MRI should be routine for all patients with localized
prostate cancer? | Opinion: No
Joel B. Nelson 1
1 Department of Urology, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA
___________________________________________________________________________________
Keywords: Magnetic Resonance Imaging; Prostatic Neoplasms; Diagnosis; Watchful Waiting
_______________________________________________________________________________________
One of the basic principles of medical care is that a diagnostic test should inform a clinical decision. If the test is uninformative, it is not useful; if no decision is to be made then a diagnostic test is not necessary. Indeed, performing a diagnostic test when it adds nothing to the decision-making process is not only a waste of healthcare resources, it is potentially harmful, leading to incorrect conclusions or more unnecessary testing. From this perspective, how could mp-MRI potentially inform the initial management of localized prostate cancer?
Men who are candidates for active surveillance based on low-risk prostate cancer (cT1c, PSA<10, Grade Group 1 (Gleason 3+3=6)) may be harboring a higher grade tumor that eluded the initial biopsy, particularly if it is anteriorly placed. mp-MRI has the promise of de-tecting this potentially more serious cancer and avoiding the risk of inappropriate observation. Some have argued men with low-risk prostate cancer with a “normal” mp-MRI (PI-RADS 1) have very little risk of cancer progression. The promise of mp-MRI to provide a better risk assessment in men considering active surveillance is alluring.
Unfortunately, the evidence that mp-MRI used in the initial assessment of clinically localized prostate cancer to improve the outcome of men undergoing active surveillance is lacking. The slow growth of prostate cancer means that even higher grade cancer will become clinical evident, with or without an MRI. Metastatic or lethal prostate cancer in the largest active surveillance cohorts—mostly selected without mp-MRI—are rare events (1). It appears readily available clinical features like PSA, grade and stage are adequate in almost all cases to determine who can safely start down the path of active surveillance. Although a “normal” mp-MRI may be reassuring to a patient and/or their physician it actually adds very little to the decision-making process.
The local staging of prostate cancer based on a digital rectal exam (DRE), which only assesses the posterior aspect of the gland, could be enhanced by the whole-gland assessment provide by mp-MRI. Certainly it is better to know the location, size and extent of the cancer before considering treatment. This information can determine whether the cancer is surgically resectable and guide surgical approach, particularly in the decision to preserve neurovascular tissues. It could also guide a focal therapeutic approach. The improved staging provided by mp-MRI make it an attractive test to obtain in the initial assessment of clinically localized prostate cancer.
DIFFERENCE
OF OPINION
1065
doi: 10.1590/S1677-5538.IBJU.2016.06.04
1066
Unfortunately, mp-MRI is not as nearly as at-tractive as promised in prostate cancer staging. First, prostate cancer is distinguished by multifocality wi-thin the gland. The accuracy of mp-MRI to find all the prostate cancers is woeful. Using the gold-standard of whole-mount histopathology compared to preope-rative mp-MRI, the overall sensitivity of mp-MRI to detect tumors was 47% (2). Sensitivity improved to 72% for tumors over 1 cm or with Gleason score ≥7, and up to 80% for the index tumors. Prostate cancers less than 5 mm in diameter are essentially invisible on mp-MRI. As a staging test, mp-MRI is only use-ful for lesions it can detect: the remainder the gland remains a clinical black box. Second, accurate sta-ging requires defining the extent of an infiltrating cancer. The accuracy of mp-MRI to locate the edge of a cancer is awful. It systematically underestimates histologically determined tumor boundaries. This is particularly true for the most clinically concerning cancers, those with a high imaging suspicion score and high Gleason score (3). This is why focal therapy based on mp-MRI is not nearly as focal as it could be, as a 9 mm treatment margin is advocated with focal therapies to ensure successful treatment of the entire tumor (3). Others have shown prostate cancer foci are an average 11 mm longer and have a volume 3 times greater than estimated by MRI (4). Again, as a staging test, mp-MRI comes up short. Third, the defining the presence of extracapsular extension (ECE) can direc-tly influence a therapeutic approach. Here, mp-MRI has consistently demonstrated high specificity, in the 90% range (5). If one suspects ECE on mp-MRI there is a high likelihood it will be present on final patholo-gical assessment of the specimen. Unfortunately, mp--MRI has very poor sensitivity to detect histological ECE, roughly 50% (5). There is no assurance ECE is not present when the mp-MRI doesn’t detect it. Ove-rall, as a staging test, mp-MRI is far from attractive: “homely” would be a better descriptor.Zealots for mp-MRI in the management of prostate cancer have suggested it has the ability to grade the cancer, or at least distinguish between low--risk (Gleason score 6) and higherlow--risk (Gleason score 7, 8 and 9) tumors. Although low-risk tumors have higher ADCs than higher risk tumors, the ADC over-lap between Gleason score 6 and Gleason score 7 cancers is significant: roughly half of Gleason scores 7 cancers have ADCs that are indistinguishable from Gleason score 6 cancers (6). Furthermore, the ranges of ADC between roughly half of Gleason score 7 and
all Gleason score 8 and 9 cancers are overlapping. By far, the most accurate assessment of grade is by histology, not radiology.
