rev bras ortop.2016;51(1):105–108
w w w . r b o . o r g . b r
Case
Report
Presence
of
a
long
accessory
flexor
tendon
of
the
toes
in
surgical
treatment
for
tendinopathy
of
the
insertion
of
the
calcaneal
tendon:
case
report
夽
Nelson
Pelozo
Gomes
Júnior,
Carlos
Vicente
Andreoli
∗,
Alberto
de
Castro
Pochini,
Fernando
Cipolini
Raduan,
Benno
Ejnisman,
Moisés
Cohen
UniversidadeFederaldeSãoPaulo(Unifesp),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received31December2014
Accepted28January2015
Availableonline21December2015
Keywords:
Tendinopathy Ankle Foot
a
b
s
t
r
a
c
t
Thepresenceofaccessorytendonsinthefootandankleneedstoberecognized,giventhat
dependingontheirlocation,theymaycausedisordersrelatingeithertopainprocessesor
tohandlingofthesurgicalfindings.Wedescribethepresenceofanaccessoryflexortendon
ofthetoes,seeninsurgicalexposurefortransferringthelongflexortendonofthehallux
tothecalcaneus,duetothepresenceofadisorderoftendinopathyoftheinsertionofthe
calcanealtendoninassociationwithHaglund’ssyndrome.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
Presenc¸a
do
tendão
flexor
acessório
longo
dos
dedos
no
tratamento
cirúrgico
da
tendinopatia
insercional
do
tendão
calcâneo:
relato
de
caso
Palavras-chave:
Tendinopatia Tornozelo Pé
r
e
s
u
m
o
Apresenc¸adetendõesacessóriosnopéenotornozelonecessitadeseureconhecimento,
vistoque,adependerdalocalizac¸ão,podemgerarafecc¸ões,sejaemprocessosálgicosou
nomanuseiodoachadocirúrgico.Descrevemosapresenc¸adotendãoflexoracessóriodos
dedosnaexposic¸ãocirúrgicaparatransferênciadotendãoflexorlongodoháluxparao
calcâneonavigênciadeafecc¸ãodetendinopatiainsercionaldotendãocalcâneoassociado
àafecc¸ãodeHaglund.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora
Ltda.Todososdireitosreservados.
夽
WorkperformedintheDisciplineofSportsMedicine,DepartmentofOrthopedicsandTraumatology,EscolaPaulistadeMedicina
(EPM),UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](C.V.Andreoli).
http://dx.doi.org/10.1016/j.rboe.2015.12.003
106
rev bras ortop.2016;51(1):105–108Introduction
Tendinopathyoftheinsertionofthecalcanealtendonwithor
withoutassociatedboneexostosisorHaglund’sdeformityisa
conditionthatisdifficulttotreatanditmaycausefunctional
incapacityandlimitationofathletes’performance.1
Thisconditioninvolves tendondegeneration in
associa-tionwiththickeningofthebursaandthetissuessurrounding
thetendon,togetherwithmechanicalpressureexertedbythe
boneprominence,withdiminutionoflocalvascularization.1
Whenthisconditionissevere,thepercentagesuccessthrough
conservative treatment is low. One treatment option is
to transfer the long flexor tendon of the hallux to the
calcaneus.1,2
Thelongflexorofthehalluxischosenbecauseithas
suf-ficientlength,it isdurable, it isstrongerthan the fibularis
tendon,itscontractionforceaxisissimilartothatofthe
cal-caneal tendonand maintainsthe musclebalance and it is
closetothecalcanealtendon,whichfacilitatesthe surgical
procedure.1,2
Thesurgicalprocedureisperformedinassociationwiththe
necessarydebridementoftheentireareaofdevitalized
tendi-nosisofthecalcanealtendon,withexostectomyorostectomy
oftheposterosuperiorprocessofthecalcaneus,until
decom-pressionoftheentirecalcanealtendonhasbeenachieved.In
thecasepresentedhere,weusedthetechniqueoftransferring
theflexortendonofthehalluxtothecalcaneus,withtendon
harvestingabovethemalleolus1andfixationofthelongflexor
tendonusinganinterferencescrewanteriorlytotheinsertion
ofthecalcanealtendon.Throughthistechnique,the
connec-tionsorlinksofthedistalstumpofthelongflexortendonof
thehalluxwiththeflexortendonofthetoesaremaintained
intact.
Theaimofthiscasereportwastopresentasurgical
find-ingofanaccessorylongflexortendonofthetoes,superficially
andlaterallytotheflexortendonofthehallux,duringa
trans-fer procedureto treattendinopathy ofthe insertionofthe
calcanealtendon.
Case
report
Thepatientwas a48-year-oldman who presentedchronic
posterioranklepainofprogressivenature,duringandafter
physical activity, even at recreational level, which caused
functional limitation with regard to practicing soccer and
short-distance running. He presented pain upon
palpa-tion at the insertion of the calcaneal tendon and antalgic
gait.
