AIDS Projections, A Jamaican Perspective
J
.PETERFIGUEROA~
I
have read Alexander Langmuir’s views on the AIDS epidemic with care and respect. However, I do not agree with him that the AIDS epidemic in the United States will crest soon (in 1988) or that the projected number of cases will be as low as one-half the presently accepted figure.Dr. Langmuir bases his views upon Farr’s Law that epidemics rise and fall in a normal curve, as well as upon analysis of AIDS incidence data for the United States from 1982 through 1986. His pre- vious forecast, that the epidemic would crest in “mid-summer of 1986,” was wrong. His explanation for the miscalcu- lation is a “grossly underestimated” in- cubation period and a “lag in reporting.”
My own view is that AIDS projections, whether for the U.S. or any other coun- try, must be made with caution because our information regarding several critical variables is limited. We do not know the extent of human immunodeficiency virus (HIV) infection in most population groups, or the duration and intensity of the infectivity of HIV-positive persons, or whether all HIV-infected people will de- velop AIDS (and if so over what time pe- riod). Nor are we sufficiently familiar with patterns of sexual activity to accu- rately predict the number of AIDS cases in any given country.
Nevertheless, we do have enough in- formation to consider Dr. Langmuir’s forecasts erroneous. In the first place, the AIDS epidemic is the terminal clinical manifestation of a significantly more widespread but silent epidemic of HIV
‘Epidemiology Section, Ministry of Health, l?O. Box 478, Kingston, Jamaica.
infection. As there are many HIV- infected people for every person with AIDS (WHO estimates that there are 50 to 100 HIV-positive people per AIDS case), it is logical to assume that the num- ber of AIDS cases will continue to in- crease over the next few years.
Although the extent of HIV infection in most populations is simply not known, the prevalence studies that have been done have found the level of HIV infection, particularly among high-risk groups, to be almost invariably increas- ing. Thus, people newly infected with HIV are continually being added to the pool of people out of which the AIDS epi- demic grows.
Furthermore, even though the relative proportions of people belonging to the various transmission categories in the United States may not have changed, it would be wrong to conclude that they will not. For instance, the data from the English-speaking Caribbean are showing “a shift from predominantly homosexual spread, seen earlier in the AIDS epi- demic, towards a pattern of predomi- nantly heterosexual transmission” (I). The absolute number of heterosexuals with AIDS in the United States is increas- ing, and there are clear potential routes of HIV infection into the heterosexual community. These include sex with in- fected bisexuals, prostitutes, injecting drug abusers, and people from countries where HIV infection is prevalent. In my view, it is only a question of time before AIDS due to heterosexual transmission accounts for a larger proportion of cases in the United States.
Table 1. AIDS cases in Jamaica, by year of Table 2. Sexual preferences of AIDS patients reporting and sex of patients, 1982-July 1988. in Jamaica, 1982-July 1988.
Sex of patient Annual Cumulative Classification Cases Year Male Female total total of uatient No. (%) 1982 1 0 1 1 Heterosexual
1983 0 0 0 1 Male
1984 1 0 1 2 Female
1985 4 0 4 6 Homosexual
1986 5 0 5 11 Bisexual
1987 20 13 33 44 Child (pediatric case)
1988 15 4 19 63 Unknown
Total 4.6 17 63 63 Total
in order to discuss projections in that country.
Sixty-three AIDS cases had been re- ported in Jamaica (population 2.36 mil- lion) as of 31 July 1988, yielding a cumu- lative AIDS rate of 2.7 cases per 100,000 inhabitants (Table 1). Forty-six of those with AIDS (including children under five years old) were males and 17 were fe- males, so that the male/female ratio was 2.7 to 1. As of 31 July 1988,44 of these 63 people had died, yielding a case fatality rate of 70%.
Nearly all the initial AIDS patients in Jamaica acquired their infections abroad, mainly in the United States. These peo- ple included roughly equal numbers of homosexuals and heterosexuals-mainly
migrant farm workers employed in Belle Glade, Florida, for four to six months each year. It was not until early 1987, when the number of AIDS cases in- creased sharply, that the first female (the common-law wife of a migrant farm worker) and the first child with AIDS were diagnosed. In all, 22 of the 63 peo- ple with AIDS acquired the infection abroad, while in 24 cases the infection was acquired locally and in 17 cases the area of acquisition is unknown.
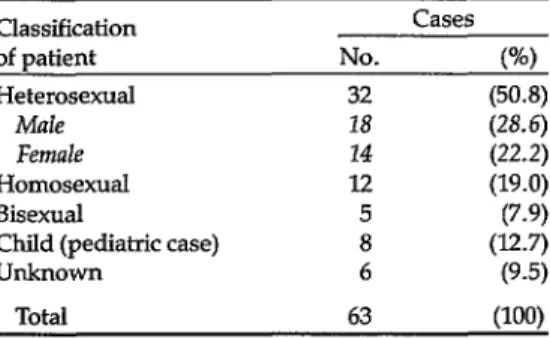
As Tables 2 and 3 indicate, the epidemi- ologic pattern of AIDS in Jamaica is quite different from that found in the United States and Europe. Of the 63 cases, 18 (28.6%) occurred in adult male heterosex-
32 (50.8) 18 (28.6) 14 (22.2) I.2 (19.0) 5 (7.9) 8 (12.7) 6 (9.5)
63 ww
uals and 14 (22.2%) in adult female het- erosexuals, as compared to 12 (19.0%) in exclusively homosexual males and five (7.9%) in bisexual males. In six cases (9.5%), the patient’s sexual preferences are unknown. Thus, heterosexual trans- mission appears to have been nearly twice as common as homosexual trans- mission, accounting for 65.3% versus 34.7% of the AIDS cases in adults with known sexual preferences.
