, they lead to an intensification of feelings, emotions and thoughts that the person had at first tried to avoid them (Smoot, 2008; Han and McCracken, 2014).
Generally, disorders in which a person will not want to associate with his inner experiences (thoughts, emotions, memories and physical emotions), and take steps to transform this event or aspects of them-even when trying for such things, has a negative impact on quality of life, it is called avoiding experience (Niles et al, 2014). Some researchhas been done,in recent years,on the application of Acceptance and Commitment Therapy for patients with drug abuse (Khakbaz, 1393; Thekiso et al., 2015). For example,Khakbaz (2014) in a research has shown that Acceptance and Commitment Therapy is effective foremotional regulation of methamphetamine-dependent individuals. Also, according to the theoretical framework, this study has been done with the aim of determining the effect of treatment, based on acceptance and commitment to a team approach on aggressive behaviors and satisfaction with the treatment of patients with drug abuse disorders and treated with MMT.Conducting this research from the incremental aspect can strengthen the clinical psychology and its findings have an important role in helping rehabilitation patients treated with MMT, by highlighting the impact of this treatment, for therapists working in this area with strengtheningpsychology research. Therefore, this study seeks to achieve that, if acceptance and commitment group therapy has an impact on aggressive behavior and satisfaction with the treatment of patients with drug abuse or not?
METHOD
variable applying. In this study, the independent variable is acceptance and commitment therapy, and the dependent variable isthe score of aggressive behaviorand treatment satisfaction of patients withdrug abuse, that will obtain from the Buss Aggression Questionnaire (BAQ) and satisfaction of treatment questionnaire.Statistical population of this study was all patients treated with MMT in Tehran, voluntarily, in a period of six months in 2015 that referred to addiction centers, located in area 4th district of 12 region of Tehran and were under treatment.The availability of thesepatients was possible with cooperation of addiction centers in district 4 of Tehran thateventually, 30 subjects were selected as a sample, which were randomly selected and were divided to the same two groups (15 people experimental and 15 people control) and subsequently, they were evaluated with members, with the written agreement, by using considering tools.
Measuring tool
Buss Aggression Questionnaire (BAQ) thatits previous version was hostile questionnaire, was reviewed by Buss and Perry (1992). This questionnaire is a self-report instrument, which contains 29 words and 4 subscalesthat are physical aggression (PA), verbal aggression (VA), anger (A) and hostility (H). Subjects answer the questions in a range of 5 degrees from quite similar to me (5), somehow similar to me (4), is not similar tome and is similar tome (3), somehow not similar to me (2), is quite similar to me (1). Two questions, 9 and 16 are inversely scored. The total score for aggression will be obtained with the total score of the subscale.
The retest coefficient results for the four subscales (with an interval of 9 weeks) were obtained0.80 to 0.72 and the correlation between the four subscales were obtained 0.38 and 0.49. Cronbach's alpha coefficient was used to assess the inner reliability of the scale, that the results showed an internal consistency of physical aggression sub-scale 0.82, verbal aggression 0.81, anger 0.83 and hostility 0.80 (buss, A.H and Perry, M., 1989). The reliability coefficient of this questionnaire with retest way was equal to 0.78. The comparison of these factors
between males and females revealed that males in the three factors of aggression (0.001> p), anger (0.001> p), and hostility (0.01> p) had a significantly more scorethan girls. Also high correlation of these factors with the total score of the questionnaire, the weak correlation of factors with each other and alpha coefficient value indicate the efficacy of this questionnaire for researchers’ application, specialists and psychologists in Iran (Samani, 2007; TalaKar, 2010).
Satisfaction of treatment questionnaire
This questionnaire contained 23 statements that was prepared based on 5-degree of Likert spectrum and is questioned the various aspects of treatment satisfaction of the patients. To validate the content of the questions in their parts of "physical space", "personnel’s communication way" and "service delivery" ware investigated.In order to determine the content validity, in this study, 11 professors of nursing and midwifery university of Medical Sciences, Tehran, Iran, ShahidBeheshti University, TarbiatModarres and health center staff and patients were asked to judge the content validity of designed questionnaires based on content validity index, "relevance", "clarity" and "simplicity".After collecting comments and adding 5 words, content validitywas judged by using content validity standard indices. To assess the formal validity, the questionnaire was distributed among 11 teachers, staff, and clients of the health centers. To determine internal consistency, the questionnaire was distributed among 15 professors of nursing university and health care workers and then the Cronbach's alpha was measured, which was obtained 0.90 (Yaghmaei et al., 2007). In this study, the reliability was calculated by Cronbach's alpha method that the Cronbach’s alpha coefficient values were reported for the four subscales of the questionnaire for the physical aggression 0.82, verbal aggression 0.81, 0.83 and hostilities 0.80.
