rev bras ortop.2017;52(2):141–147
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Malignant
transformation
in
chronic
osteomyelitis
夽
Diogo
Lino
Moura
∗,
Rui
Ferreira,
António
Garruc¸o
CentroHospitalareUniversitáriodeCoimbra,Coimbra,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6January2016 Accepted6April2016 Availableonline8March2017
Keywords:
Osteomyelitis Malignanttumors Squamouscellcarcinoma Neoplasiccelltransformation
a
b
s
t
r
a
c
t
Introduction:Carcinomatousdegenerationisarareandlatecomplicationdevelopingdecades afterthediagnosisofchronicosteomyelitis.
Objectives: Topresenttheresultsfromaretrospectivestudyofsixcasesofsquamouscell carcinomaarisingfromchronicosteomyelitis.
Methods:Sixcasesofchronicosteomyelitisrelatedtocutaneoussquamouscellcarcinoma wereidentified.Thecauseandcharacteristicsoftheosteomyelitiswereanalyzed,aswellas timeuptomalignancy,thesuspicionsignsformalignancy,thelocalizationandhistological typeofthecancer,andthetypeandresultofthetreatment.
Results:Themeantimebetweenosteomyelitisonsetandthediagnosisofmalignant degen-erationwas49.17years(range:32–65).Thecarcinomaresultedfromtibiaosteomyelitisin fivecasesandfromfemurosteomyelitisinone.Thepathologicalexaminationindicated cutaneoussquamouscellcarcinomainallcases.AllthepatientswerestagedasN0M0, exceptforone,whoselomboaorticlymphnodeswereaffected.Thetreatmentconsisted ofamputationproximaltothetumorinallpatients.Nopatientpresentedsignsoflocal recurrenceandonlyonehadcarcinomametastasis.
Conclusion: Earlydiagnosisandproximalamputationareessentialforprognosisandfinal resultsincarcinomatousdegenerationsecondarytochronicosteomyelitis.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Transformac¸ão
maligna
na
osteomielite
crônica
Palavras-chave:
Osteomielite Tumoresmalignos
Carcinomadecélulasescamosas Transformac¸ãocelularneoplásica
r
e
s
u
m
o
Introduc¸ão: Degenerac¸ãocarcinomatosaéumacomplicac¸ãoraraetardiaquesedesenvolve décadasapósodiagnósticodeosteomielitecrônica.
Objetivos:Apresentarosresultadosdeumestudoretrospectivodeseiscasosdecarcinoma espino-celularemumcontextodeosteomielitecrônica.
夽
StudyconductedattheCentroHospitalareUniversitáriodeCoimbra,Coimbra,Portugal.
∗ Correspondingauthor.
E-mail:[email protected](D.L.Moura).
http://dx.doi.org/10.1016/j.rboe.2017.03.005
142
rev bras ortop.2017;52(2):141–147Métodos: Identificamosseiscasosdecarcinomaespino-celularrelacionadosàosteomielite crônica.Acausaeascaracterísticasdaosteomieliteforamanalisadas,bemcomootempo decorridoatétransformac¸ãomaligna,ossinaisdesuspeitademalignizac¸ão,alocalizac¸ão eotipohistológicodocâncereotipoeosresultadosdotratamento.
Resultados: Otempomédioentreacausadaosteomieliteeodiagnósticodatransformac¸ão malignafoide49,17anos(intervalo:32a65).Ocâncerteveorigememosteomielitesda tíbiaemcincocasoseemumaosteomielitedofêmuremumcaso.Aanálisehistológica demonstroucarcinomaespinocelularcutâneoemtodososcasos.Todosospacientesforam estadiadoscomoN0M0,comexcec¸ãodeum queapresentavaatingimentodosgânglios linfáticoslomboaórticos.Otratamentofoiaamputac¸ãoproximalaotumoremtodosos pacientes.Nenhumdospacientesapresentousinaisderecidivalocaleapenasum desen-volveumetastizac¸ãodocarcinomaespinocelular.