Three Jamaican risk groups have emerged in cases where heterosexual transmission is responsible for AIDS- these being migrant farm workers, pros- titutes, and sailors. The well-recognized association between HIV infection and promiscuity is the most likely explana- tion for AIDS developing in these risk
Table 3. AIDS cases in Jamaica by risk group, 1982-Tdv 1988.
Risk El-OUD
Cases No. (%I Homosexual males 12 Bisexual males 4 BisexuaIsl1.K drug abusers 1
Heterosexuals 20
Migrant farm workers 9 Prostitutes Cfemale) 7
Sailors 4
Chiklren of HIV-positive mothers 8 Blood transfusion recipients 2
Unknown 16
(19.0) (6.3)
(1.6)
(31.7) (14.4) (12.1) (6.3)
(12.7)
(3.2) (25.4)
Total 63 (100)
Table 4. Results of HIV testing in Jamaica.
Test No. of No. positive %
period Group tested tests (by ELISA) positive
12/85-4/88 Blood donors 47,978 127 0.265
1985-1987 Farm workers 31,552" 57 0.18
1985 Food service workers 4,000 0 0
1985 Homosexuals 123 18b 14.6
1985-1986 Sexually transmitted disease clinic attendees 2,400 9b 0.375
1986 Prisoners 239 0 0
=12,000 to 15,000 workers tested annually. bConfirmed by Western blot.
groups. However, a number of the mi- grant farm workers denied promiscuity while admitting to occasional heterosex- ual relations in Belle Glade, Florida, where there is a relatively high level of HIV infection among prostitutes.
The eight children with AIDS all ac- quired the infection through maternal- infant transmission. The high proportion of cases in this category (12.7%) is consis- tent with a pattern of predominantly het- erosexual HIV transmission. The only case involving intravenous drug abuse occurred in a bisexual who acquired AIDS abroad. (1.V drug abuse is not a problem in Jamaica.) The two infections transmitted by blood transfusion were passed before December 1985, when screening of all blood donations was in- troduced.
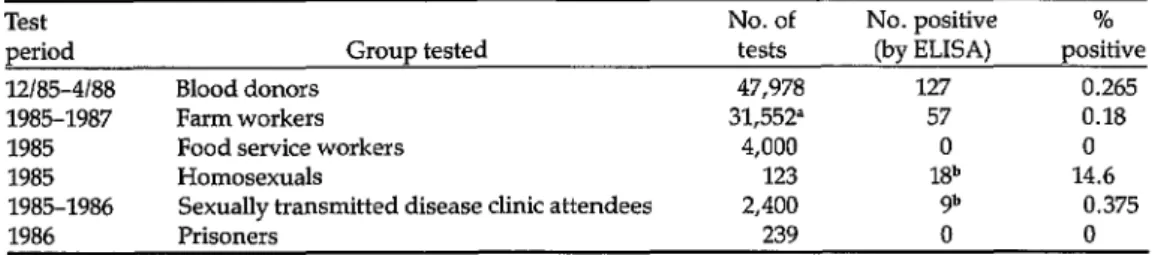
HIV testing in Jamaica has revealed a mixed picture (Table 4). In 1985 none of 4,000 food service workers island-wide and in 1986 none of 239 prisoners were found to be infected, while the level of HIV infection among 2,400 sexually transmitted disease (STD) clinic attend- ees was relatively low (0.375%). HOW-
ever, 0.265% of all blood donations tested from December 1985 through April 1988 were ELISA-positive (the estimated per- centage of true positives based on this figure is 0.125%), a rate higher than that found in the United States; and during 1985 HIV infection was clearly well- established within the homosexual com-
munity. During 1985-1987, 12,000 to 15,000 migrant farm workers were tested annually before departing for the United States. Of the 31,552 tests performed in that period, 0.18% were positive by ELISA, for an estimated prevalence in those workers ranging from 0.38% to 0.475%. It is expected that approximately 94% of the positive results will be con- firmed.
474.8 cases per 100,000 for gonorrhea and 120.8 cases per 100,000 for syphilis in 1987 (4).
