Arq Neuropsiquiat r 2002;60(4):964-966
PARACHUTE AND LATERAL PROPPING
REACTIONS IN PRETERM CHILDREN
Lygia Ohlw eiler
1, Alexandre R. da Silva
2,
New ra T. Rot t a
3ABSTRACT - A non-cont rolled, prognost ic cohort st udy w as performed w it h t he aim of est ablishing markers of neurological development and defining a clinical and epidemiological profile of pret erm new borns at 3, 6, 9, and 12 mont hs of gest at ion-correct ed age in t erms of parachut e and lat eral propping react ions. New borns w it h gest at ional age of up t o 36 w eeks and 6 days, w eighing 2,000 g or less at birt h, w ere included in t he st udy At 6 mont hs of age, parachut e and lat eral propping react ions w ere present in 8.1% of t he pat ient s. At 9 mont hs, t he parachut e react ion w as present in 87.5%, and t he lat eral propping react ion w as present in 90% of t he children. It w as possible t o assess parachut e and lat eral propping react ions in pret erm children in t he first year of life. Alt erat ions in t runk-limb coordinat ion may be evidenced in t he 1st year of life t hrough post ural react ions, w hich are maint ained as premat urit y markers unt il school age.
KEY WORDS: psychomot or performance, parachut e, lat eral propping, pret erm new born.
Reações de paraquedismo e apoio lateral em crianças prematuras
RESUM O - Com o objet ivo de t raçar um perfil clinico-epidemiológico e est abelecer marcos do desenvolviment o neurológico de recém-nascidos premat uros aos 3, 6, 9 e 12 meses de idade corrigida, quant o às reações do paraquedismo e do apoio lat eral, foi realizado est udo de coort e não cont rolado, com enfoque prognóst ico. Foram incluídos no est udo recém-nascidos com idade gest acional at é 36 semanas e 6 dias, com 2000g ou menos de peso ao nasciment o. As reações do paraquedismo e apoio lat eral est avam present es em 8,1% aos 6 m eses, em 87,5% e 90% respect ivam ent e aos 9 m eses. Foi possível avaliar as reações post urais do paraquedismo e do apoio lat eral em crianças premat uras no periodo de um ano. Alt erações na coordenação t ronco-membros pode ser evidenciada no 1o ano de vida at ravés de reações post urais, que são mant idas
como marcadores de premat uridade at é a idade escolar.
PALAVRAS-CHAVE: desenvolviment o neurológico, paraquedismo, apoio lat eral, recém nascido premat uro.
Depart ment of Pediat rics, School of M edicine, Universidade Federal do Rio Grande do Sul; and Pediat ric Neurology Unit , Hospit al de Clínicas de Port o Alegre, Port o Alegre RS, Brazil: 1Assist ant Physician; 2Resident ; 3Professor.
Received 15 M ay 2002, received in final form 11 July 2002. Accept ed 19 July 2002.
Dr. Lygia Ohlw eiler - Avenida Pirapó 71/702 - 90470-450 Port o Alegre RS - Brazil - FAX: 55-51-311-1447. E-mail: f p54@t erra.com.br. Premat urit y is a risk fact or for impaired
neurolo-gical development . Even so, 80 t o 90% of pret erm children develop normally, provided no brain-com-promising event s occur1-3. Among several risk fact ors
for neurologic impairment , asphyxia and peri and intraventricular hemorrhage are especially important, due t o t heir pot ent ial for causing neurological da-mage. The effect of perinat al anoxia on t he cent ral nervous syst em (CNS) depends on gest at ional age: in pret erms, perinat al anoxia affect s subcort ical re-gions, and in t erm new borns, cort ical regions. The p resence of sub ep end ym al g erm inat ive m at rix, w hich is richly vascularized and vulnerable to O2 varia-t ions in prevaria-t erms, explains varia-t he variable locavaria-t ion of t his t ype of lesion4,5. The mat urat ion of balance
reac-tions requires a minimal know ledge of the body. Such know ledge is acquired t hrough t he exercise of
laby-rint hine reflexes, and generally of all reflexes, as w ell as t hrough t he accumulat ion of an adequat e amo-unt of impressions received from peripheral recep-t ors, w hich allow recep-t he child recep-t o ourecep-t line a skerecep-t ch of recep-t he surrounding w orld. At 6 mont hs, t he child is already aw are of his/her ow n body. There is a grow ing int e-rest in hand movement s, and gradually t he hands change from t oys t o t ools: t he child is able t o t ry efficacious balance react ions t hat involve a complex int errelat ion of t he sensorial (propriocept ive, visual, and vest ibular), cerebellar, and cort ical pat hw ays6,7.