Conclusão: Odiagnósticoprecoceeaamputac¸ãoproximalaotumorsãofundamentaispara oprognósticoeosresultadosfinaisnatransformac¸ãomalignasecundáriaaosteomielite crônica.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Chronicosteomyelitis isalong-lasting andpersistent bone infection caused by complex colonies of microorganisms involved in a matrix of proteins and polysaccharides, the biofilm,which protectsthemfromthe body’simmune sys-temandtheactionofantibiotics.1,2 Thisconditioncanhave
anhematogenousorigin,bycontiguitytoafocusofinfection orbydirectinoculation.1Unlikehematogenous
osteomyeli-tis,the incidenceofosteomyelitiscontiguous toafocus of infectionoriginating fromtrauma, surgery,orimplants has increased.3
Non-treatmentofacuteosteomyelitis,ortreatmentfailure, associatedwithimportantlesionsofthesurroundingsoft tis-sues,poorbonevascularization,systemicinvolvement,and multipleandresistantmicroorganismsleadstoachronicand refractoryboneinfection,whoseconstantinflammatory activ-itycausesbonedestructionandmayfavorthedevelopment ofneoplasias.1,3 Theincidenceofmalignanttransformation
inthesettingofchronicosteomyelitisisverylowin devel-opedcountries; nonetheless,itremainsamajorproblemin countrieswithpoorhealthcare.1
Parasiticinfectionanditseffectonstemcellsignalingis oneoftheoldesttheoriesofcancerorigin.4,5Currently,itis
acceptedthattheassociationofchronicinfectionand develop-mentofmalignanciesmaybeunderestimated.5Someauthors
acknowledge that over 25% of malignant neoplasms may originatefrom chronicinflammationandinfectiousagents. Thereisaconsiderablebodyofevidenceforsomeofthese associations,suchasbetween Salmonellatyphi and hepato-biliarycarcinoma;OpisthorchisviverriniandClonorchissinensis
andcholangiocarcinoma;Schistosomahematobiumandbladder cancer;andbetweenhidradenitissuppurativaandcutaneous squamouscellcarcinoma,amongothers.5,6
The exact mechanism of malignant transformation remains unknown. It is assumed that, in a multifactorial manner, the chronicinflammatorystate behavesas a pro-moterinthecomplexprocessofcarcinogenesis.1,6Malignant
transformation begins inthe skinor epithelium ofthe fis-tula and infiltrate the adjacent tissues, including bone.7,8
The prevalenceofmalignant transformation in the setting of chronicosteomyelitis ranges from 1.6%to 23%,and the most commonly affected bones are the tibia and femur. Themost frequentlyobserved malignant transformationis squamouscell carcinomaoftheskin.1,5,9,10 Theincreasein
fistulous drainage,aswellaspersistence,exophytic growth of an ulcer or mass can be warning signs for malignant transformation.1,11Allpatientswithulcersandfistulas
asso-ciatedwithchronicosteomyelitis shouldbefrequently and carefully followed-up, and any characteristicalterations in a chronic wound should raise the suspicion of malignant transformation.8,12 Diagnosisisconfirmedthroughbiopsies,
which shouldbeperformed earlyinmultiplelocations and depths, including ulcers, fistulas, and bone, in order to increasediagnosticaccuracyandreducethenumberoffalse negatives.10,12,13 When malignant transformation is
diag-nosed,itisessentialtostagetheneoplastic diseaseandto assessthepresenceofdistantmetastasesthroughstudiesby computerizedtomography,magneticresonanceimaging,and positronemissiontomography.12
The definitive and most frequently used surgical treat-ment inthese situations, considering that the majority of patientshaveadvanceddisease,istheproximalamputation oftheneoplasia.7,10Adjuvantchemoradiotherapyisindicated
in metastaticdisease and high-gradetumors.14 In selected
patients withoutmetastaticdisease,limb-sparingextended tumorexcisionwithlimbsalvagemaybechosen.1
The main prognostic factor is the staging of the neo-plastic disease.8,10 In most cases, chronic osteomyelitis in
squamous cell carcinomas is aggressive, with high levels of local recurrence and metastasis. Metastasis is observed early(in mostcases,inthefirst 18monthsaftermalignant transformation)andismainlylocatedinthelymphnodes.15
However,ifthepatientdoesnotpresent metastaticdisease duringthe firstthree yearsand thetumorlesion hasbeen excised correctly, prognosis is favorable.15 Early diagnosis
rev bras ortop.2017;52(2):141–147
143
Fig.1–PatientLMM.(A)Radiographywithsignsofchronicosteomyelitisofthetibia;(B)Malignanttransformationofulcer intosquamouscellcarcinoma.
chronicosteomyelitisare criticaltothe prognosisandfinal results.1Themosteffectivemethodofpreventingtheonset
ofthesemalignanciesisappropriateanddefinitivetreatment ofchronicosteomyelitis,debridement,andantibiotictherapy.