Methods and Analysis
in 15therapy sessions wasbased onDarrahWestrup’s principle (2014), which have been customized and set by the researcher with the cultural conditions.
After the training sessions end, for both groups at the end of the session a post-test was taken from both groups. After collecting the questionnaires, the raw datawere analyzed by using SPSS and the covariance analysisdue to an intergroup variable (experimental group and control group).
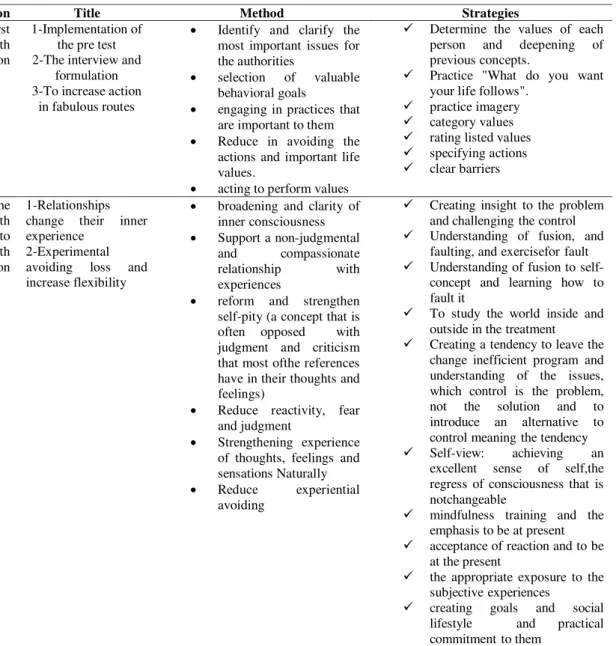
Table 1- The content of training sessions
Findings
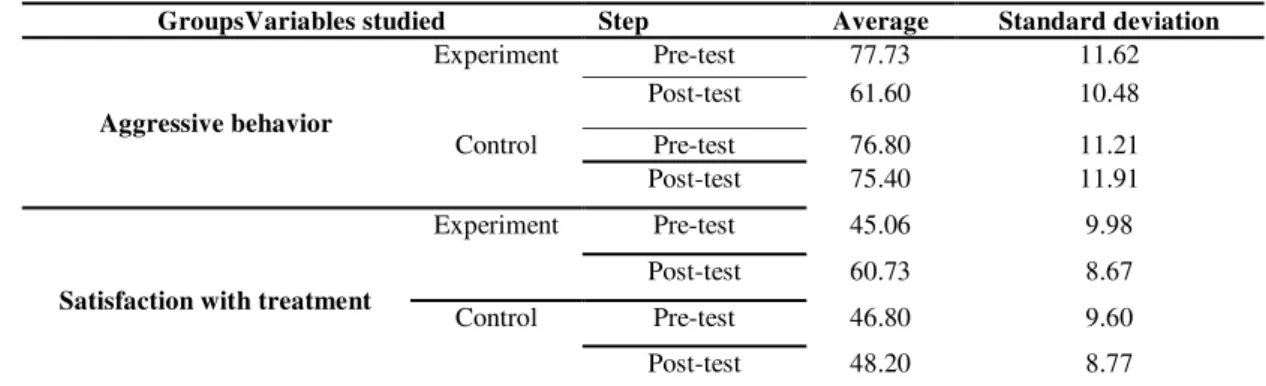
According to Table 2, descriptive indicators ofaverage, and standard deviation of the pre-test and post-test scores and scores of experimental and control groups are provided after excluding the pre-test effect of aggressive behavior and
treatment satisfaction scale. On the average,the aggressive behaviors and treatment satisfaction in pre-test were77.37, 45.06 and in post-test were61.60 and 60.73.The average of score in pre-test in the control group were, respectively, 76.80, 46.80 and in the post-test were75.40 and 48.20. Results of Kolmogorov-Smirnov tests showed that for the study variable, the normalitypre-assumptions of variable distribution in both phases (pre-test and post-test) has been established and the normal assumption is not rejected. Therefore, the use of parametric tests for data is unhindered.