Radiographyshowed calcificationattheinsertionofthe
tendon and magnetic resonance imaging showed
tendi-nosis and partial injury of the tendon at the insertion
of the calcaneal tendon (Fig. 1). After clinical
examina-tion and complementary examinations, the condition was
diagnosed as tendinitis of the insertion of the calcaneal
tendonwithHaglund’sdeformityandsignificantassociated
tendinosis.
After eight months of conservative treatment
compris-ingspecific physiotherapy,hydrotherapyand analgesicand
anti-inflammatorymedications,itwasdecidedtoimplement
surgicaltreatment.Thiswasplannedtoincludetransferofthe
longflexortendonofthehallux,posterosuperiorostectomyof
thecalcaneusanddebridementoftheentiredevascularized
andfibroticregionofthecalcanealtendon.
Thepatientwaspositionedinpronedecubitus,a
tourni-quet was applied at the root of the thigh after spinal
anesthesia,asepsisandantisepsiswereperformedand
ster-ilefieldswereemplaced.Aposteromedialincisionwasmade,
goingfromthemuscle-tendontransitionofthecalcaneal
ten-dontothedistalinsertion,withlateralcurvatureforabetter
approachtotheinsertionandboneexostosis.
Dissection was performed in layers, with rigorous
hemostasis,andthesubcutaneoustissuewaspreserveduntil
theparatendonwasviewed.Aninspectionwasmade,andall
ofthedevitalized,calcified,degeneratedandamorphous
tis-sue atthe insertionofthe calcanealtendonwas debrided.
Posterosuperior ostectomy of the calcaneus was then
per-formeduntiltotaldecompressionofthecalcanealtendonhad
beenachieved.
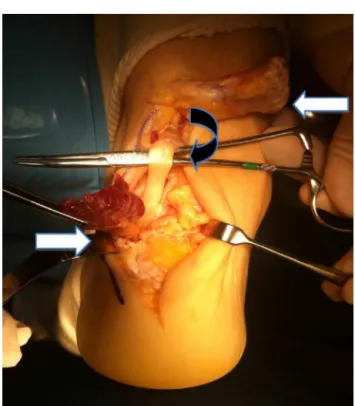
Afterpushingthecalcanealtendonbacksuperiorlywithin
the surgicalexposureafterits deinsertion, it wasobserved
thatananomalousflexortendonwaspresent,superficiallyto
thedeepfascia,withamusclebellygoingfromwhereitwas
viewedproximallyinthesurgicalfieldtowhereitwentbeyond
theankledistallyandacquiredtheshapeofatendon,withits
ownfibrousbonetunnel.
Fromitslocation,itwasidentifiedasananomalous
acces-sorylongflexortendonofthetoes,withanatomicalvariation
suchthatitwasnotindirectcontactwiththe
neurovascu-larbundle.Thistendondidnotpresentanydegenerativeor
fibroticalterationtoitsmorphology.Itwasfoundthrough
sur-gicalexposureanddidnothaveanydirectrelationshipwith
theetiology oftheconditioninquestion(Fig.2).Theentire
lengthoftheanomaloustendonwasthenresected.Thedeep
fasciawasopened,thelongflexorofthehalluxwasisolated
and identified inits tunnel, and tenotomywas performed.
Themaximumtendonlengthwasobtainedandtheankleand
halluxremainedwithmaximumflexion.
Atthisstage,tenodesisofthelongflexorofthehalluxwas
performedatthecalcaneus,usinga7.00mmbioabsorbable
interferencescrewslightly anteriorlytothe previous
inser-tionofthecalcanealtendon,withtheankleat15◦ofequinus.
The debrided calcaneal tendon was reinserted using bone
anchors. Afterclosure of the incision in layers, a dressing
andaplastercastsplintat15◦ofequinuswereapplied.The
patientbeganphysiotherapyafterthreeweeksoffixed
immo-bilization, atwhichtimethiswasexchangedforremovable
immobilization.Partialloadbearingwasauthorizedafterfive
weeks.
Discussion
Fivedifferentanomalousmusclesinthefootandanklehave
beendescribed3,4:intheposterolateralregion,thetendonof
thefourthfibularis;intheposteromedialregion,thetendons
oftheinternalfibulocalcaneal ligament;the longaccessory
flexorofthetoes (quadratusplantae); theinternal
rev bras ortop.2016;51(1):105–108
107
Fig.1–T2magneticresonanceimagingshowing(left)tendinitisoftheinsertionwithdegenerationandtendinosisofthe calcanealtendon;and(right)theaccessoryflexortendonofthetoesatitsmusclebellyisidentifiedthroughthestraight arrowontheleft,whilethelongflexorofthehalluxisalsoidentifiedthroughthearrow.