Another problem of mp-MRI for prostate cancer is the significant challenge of accurate inter-pretation. The literature is replete with examples of the variability of radiologists to assess prostate can-cer using mp-MRI (7, 8). The learning curve appears to be steep and long: this is not a skill acquired easily. Unless prostate mp-MRI becomes a standard test in all cases of prostate cancer—a dubious goal given the points articulated above—it is reasonable to question whether there will be enough informative cases to train the world of radiologists to interpret them. Fur-thermore, using the current mp-MRI technology, it seems the limits of this test have been reached. The visual and cognitive challenge for a radiologist to ac-curately define prostate cancer will only be as good as the mp-MRI images that routinely fail to detect, define and characterize prostate cancer.
Value in healthcare has been defined as the outcome divided by the cost (9). Outcomes of men with prostate cancer must be demonstrably improved by introducing the additional expense of mp-MRI for that technology to be considered of value. Frankly, I see almost no evidence mp-MRI has improved the ou-tcome of population of patients with prostate cancer.
Accepting that mp-MRI may not be useful in every man with clinically localized prostate can-cer, isn’t there a role in selected patients, particularly when it may directly influence a surgical approach? In my opinion, the answer to this question must be based on an honest assessment of the outcomes of one’s own surgical series and clinical experience as opposed to practice patterns the field. This is admitte-dly the least scientifically approach to answering the question, but it is also the most applicable to the next patient presenting to me as a surgeon. If including mp-MRI in the initial assessment of that patient will improve his eventual outcome, it should be obtained: if it will not, then it adds nothing.
1067
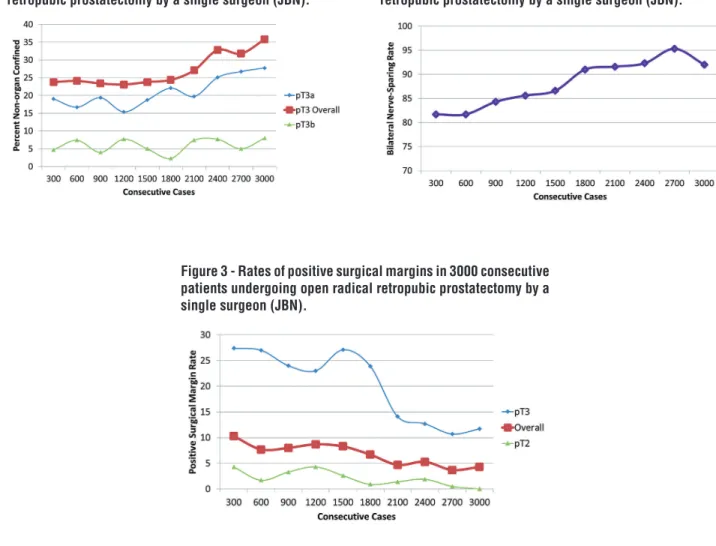
cancer grossly invading the bladder intraoperatively; although mp-MRI may have been useful in avoiding surgery in those handful of cases, it certainly does not justify obtaining imaging even in selected ca-ses. Furthermore, since I routinely widely resect the bladder neck, any positive margin at that location is microscopic and are invisible to mp-MRI. Second, the need to perform a wider resection of the neuro-vascular bundle in an area of suspected ECE is not a mystery. Preoperative DRE and inter-operative assessments are rarely misleading. Third, even if mp-MRI suggests ECE, clinical T3 disease does not equate to surgical futility. Men with pT3 disease can still be cured with radical prostatectomy and mp--MRI should not dissuade taking that approach. In-deed, in my series of 3000 consecutive open radical prostatectomies, the percent of non-organ confined cancers has increased significantly (Figure-1). Despi-te more locally invasive disease, the frequency of bi-lateral nerve-sparing procedures remains over 90%(Figure-2). How? Because for the last 1200 cases, the overall positive surgical margin rate has been under 5% (6.7% for the entire series) (Figure-3). With ex-perience and meticulous attention visual and hap-tic cues, the positive surgical margin rate for pT3 diseases has been less than 15% for the last 1200 cases. Only a fraction of these patients underwent an mp-MRI prior to surgery (obtained by another physician) and in no case did the result of that stu-dy influence the operative approach. Based on this experience, I tell my patients who are candidates for a radical prostatectomy that mp-MRI plays no role in the clinical decision-making process.