Moreover, the Levine test showed that pre-assumptions related to the homogeneity of variances for study groups is not meaningful in aggressive behavior variable of (P =0.213; F =0.648) and treatment satisfaction (P =0.527; F
Session
Title Method Strategies
The first to sixth session
1-Implementation of the pre test 2-The interview and
formulation 3-To increase action
in fabulous routes
Identify and clarify the most important issues for the authorities
selection of valuable behavioral goals
engaging in practices that are important to them Reduce in avoiding the
actions and important life values.
acting to perform values
Determine the values of each person and deepening of previous concepts.
Practice "What do you want your life follows".
practice imagery
category values
rating listed values
specifying actions
clear barriers
The seventh to fifteenth session
1-Relationships change their inner experience
2-Experimental avoiding loss and increase flexibility
broadening and clarity of inner consciousness Support a non-judgmental
and compassionate relationship with experiences
reform and strengthen self-pity (a concept that is often opposed with judgment and criticism that most ofthe references have in their thoughts and feelings)
Reduce reactivity, fear and judgment
Strengthening experience of thoughts, feelings and sensations Naturally Reduce experiential
avoiding
Creating insight to the problem and challenging the control
Understanding of fusion, and faulting, and exercisefor fault
Understanding of fusion to self-concept and learning how to fault it
To study the world inside and outside in the treatment
Creating a tendency to leave the change inefficient program and understanding of the issues, which control is the problem, not the solution and to introduce an alternative to control meaning the tendency
Self-view: achieving an excellent sense of self,the regress of consciousness that is notchangeable
mindfulness training and the emphasis to be at present
acceptance of reaction and to be at the present
the appropriate exposure to the subjective experiences
=0.410). The hypothesis of equality of variances also been established at both stages. Table 2- The average, standard deviation of aggressive behaviors before and after the ACT divided of the experimental and control groups
GroupsVariables studied Step Average Standard deviation
Aggressive behavior
Experiment Pre-test 77.73 11.62 Post-test 61.60 10.48
Control Pre-test 76.80 11.21
Post-test 75.40 11.91
Satisfaction with treatment
Experiment Pre-test 45.06 9.98
Post-test 60.73 8.67
Control Pre-test 46.80 9.60
Post-test 48.20 8.77
Table 3: Analysis of variance Summary in studying the impact of ACT on aggressive behavior and satisfaction with treatment
Changes source
Sum of
squares
Degrees of freedom
Average of squares
The amount of F
he significance level
Squared Eta Pretest of aggressive behavior
2035.41 1 2035.41 36.83 0.000 0.577
Intergroup
1573.32 1 1573.32 28.47 0.000 0.513
In-group
1491.78 27 55.25
Total
145723 30
Pre-test of treatment satisfaction
369.32 1 369.32 5.65 0.025 0.173
Intergroup
1291.24 1 1291.24 19.78 0.001 0.423
In-group
1762.01 27 65.26
Total
92308 30
In Table 3, the results of two covariance
analyses in studying the Effect of Acceptance and Commitment Therapy in a group on the reduction of aggressive behavior and enhancing the satisfaction of patients treated with MMT are provided. In the first part, the results of Acceptance and Commitment intervention effect on aggressive behavior are examined, and in the second part, the effect of this intervention on treatment satisfaction is examined: As can be seen, the effect of Acceptance and Commitment Therapy has been approved in both variables (0.05> P).
Discussion and conclusion
This study has been done in order to assess the impact of intervention based on acceptance and commitment, in a group, on reducing aggressive behavior and satisfaction with treatment, in the drug abuse patients that are being treated with MMT in Tehran. The results showed a significant difference between the experimental group and control aggressive behavior in post-test, which means that ACT have had a significant effect on the improving aggressive behavior of MMT patients. This finding is consistent with research findings of Wright, D.
and HOLZ (2009; quoted from Cohen, 2014), Khakbaz (2014) and Mosaberi (2014).
In this regard, Khakbaz (2014) in a study entitled "Effectiveness of Group Therapy based on Acceptance and Commitment (ACT) on emotional regulation in rehabilitation methamphetamine-dependent individuals” showed that group therapy based on acceptance and commitment impacts on improving emotional regulation. Mobaseri (2014) also showed in a research that mindfulness-based stress-reduction technique, awareness of anger is effective. Wright, D. and HOLZ (2009; quoted from Cohen, 2014) in an overview research entitled "Mindfulness and treatment of anger problems" showed that mindfulness-based interventions are effective in the treatment of anger problems.