Material
and
methods
Aretrospectiveanalysisofpatientsdiagnosedwithmalignant transformationinchronicosteomyelitiswasperformed.The evaluationwasmadethroughtheclinical recordsand con-sistedofananalysisoftheetiologyofchronicosteomyelitis anditscharacteristics,timeelapseduntildiagnosisof malig-nant transformation and reasons that led toits diagnosis, cancerlocationandhistologicaltype,andsurgicaltreatment performedanditsresults.
Results
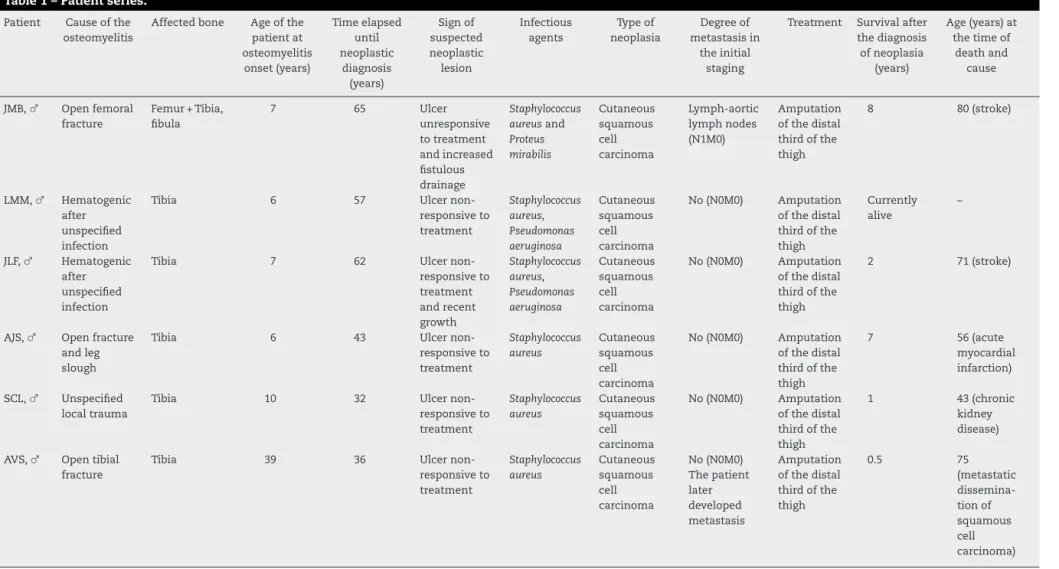
Theauthorspresentaseriesofsixpatientsdiagnosedwith malignanttransformationofchronicosteomyelitis(Table1). Allpatientsweremale.Itwasobservedthat,intwothirdsof thesample,chronicosteomyelitisoriginatedfromatrauma that had occurred at an early age, while the other third wasassociated withahematogenous cause resulting from unspecified childhood infections. All traumatic causes of osteomyelitiswereopenfracturesofthelowerlimb,withthe exceptionofonepatientwhosetraumacouldnotbe ascer-tained.Forallpatients,thelegwastheaffectedanatomical site,andthetibiawasthemostaffectedbone.Inonepatient, althoughosteomyelitis reachedthe legbones, it had origi-natedfromanopenfractureofthefemur;patientdeveloped alatechroniculcerinthelegthatlaterbecame malignant. In83.33%ofthepatients,thecauseofosteomyelitisoccurred inchildhood,whileonepatienthadtheinitialtraumaat39 yearsofage.Inallpatients,theevolutionfromosteomyelitis
tomalignancyoccurredoverdecades,withameanintervalof 49.17years(minimumof32andmaximumof65).