Given the pattern of AIDS in Jamaica, there are absolutely no grounds for com- placency concerning the likely course of the epidemic. We are convinced that we will continue to see an increasing number of cases over the next several years, de- spite concerted control program and edu- cational efforts. It is no comfort that the cumulative AIDS rate per 100,000 popu- lation was only two cases in Jamaica as of December 1987, as compared with 19 in Trinidad and Tobago, 20 in Barbados, and 25 in the United States. For reasons not fully understood, the AIDS epidemic in Jamaica is lagging about two years be- hind those in Trinidad and Tobago and Barbados. However, we have no doubt that an increasing number of AIDS cases will arise out of the hidden but exploding HIV epidemic.
Making specific projections of the num- ber of AIDS cases expected in Jamaica is quite different than anticipating the gen- eral course of the epidemic. Three ap- proaches have been used to make such projections. The first simply doubles the number of cases each year over a five- year period beginning with 30 cases in the year ending in September 1987. This approach forecasts 60 cases in September 1988, 120 cases in September 1989, and 960 cases in September 1992.
The second approach estimates the number of HIV-positive individuals by risk group and the number of AIDS cases that can be expected among these indi- viduals by the end of 1992. Using this approach, it has been estimated that there were 3,681 HIV-positive persons in Jamaica as of September 1987 and that some 1,105 AIDS cases would arise within this group by 1992, assuming 30% progression to AIDS within five years (5).
The third approach uses a simplified projection model that assumes an initial
number of HIV-positive people in the population, an annual rate of increase in the number of HIV positives, and an an- nual rate of conversion of HIV infections to AIDS. These three variables can be ad- justed as more information becomes available (5).
The real problem is that for accurate projections to be made, one requires data on the prevalence and incidence of HIV infection that are not readily available. For instance, we have no idea of current levels of HIV infection among prostitutes or their customers, two key groups in the spread of HIV infection in Jamaica. We also have no current information on HIV infection among homosexuals, sailors, informal commercial importers (who travel frequently), workers in the tourist industry, etc. Plans are in place for doing a number of baseline KAP (knowledge- attitude-practice) studies and serosur- veys among these high-risk groups, so as to provide a basis for developing better- targeted interventions. Nevertheless, im- portant gaps will remain in the data base upon which projections must depend.
In the final analysis, public health prac- titioners around the world must decide about the likely course of the AIDS epi- demic in their countries and take appro- priate measures to control the spread of HIV Given the nature of the HIV and AIDS epidemic, Dr. Langmuir is indeed bold in predicting an early cresting of the epidemic in the United States.
Acknowledgments. I wish to acknowl- edge the work of my colleagues, in par- ticular Dr. M. Bullock-DuCasse and Dr. A. Braithwaite.
REFERENCES
1. Caribbean Epidemiology Center. AIDS in the Caribbean: An update. CARE Suweil- lance Report 14(5), 1988.
2. National Family Planning Board in colIabo-
ration with D. Powell, J. Jackson, V. James, C. Watson, L. Morris, and A. Whatley. Young Adult Reproductive Health Survey, Jamaica, 1987, Preliminary Report, Sep- tember 1987. Mimeo. dot. National Family Planning Board, Kingston, 1987.
3. Ministry of Health of Jamaica, Market Re- search Services Ltd., and The Futures Group (SOMARC). Jamaica AIDSlSTD KAP Study 1988. Kingston, 1988.
4. Braithwaite, A. STD Control Programme Annual Report 1987. Ministry of Health of Jamaica, Kingston, 1988.
5. Jillson-Boostrom, I., E. Boostrom, and J. I? Figueroa. Simplified Approaches to Esti- mating Trends in Cases of AIDS. Paper presented at the IV International Confer- ence on AIDS held in Stockholm, 12-16 June 1988. Book of Abstracts 2, Abstract
4691, p. 234.
Changing Pattern of HIV Transmission in the
Caribbean
DAVID
C.BASSETT~ AND JAI I?. NARAIN~
D
r. Langmuir succeeds admirably in showing that any prediction regard- ing AIDS, unless stated very cautiously and for the shortest term, must be subject to serious doubt. His own detailed pre- dictions are for the United States, with Pattern I transmission, and not for Africaand the Caribbean with Pattern II. His paper contains some rather obvi- ous truths, such as that a geometric pro- gression cannot continue indefinitely in a finite population, and at least one “feel- ing” which many would agree with-that AIDS is not about to overwhelm the gen- eral population of the United States. Sex- ually transmitted diseases (STDs) have never overwhelmed whole populations, but neither have they gone away even when readily treatable.
It would be splendid if the right-hand side of Langmuir’s Gaussian curve really represented the future of the epidemic, but there are reasons to doubt this. If the
‘Caribbean Epidemiology Center, l?O. Box 164, Port of Spain, Trinidad and Tobago.
epidemic were to peak in 1988, the curve for HIV infection should have peaked some years ago-perhaps before the dis- ease was recognized-and the incidence of seroconversion should have been de- clining since. Is there evidence of this?
Further, the left-hand side of his curve may not truly represent events to date, and may have led to the false expectation that the epidemic would peak in the im- mediate future.
Dr. Langmuir’s feeling that AIDS will remain within recognized risk groups seems to dismiss the half of heterosexual cases that would particularly interest us in the Third World-those with no known contact with the recognized risk groups.