Anomalousmusclesinthefootandankleusuallydonot
causesymptoms,but insituations ofexcessiveoverloading
suchasamongathletes,thesemusclesmaycausepain,
insta-bility and joint blockade.4,5 Ankle conditions in which the
masseffectofthe accessorytendonscangiveriseto
com-pression and posterior impact of the ankle, tarsal tunnel
syndrome,halluxflexorsyndromeand chronicpain
subse-quenttosprainsmayoccur.3–6
Magneticresonanceimagingexaminationsare
fundamen-talforelucidatingposteriorankleconditions, inidentifying
them,makingdifferentialdiagnoseswithtumorsand
choos-ingthesurgicalroute.3,6,7Theseanomalousmusclesmaynot
beidentifiedeveninmagneticresonanceimaging
examina-tions,iftheradiologistisnotfamiliarwiththelocalanatomy.3
However,whentheyaresymptomatic,thereisusuallyahigher
leveloffluidsinthemusclesheath.3
Throughanatomical studies,accessorylong flexor
mus-clesofthetoes(alsoknownasthelongaccessoryofthelong
flexors,quadratusplantae,Turner’saccessoryorHumphrey’s
secondaccessory)3,8 havebeenfoundtooccurfrequentlyin
othermammals.However,thedifferenceisthatinhumans
theyhavetwoheadsattheirorigin,representingsuccessive
stagesofthe lower pathoftheflexortendonofthehallux
towardtheplantarregionofthefoot,whilethereisasingle
musclebellyinothermammals.Themedialheadisfound
exclusivelyinhumans.9,10
Thisisthesecondmostfrequenttypefoundinanatomical
dissectionsafterthefourthfibularis.6,8 Becauseofproximity
andconsistency inrelationtothe neurovascular bundleof
thetibialnerve,thetibialflexormaycausetarsaltunnel
syn-drome.Itpresentsgreatvariety,bothinitsorigin(tibia,fibula,
interosseousmembraneorlongflexorofthetoes)andinits
108
rev bras ortop.2016;51(1):105–108insertion(longflexorofthetoesatseverallevels,orquadratus
plantae).5–7
Itrunsbelowtheretinacularflexorandhasitsownsheath
and osteofibrous canal, and it usually becomes tendinous
whenitentersthetarsaltunnel.5–7,9Itmaybelateralormedial
tothelongflexorofthehalluxattheleveloftheankleand
inferiortotheneurovascularbundlethatischaracteristically
atitsmusclebelly.Itrunsdistallyandlaterallytotheflexorof
thehallux,suchthatitusuallyhasitsinsertionintheflexor
ofthetoes.7
Thelong flexortendonofthe halluxhasbeenclassified
throughanatomicaldissectionintothreetypes,accordingto
its origin and relationshipwith the bundle9: typeI– origin
in the lower leg and muscle belly superficial to the
bun-dle,without crossingit (type Ia)or withcrossing(type Ib);
typeII–originwithinitsowntarsaltunnel.Thesamestudy
foundthatthemeanlengthwas7cmandmeanwidthwas
9.6mm, and that the tendon part had a mean length of
2.6cm.9
Conclusion
Thepresenceoftheaccessorylongflexormuscleofthetoes
didnotimpedeuseoftheflexortendonofthehalluxfor
trans-ferinacaseoftendinopathyoftheinsertionofthecalcaneus
tendon.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HartogBD.Useofproximalflexorhallucislongustransferin severecalcificachilles’tendinosis.TechFootAnkleSurg. 2002;1(2):145–50.
2.PanchbhaviVK.Chronicachillestendonrepairwithflexor hallucislongustendonharvestedusingaminimallyinvasive technique.TechFootAnkleSurg.2007;6(2):123–9.
3.BestA,GizaE,LinnklaterJ,SullivanM.Posteriorimpingement oftheanklecausedbyanomalousmuscles.JBoneJointSurg Am.2005;87(9):2075–9.
4.KinoshitaM,OkudaR,MorikawaJ,AbeM.Tarsaltunnel associatedwithanaccessorymuscle.FootAnkleInt. 2003;24(2):132–6.
5.EberleCF,MoranB,GleasonT.Theaccesssoryflexor
digitorumlongusasacauseofflexorhallucissyndrome.Foot AnkleInt.2002;23(1):51–5.
6.BowersCA,MendicinoRW,CatanzaritiAR,KernickET.The flexordigitorumaccessoriuslongus–acadavericstudy.JFoot AnkleSurg.2009;48(2):111–5.
7.BuschmannWR,CheungY,JahssMH.Magneticresonance imagingofanomalouslegmuscles:accessorysoleus, peroneusquartusandflexordigitorumlongusaccessorius. FootAnkle.1991;12(2):109–16.
8.PetersenDA,StinsonW,LairmoreJR.Thelongaccessory flexormuscle:ananatomicalstudy.FootAnkleInt. 1995;16(10):637–40.
9.HurMS,WonHS,OhCS,ChungIH,LeeWC,YoonYC. Classificationsystemforflexordigitorumaccessoriuslongus musclevariantswithintheleg:clinicalcorrelations.Clin Anat.2014;27(7):1111–6.