The persistent presenceof achronic ulcer was the red flag sign forall patientsin this series. Other signs of sus-pectedmalignanttransformationwerealsoidentified:inone patient,therewasalsoanincreaseintheintensityof puru-lentfistulousdrainage;inanother,arecentincreaseinulcer dimensions(Figs.1–4).Staphylococcusaureuswasdetectedinall microbiologicalanalyses,Pseudomonasaeruginosawaspresent intwopatients,andProteusmirabilisinonepatient. Pathologi-caltibialfracture,whichisoneofthecomplicationsofchronic osteomyelitis,wasalsoobservedintwopatients(Fig.4).
Cutaneoussquamouscellcarcinomawasthetypeof neo-plasiaobservedinall thepatientsinthesample.In83.33% ofthepatients,nosignsofmetastasisweredetected;inturn, onepatientpresentedimagingdatasuggestinglumbar-aortic lymphnodeinvolvement.Althoughtheinitialstaging corre-sponded toN0M0, alyticlesion inthe proximalportionof thecontralateralfemurwasobservedinonepatientafterfive months,andlaterwasdiagnosedasametastasisoriginating insquamouscellcarcinoma.
Thetherapeutic choiceforall patients was limb ampu-tationsurgery,notablyamputationofthedistalthirdofthe thigh.Inthepatientwithchronicosteomyelitisofthefemur andinvasionofthelumbar-aorticlymphnodes, disarticula-tion ofthehipandthe necessarylymphadenectomywould requireahemipelvectomy.However,duetotheinherentrisks ofthissurgeryandthedifficultytoachieveskincoverage,the authorsdecidedagainstit,andthusapalliativeamputation wasperformedthroughthedistalthirdofthethigh.Noneof thepatientsdevelopedlocalrecurrence.
144
r e v b r a s o r t o p . 2 0 1 7; 5 2(2) :141–147Table1–Patientseries.
Patient Causeofthe osteomyelitis
Affectedbone Ageofthe patientat osteomyelitis onset(years) Timeelapsed until neoplastic diagnosis (years) Signof suspected neoplastic lesion Infectious agents Typeof neoplasia Degreeof metastasisin theinitial staging
Treatment Survivalafter thediagnosis ofneoplasia
(years)
Age(years)at thetimeof
deathand cause
JMB,♂ Openfemoral fracture
Femur+Tibia, fibula
7 65 Ulcer unresponsive totreatment andincreased fistulous drainage Staphylococcus aureusand Proteus mirabilis Cutaneous squamous cell carcinoma Lymph-aortic lymphnodes (N1M0) Amputation ofthedistal thirdofthe thigh
8 80(stroke)
LMM,♂ Hematogenic after unspecified infection
Tibia 6 57 Ulcer non-responsiveto treatment Staphylococcus aureus, Pseudomonas aeruginosa Cutaneous squamous cell carcinoma
No(N0M0) Amputation ofthedistal thirdofthe thigh
Currently alive
–
JLF,♂ Hematogenic after unspecified infection
Tibia 7 62 Ulcer non-responsiveto treatment andrecent growth Staphylococcus aureus, Pseudomonas aeruginosa Cutaneous squamous cell carcinoma
No(N0M0) Amputation ofthedistal thirdofthe thigh
2 71(stroke)
AJS,♂ Openfracture andleg slough
Tibia 6 43 Ulcer non-responsiveto treatment Staphylococcus aureus Cutaneous squamous cell carcinoma
No(N0M0) Amputation ofthedistal thirdofthe thigh
7 56(acute myocardial infarction)
SCL,♂ Unspecified localtrauma
Tibia 10 32 Ulcer non-responsiveto treatment Staphylococcus aureus Cutaneous squamous cell carcinoma
No(N0M0) Amputation ofthedistal thirdofthe thigh
1 43(chronic kidney disease)
AVS,♂ Opentibial fracture
rev bras ortop.2017;52(2):141–147
145
Fig.2–PatientJLF.(A)Radiographywithsignsofchronic osteomyelitisofthetibia;(B)Malignanttransformationof ulcerintosquamouscellcarcinoma.
maximumofsixyears.Thepatientwithconcomitantchronic osteomyelitisofthefemurpresentedinfectionofthe ampu-tationstump,whichrequiredsurgicalcleaningofthefemur (Fig.5).