before removing unwanted experiences. Methods of linguistic and cognitive processes in interaction with other non-verbal dependencies, lead to the healthy function. This method involves exposure-based training, linguistic metaphors and methods such as mental health care (Vallis et al., 2003). Mental flexibility is the main goal, which means providing practical ability selection between different alternatives that is relevant, not a practice merely to avoid thoughts; feelings, memories or turbulent desires will be done or in fact will be imposed on the person. In this treatment, at first it is trying to increase psychological acceptance of a person about subjective experiences (thoughts, feelings) and thus to reduce ineffective controlling actions. It is taught to the patients that, any action to avoid or control these mental experiences are unwantedly ineffective or have the reverse effect and exacerbate their impact, and should (these experiences without any internal or external reaction to remove them) be fully accepted. In the second step, mental awareness of a person will be added now, which means the individual will become aware of all mental states, thoughts and his behavior in the present moment. In the third stage, the person is taught to separate himself from these subjective experiences (identification isolation) which would act independently of the experience. Fourth, efforts to reduce excessive focus on self-imagination of personal story (as being a victim) that a person has made for himself in his mind. Fifth, helping the person to recognize his main personal values, and to identify clearly, and convert them into specific behavioral goals (clarifying of values). Finally, creating a motivation to act responsibly which means an action towards the goals and identified values with acceptance of subjective experiences. These subjective experiences can be depressing, obsessive thoughts, thoughts related to events (trauma), fears, and so on (Forman et al., 2008). The purpose of acceptance and commitment therapy method is creating Psychological flexibility thatis defined as the ability to change the behavior or functional stability classes that realize through the goals. In this treatment, they encourage authorities to accept their
uncomfortable feelings and thoughts. They should also consider the reason why the behavior happens and the performance that serves to it (Hayzv et al., 2006). With regard to the cases enumerated for the ACT, it can be concluded that the implementation of ACT on patients with addiction can cause these patients find higher consciousness on their minds, with using mental flexibility on negative thoughts and irrational beliefs and unrealistically expectations, that may be the predispose to aggressive, have more control, and also have commitment on a personal and social ideals and goals in life that all of which ultimately, could prevent aggression behaviors in these patients. The results of this study showed a significant difference between satisfaction with treatment of control and experimental groups, in post-test, which means that ACT has had a significant effect on improving the satisfaction of patients treated with MMT. Reviewing Researches suggest that previous research did not evaluate the impact of ACT on treatment satisfaction. ACT aims to change thoughts functions with manipulating the verbal context that the thought takes place in it (Hayes et al., 1999; Masuda, Hayes, Saket and ToHi, 2004). ACT encourages clients to change their relationship with internal experiences and thoughts and observe them as mental events that come and go, one after the other. Clients learn to observe the thoughts just as thoughts, feelings just as feelings and memories just as memories. Because experiential avoidance occurs, fault-recognition and acceptance processes will help the person to break the avoiding patterns and their regulating laws (Hayes et al., 2002).
threatening. Thus, the sense of self that is used in ACT will help both the fault and the acceptance of the disease.
Similarly, mindfulness will encourage people to practice frequently, focused attention on neutral motives and targeted awareness of the body and mind, so the individual will be free from mental preoccupation with negative thoughts and rumination, and change their minds from automatic gear.It means, these techniques reduce negative thoughts by increasing awareness of individual from present experiences and returning attention on cognitive systems and more efficient of processing information. Because mindfulness and its teaching make adjustments of feelings without judgment and increase awareness of mental and physical emotions, and help to observe clearly and accept the emotions and physical phenomena, as they occur (Nife, 2003; quoted byBeirami et al., 2013)and follow by trust in life, deep compassion and real acceptance of life events. Therefore, in conjunction with the explanation of these findings, it can be stated that addicted patients who have received the treatment, on the one hand, they have witnessed their mental state improvement, and they have observed that, their disease continues to progress during the works, that it could take effect on satisfaction of treatment. On the other hand, mindfulness in the form of acceptance and commitment therapy, can lead to negative thoughts improvement, dysfunctional attitudes and irrational beliefs that this could lead to treatment satisfaction improvement.
Among the limitations of this study was the lack of drug efficacy control in patients treated with MMT and not following up the results of the treatment. These limitations may have influenced the results. Based on the results, attention to Acceptance and Commitment Therapy in aggressive behavior improvement in patients treated with MMT will be helpful and useful and will be the counselors and therapists’ guide to promote physical and psychological well-being of patients treated with MMT.