Arq Neuropsiquiat r 2002;60(4) 965
Lat eral propping usually appears bet w een 6 and 8 mont hs of age, w hen t he child is able t o sit w it hout assist ance. If t he infant is pushed sidew ays w it h an abrupt shove on one shoulder w hile sit t ing, s/he ex-t ends ex-t he appropriaex-t e arm and puex-t s his/her open hands over t he support plane near t he legs or in t he angle formed by t hem.
The evolutional neurological evaluation (ENE) at 7 years of age in a group of preterms show ed a statis-tically significant alteration in trunk-limb coordination in relation to term children10; other studies assessing
school-age children born at term have also observed unaltered trunk-limb coordination11,12. Our w ork aimed
at verif yin g w h et h er alt erat io n s in t ru n k-lim b coordination can be observed in the 1st year of life in preterm children. For that, w e described the clinical-epidemiological profile of preterm new borns at 3, 6, 9, and 12 months of gestation-corrected age in terms of the parachute and lateral propping reactions.
M ETHOD
This st udy w as designed as a non-cont rolled cohort st udy. The f act or under st udy w as prem at urit y and it s clinical effect on postural reactions. The sample w as com-posed of preterm new borns born at Hospital de Clínicas de Porto Alegre, Brazil, from August 1995 to November 1998. Children w ere follow ed for one year. They w ere as-sessed in t he pret erm clinic at 3, 6, 9, and 12 mont hs of age (correct ed for 40 w eeks of gest at ion). A det ailed neu-rological evaluat ion w as carried out , including assessment of neuropsychomot or and language development , of t he lat eral propping and parachut e react ions, and audit ory and visual evoked pot ent ials. Babies born w it h a ges-t ages-t ional age of up ges-t o 36 w eeks and 6 days, w eighing 2,000 g or less, and w ho fulfilled t he inclusion crit eria w ere se-lect ed for t he st udy. Gest at ional age w as det ermined by Ballard’s met hod13.
Exclusion crit eria w ere: Apgar score < 8 at t he 5t h mi-nut e, cerebral hemorrhage, seizures, alt erat ions in cons-ciousness, CNS lesions, congenit al infect ions, genet ic syn-dromes, and prenat al int oxicat ion. New borns present ing clinical intercurrences that could interfere w ith neurological development , such as severe sepsis, jaundice requiring exsanguinat ion t ransfusion, and use of mechanical vent i-lation for more than 7 days w ere also excluded. In addition, children w ho present ed int ercurrences t hat could int erfere w it h CNS development , such as seizures, t raumat ic brain injury w it h neurological sympt oms, infect ion of t he CNS, and alt ered neurological evaluat ion w ere excluded in t he follow -up period. The result s w ere analyzed using t he Epi-Info and SPSS soft w ares.
RESULTS
Fort y pret erm new borns w ho fulfilled t he inclu-sion crit eria w ere assessed; 56.2% w ere f em ale.
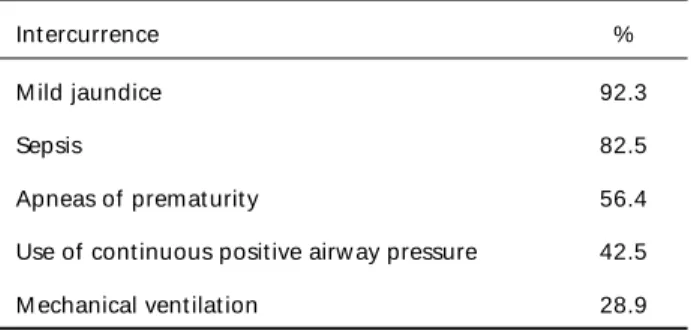
Table 3. Int ercurrences in pret erm new borns.