Discussion
StudiesintheEnglishliteratureonmalignanttransformation inthesettingofchronicosteomyelitisarescarce,consisting primarilyofisolated clinicalcases.1 Onlytwoarticleswere
caseseries:onewithsixandanotherwithsevenpatients.1,7,10
Therefore, this seriesisoneofthe firsttoanalyze aseries ofpatientsdiagnosedwithmalignanttransformationinthe contextofchronicosteomyelitis.
The prevalence of males is in agreement with the literature.1 In the present series, most cases of chronic
osteomyelitishadtraumaastheircause.Traumaremainsthe mostfrequentcause ofosteomyelitis;openfracturesofthe longbonesareassociatedwithinfectionratesof4–64%and infectionrecurrenceratesof20–30%.9,10,16,17 Thetibiaisthe
mostcommonlyaffectedbone,followedbythefemur,which isinlinewiththefindingsfromotherseries.1,5,9,10
Studies inthis area demonstrated that the presenceof chronic osteomyelitiswithyears ordecades ofevolutionis themostimportantfactorformalignanttransformation;the interval from osteomyelitisdiagnosis tomalignancyranges from18to72years.1,10,12Inallpatientsinthissample,an
inter-valofdecadeswasobservedbetweenosteomyelitisdiagnosis anddevelopmentofmalignancy.Themainsignofsuspected malignant transformationwas thepersistence ofanatonic ulcerthatdidnotrespondtotreatment,followedbyarecent enlargementoftheulcerandincreaseddrainage.Themost frequentsymptomsthatraisesuspicionofmalignant trans-formationareincreaseddrainage,lackoflesionimprovement
146
rev bras ortop.2017;52(2):141–147Fig.4–PatientAVS.(A)Radiographywithsignsofchronictibialosteomyelitis,pathologicalfracture;(B)Non-consolidation aftersixweeks;(C)Malignanttransformationofulcerintosquamouscellcarcinoma.
afterthree months of treatment, followed by increasedor exophyticlesion,erythema,hemorrhage,lymphadenopathy and,lessfrequently,hyperkalemia,weightloss,anorexia,and hyperpigmentation ofthe surrounding skin.1 In agreement
withotherstudies,S.aureuswasthemostfrequentlydetected microorganism.1Themostfrequentlyobservedmalignancyin
chronicosteomyelitisiscutaneoussquamouscellcarcinoma, whichwastheonlyneoplastichistologicaltypeidentifiedin thepresentstudy.1,5,9,10
Asmentioned in the introduction,squamous cell carci-nomas in the context of chronic osteomyelitis are usually
aggressiveandhavehighlevelsoflocalrecurrenceandearly metastasis.15Despitethesedata,inthepresentstudy,tumors
showed nosignalsofmetastatic diseaseatthe momentof diagnosis in83.3%(n=5)ofpatients.All sixpatientsinthe studybyAlamietal.7werestagedasN0M0.Incontrast,out
of the sevenpatients in the study by Altayet al.,10 three
were at the N0M0stage; two,N1M0; one, N1M1; the other diedpriortothestaging.Oneofthepatientsinthepresent study,stagedasN0M0,developedbonemetastaseswithinfive months.Thesedatapointtotheneedforvigilanceand assid-uous monitoring ofthese cases, including those staged as
rev bras ortop.2017;52(2):141–147
147
N0M0,duetotheprecocityandrapidityofmetastatic dissem-ination.