I hope my comments will quickly become of historic interest only, as better imaging techniques overcome the current short-comings of mp-MRI and allow precise cancer localization and characteriza-tion. This will make whole-gland focused therapies largely obsolete and allow us to observe the majority of prostate cancers that are of no threat.
Figure 1 - Percent of non-organ confined prostate cancer in 3000 consecutive patients undergoing open radical retropubic prostatectomy by a single surgeon (JBN).
Figure 2 - Frequency of bilateral nerve-sparing procedures in 3000 consecutive patients undergoing open radical retropubic prostatectomy by a single surgeon (JBN).
1068
REFERENCES
1. Yamamoto T, Musunuru B, Vesprini D, Zhang L, Ghanem G, Loblaw A, et al. Metastatic Prostate Cancer in Men Initially Treated with Active Surveillance. J Urol. 2016;195:1409-14. 2. Le JD, Tan N, Shkolyar E, Lu DY, Kwan L, Marks LS, et al.
Multifocality and prostate cancer detection by multiparametric magnetic resonance imaging: correlation with whole-mount histopathology. Eur Urol. 2015;67:569-76.
3. Le Nobin J, Rosenkrantz AB, Villers A, Orczyk C, Deng FM, Melamed J, et al. Image Guided Focal Therapy for Magnetic Resonance Imaging Visible Prostate Cancer: Defining a 3-Dimensional Treatment Margin Based on Magnetic Resonance Imaging Histology Co-Registration Analysis. J Urol. 2015;194:364-70.
4. Priester A, Natarajan S, Khoshnoodi P, Margolis DJ, Raman SS, Reiter RE, et al. MRI Underestimation of Prostate Cancer Geometry: Use of Patient-Specific Molds to Correlate Images with Whole-Mount Pathology. J Urol. 2016; 30 [In press]. 5. Tamada T, Kanomata N, Sone T, Jo Y, Miyaji Y, Higashi H, et
al. High b value (2,000 s/mm2) diffusion-weighted magnetic resonance imaging in prostate cancer at 3 Tesla: comparison with 1,000 s/mm2 for tumor conspicuity and discrimination of aggressiveness. PLoS One. 2014;9:e96619.
6. de Rooij M, Hamoen EH, Witjes JA, Barentsz JO, Rovers MM. Accuracy of Magnetic Resonance Imaging for Local Staging of Prostate Cancer: A Diagnostic Meta-analysis. Eur Urol. 2016;70:233-45.
7. Ruprecht O, Weisser P, Bodelle B, Ackermann H, Vogl TJ. MRI of the prostate: interobserver agreement compared with histopathologic outcome after radical prostatectomy. Eur J Radiol. 2012;81:456-60.
8. Tay KJ, Gupta RT, Brown AF, Silverman RK, Polascik TJ. Defining the Incremental Utility of Prostate Multiparametric Magnetic Resonance Imaging at Standard and Specialized Read in Predicting Extracapsular Extension of Prostate Cancer. Eur Urol. 2016;70:211-3.
9. Porter ME. What is value in health care? N Engl J Med. 2010;363:2477-81.
Joel B. Nelson, MD