Int ercurrence %
M ild jaundice 92.3
Sepsis 82.5
Apneas of premat urit y 56.4
Use of cont inuous posit ive airw ay pressure 42.5
M echanical vent ilat ion 28.9
Table 2. Dist ribut ion of new borns according t o birt hw eight .
Birt hw eight (g) n %
< 1000 11 27.5
1000-1500 18 45
> 1500-2000 11 27.5
Tot al 40 100
Table 1. Dist ribut ion of new borns according t o gest at ional age.
Gest at ional age (w eeks) n %
< 30 10 25
30-34 19 45.5
> 34 11 27.5
Tot al 40 100
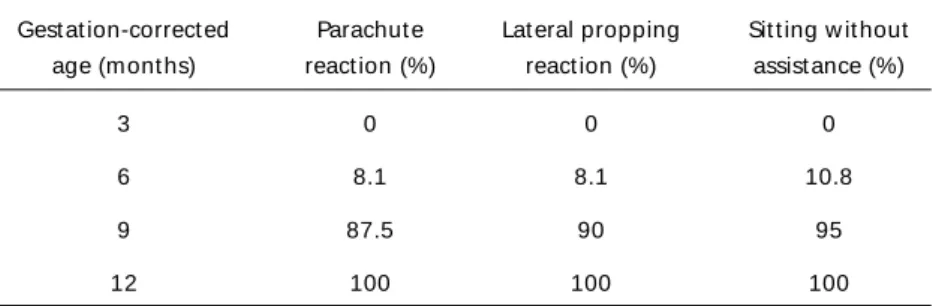
M ean mat ernal age w as 29± 7.9 years. Gest at ional age w as 30-34 w eeks for 45.5% of t he babies, and less t han 30 w eeks for 25% (Table 1). Concerning birt hw eight , 45% present ed low w eight , and 27.5% present ed ext remely low w eight (Table 2). Int ercur-rences during the neonatal period w ere mild jaundice (92.3%), follow ed by sepsis (82.5%), and apneas of premat urit y (56.4%) (Table 3); mean hospit alizat ion t ime w as 44 days. From 6 t o 9 mont hs w e observed a major increase in t he percent age of infant s pre-sent ing parachut e and lat eral propping react ions (Table 4). We observed a similar frequency for t he parachut e and lat eral propping react ions in all ges-t ages-t ion-correcges-t ed ages (3, 6, 9, and 12 monges-t hs); ges-t here w ere small differences result ing from t he fact t hat some children missed one of t he four evaluat ions.
DISCUSSION
966 Arq Neuropsiquiat r 2002;60(4)
show n t o t ake more t ime t o develop it7. Caput e et
al.14 and Blasco15 emphasize t he dist inct ion bet w een
primit ive reflexes and post ural react ions. Primit ive reflexes are t riggered by sensorial st imuli, and t hey are highly st ereot yped. The connect ions t hat are necessary for t hese reflexes are subcort ical, locat ed in t he brain st em. Cort ical mat urat ion inhibit s brain st em reflexes – t hey st art t o appear at 25 w eeks of gest at ion and remain clinically evident unt il 3 t o 6 mont hs of life.
Post ural react ions, on t he cont rary, are not t rue reflexes; t hey require cort ical mat urit y. These mo-vement s are less st ereot yped, and require a complex int errelat ion bet w een cort ical, cerebellar, and sen-sorial (propriocept ive, visual, and vest ibular) pat h-w ays. Lat eral propping and parachut e react ions are observed from 6 mont hs of age on. Our sample of pret erms is considered at low risk for neurological impairment – despit e t he low birt hw eight and ges-tational age – because they did not experience any events that could interfere w ith neurological deve-lopment. Even so, w e found lateral propping and para-chute reactions in only 7.5% of the children studied.
Amiel-Tison and Grenier9 report t hat lat eral
prop-ping react ion appears w hen t he child is able t o sit w ithout assistance; to Coriat7, it manifests itself w hen
t he child st ill requires assist ance t o sit , and reap-pears in special cases, aft er t he child acquires t he abilit y t o sit w it hout assist ance. We consider t he lat eral propping react ion a post ural react ion (not a reflex) for t he maint enance of t runk balance; only at 12 m ont hs of age did all children in our sam ple present t hese react ions.