Amputationproximaltothelesionisasurgicaltreatment thatresolvesnotonlytheneoplasticlesionbutalsothechronic osteomyelitis;itisthegoldstandardformalignant transfor-mationsofosteomyelitis.In allpatients ofthissample, an amputation wasperformed through the distalthird ofthe thigh;nocasesoflocalrecurrencewereobserved.Mean sur-vivalafterdiagnosisoftheneoplasiawasonly3.8years.This canbeexplainedbythefactthatfourofthefivepatientsdied duetootherassociateddiseases,notduetomalignancyof osteomyelitisortothesurgicalprocedureperformed(Table1). Interestingly,thepatientwiththelongestsurvival(eightyears) wastheonewhounderwentpalliativeamputationthrough thethighandwhopresentedconcomitantchronic osteomyeli-tis ofthe femuras wellas suspectedlumbar-aortic lymph nodeinvolvement.Theneedforregionallymphadenectomy remains controversial, asthe increase inlymph node size isoftenonlyreactivetoinflammation.10However,itisnow
thoughtthatifthesignsoflymphadenopathypersistsixto12 weeksafteramputation,theirsurgicalremovalisrequired.10,11
Intheaforementionedcase,thelumbar-aorticadenopathies wereprobablyreactive,ratherthancausedbymetastatic dis-ease,allowingthepatienttosurviveforeightyearsafterthe diagnosisofsquamouscellcarcinoma.
Conclusion
Malignanttransformationisarareandlatecomplicationof chronicosteomyelitis,whoseclinicalsignsofsuspicionmust beidentifiedearly.Earlydiagnosisbymeansofbiopsiesand aggressivetreatmentoftheselesionsarefundamentalforthe prognosisandfinalresults.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. PanteliM,PuttaswamaiahR,LowenbergDW,GiannoudisPV. Malignanttransformationinchronicosteomyelitis:
recognitionandprinciplesofmanagement.JAmAcadOrthop Surg.2014;22(9):586–94.
2.ForsbergJA,PotterBK,CiernyG3rd,WebbL.Diagnosisand managementofchronicinfection.JAmAcadOrthopSurg. 2011;19Suppl.1:S8–19.
3.LewDP,WaldvogelFA.Osteomyelitis.Lancet. 2004;364(9431):369–79.
4.SellS.Infection,stemcells,andcancersignals.CurrPharm Biotechnol.2011;12(2):182–8.
5.SamarasV,RafailidisPI,MourtzoukouEG,PeppasG,Falagas ME.Chronicbacterialandparasiticinfectionsandcancer:a review.JInfectDevCtries.2010;4(5):267–81.
6.MulthoffG,MollsM,RadonsJ.Chronicinflammationin cancerdevelopment.FrontImmunol.2012;2:98.
7.AlamiM,MahfoudM,ElBardouniA,BerradaMS,ElYaacoubi M.Squamouscellcarcinomaarisingfromchronic
osteomyelitis.ActaOrthopTraumatolTurc.2011;45(3): 144–8.
8.WolfH,PlatzerP,VécseiV.Verrucouscarcinomaofthetibia arisingafterchronicosteomyelitis:acasereport.WienKlin Wochenschr.2009;121(1–2):53–6.
9.McGroryJE,PritchardDJ,UnniKK,IlstrupD,RowlandCM. Malignantlesionsarisinginchronicosteomyelitis.Clin OrthopRelatRes.1999;(362):181–9.
10.AltayM,ArikanM,YildizY,SaglikY.Squamouscell
carcinomaarisinginchronicosteomyelitisinfootandankle. FootAnkleInt.2004;25(11):805–9.
11.TrentJT,KirsnerRS.Woundsandmalignancy.AdvSkin WoundCare.2003;16(1):31–4.
12.OgawaB,ChenM,MargolisJ,SchillerFJ,SchnallSB.Marjolin’s ulcerarisingattheelbow:acasereportandliteraturereview. Hand(NY).2006;1(2):89–93.
13.PandeyM,KumarP,KhannaAK.Marjolin’sulcerassociated withchronicosteomyelitis.JWoundCare.2009;18(12): 504–6.
14.PuriA,ParasnisAS,UdupaKV,DuggalA,AgarwalMG. Fibroblasticosteosarcomaarisinginchronicosteomyelitis. ClinRadiol.2003;58(2):170–2.
15.RauhMA,DuquinTR,McGrathBE,MindellER.Spreadof squamouscellcarcinomafromthethumbtothesmallfinger viatheflexortendonsheaths.JHandSurgAm.
2009;34(9):1709–13.
16.LazzariniL,MaderJT,CalhounJH.Osteomyelitisinlong bones.JBoneJointSurgAm.2004;86(10):2305–18.