ACKNOWLEDGMENTS
Hereby, I appreciate the authorities and those who involved in addiction treatment and centers District 4 in Tehran because of their sincere cooperation.
REFERENCES
1. Khakbaz, Hamid (2014). Effectiveness of group therapy based on acceptance and commitment (ACT) onemotion regulation of rehabilitation methamphetamine-dependent individuals. Master's Thesis of Psychology, University of Welfare and Rehabilitation Sciences
2. Talakar, Mehrdad (2010). Review the effectiveness of cognitive - behavioral group therapy on anger and general health of female students of Khor Asegan University. Master's thesis in General Psychology, Department of Psychology, Islamic Azad University of Surrey. 3. Zahid Nejad, Hadi; Poursharifi.Hamid .Babapour.
Jalil (2010). Healthcontrolrelation council, memory and physician - patient relation with treatment satisfaction in patients.School of Nursing and Midwifery Journal.9 (2). 75-67. 4. Emamipoor, Susan Shams Esfandabad Hassan,
Sadrossadat, Seyed Jalal, Nejad Naderi, Samira (2008) Mental disorders and quality of life comparsion in four groups of male addicts with AIDS, non- addict with HIV and healthy. University of Medical Sciences Shahre Kord Journal, Volume 1, Issue 1, 77-69
5. Ghorbani, Maryam, Kazemi, Hamid, Ghorbani, Tahere, (2011). Comparing irrational beliefs of patients with drug abuse and normal individuals. Knowledge and Research in Applied Psychology, Issue 3, 37-31.
6. Hayes, S. C., Strosahl, K., & Wilson, K. G. (1999). Acceptance and Commitment Therapy: An experiential approach to behavior change. New York: Guilford Press.
7. Niles, A., N., & et al., (2014). Cognitive Mediators of Treatment for Social Anxiety Disorder: Comparing Acceptance and Commitment Therapy and Cognitive-Behavioral Therapy. Behavior Therapy, 45, 5, 664–677. 8. Rooke, S. Hine, W. Thorsteinsson B. (2008)
implicit cognition and substance use: A meta-analysis. Addictive Behaviors, 33(12), 1314– 1328.
9. Masuda, A., Hayes, S. C., Sackett, C. F., &Twohig, M. P. (2004). Cognitive defusion and self-relevant negative thoughts: Examining the impact of a ninety year old technique. Behaviour Research and Therapy, 42, 477-485.
10.Hayes, S. C. &Strosahl, K. D. (2005).A Practical Guide to Acceptance and Commitment Therapy. New York: Springer-Verlag. [Shows how to do ACT with a variety of populations]
Acceptance and Commitment Therapy and Cognitive Therapy for anxiety and depression. Behavior Modification, 31(6), 772-799.
12.Vallis, J.M, & Campbell, W.K, &Foster,C.A, 2003, Parenthood and Marital Satisfaction: A Meta Analytic Review, Journal of Marriage and Family vol 65, pp 574–583 .
13.Cohen, A., (2014). Mechanisms of Change in Brief Couple Therapy for Depression.Behavior Therapy, Volume 45, Issue 3, Pages 402–417. 14.Thekiso, T., Murphy, Ph., Milines, J., Lambe, K.,
Curtin, A., et al. (2015). Acceptance and Commitment Therapy in the Treatment of Alcohol Use Disorder and Comorbid Affective Disorder: A Pilot Matched Control Trial. Behavior Therapy, 46 (6), 717-728.
15.Rao JK. Weinberger M. Visit specific expectation and patient- centered outcomes. Arch FamMed ; 1148-55.
16.Hayes S., Luoma J.B., Bond F. (2006). Acceptance andcommitment therapy: Model, processes andoutcomes. Behavior Research and Therapy, (44), 1-25.
17.Vilardaga, J. C. P., Villatte, M., & Hayes, S. C. (2014). Understanding and taking advantage of experiential work in Acceptance and Commitment Therapy. In N. Thoma (Ed.). 18.Han, K, E, J., McCracken, L, M., (2014). A
systematic review of randomized controlled trials of Acceptance and Commitment Therapy for adults with chronic pain: Outcome domains, design quality, and efficacy. Journal of Contextual Behavioral Science, 3, 4, 217–227. 19.Smout, M. (2008). Psychotherapy for
Methamphetamine Dependence, Drug and Alcohol Services South Australia. 429.
20.Flannery, D, J., Vazsonyi, A, T., Waldman, I, D., (2012).The Cambridge Handbook of Violent Behavior and Aggression (Cambridge Handbooks in Psychology).