Balance is maint ained t hrough a complex physio-logic mechanism, in w hich t he ost eoart icular syst em, propriocept ive sensit ivit ies, cerebellar and vest ibular funct ions have import ant roles6. The development
of st at ic balance in t he 1st year of life requires ma-t urama-t ion of ma-t his mechanism; ama-t 6 monma-t hs of age, 50% of t he child ren sit unsup p ort ed , and at 9
mont hs, 100% have acquired t his abilit y16. In our
sample of pret erm new borns, only 10.8% sat unsup-port ed at 6 mont hs of age, and 95% at 9 mont hs.
Post ural react ions are mechanisms acquired t o help balance maint enance. In t his st udy, post ural react ions w ere observed t o appear lat e in m ost children, at 9 mont hs of age (Table 3). Trunk and limb dyskinesia, w hich implies axial musculat ure dys-funct ion, is more visible w hen t here is involvement of t he cerebellar vermis, responsible for t runk ba-lance. We conclude t hat alt erat ions in t runk-limb coordinat ion may be evidenced in t he 1st year of life through postural reactions, w hich are maintained as premat urit y markers unt il school age.
REFERENCES
1. Aylward GP, Pfeiffer SI, Wright A, Verhulst SJ Outcome studies of low birth weight infants published in last decade: a metaanalysis. J Pediatr 1989;118:512-520.
2. Escobar GJ, Littenberg B, Petitti DB. Outcome among surviving very low birthweight infants: a meta-analysis. Arch Dis Child 1991;66:204-211. 3. Allen MC . The high-risk infant. Pediatr Clin N Am 1993;40:479-489. 4. Volpe J J. Current concepts of brain injury in the premature infant. Am
J Roentgenol 1989;153:243-251.
5. Weindling, M. Periventricular haemorrhage and periventricular leukomalacia. Br J Obstet Gynaecol 1995;102:278-281.
6. Thomas A, Saint-Anne Dargassies S. Le nouveau-né normal. In Études neurologiques sur le nouveau-né et le jeune nourrisson. Paris: Masson, 1952. 7. Coriat LF. Maturação psicomotora no primeiro ano de vida da criança.
3.Ed. São Paulo: Moraes, 1991.
8. Paine RS, Brazelton TB, Donovan DE, Drorbaugh JE, Hubbell JP, Sears M. Evolution of postural reflexes in normal infants and in presence of chronic brain syndromes. Neurology 1964; 4:1036-1048.
9. Amiel-Tison C, Grenier A. Neurologic evaluation of the newborn and the infant. New York: Masson, 1983.
10. Ohlweiler L, Alfano L, Rotta N T. Evolutional neurologic evaluation of seven year –old children born prematurely. Arq Neuropsiquiatr 1996; 54:369-374.
11. Rotta NT. Exame neurológico evolutivo e dificuldade no aprendizado. Arq Neuropsiquiatr 1975;33:132-139.
12. Rotta NT, Guardiola A. Aspectos clínicos de la disfuncion cerebral mínima. An Neuroped Latinoamericana 1989;1:59-69.
13. Ballard J L, Khoury JC, Wedig K, Wang L, Eilers-Walsman BL, Lipp R. New Ballard Score, expanded to include extremely premature infants. J Pediatr 1991;119:417-423.
14. Capute AJ, Shapiro BK, Accardo PJ. Motor functions: associated primitive reflex profiles. Dev Child Neurol 1982;24:662-669. 15. Blasco PA. Primitive reflexes: their contribution to the early detection
of cerebral palsy. Clin Pediatr1994;33:388-397.
16. Diament AJ. Exame neurológico do lactente. In Diament AJ, Cypel S (Eds.). Neurologia infantil, 3.Ed. São Paulo: Atheneu, 1996. Table 4 . Appearance of post ural react ions and st at ic balance according t o t he age.
Gest at ion-correct ed Parachut e Lat eral propping Sit t ing w it hout age (mont hs) react ion (%) react ion (%) assist ance (%)
3 0 0 0
6 8.1 8.1 10.8
9 87.5 90 95