Arq. Bras. Cardiol. vol.77 número5
Texto
Imagem
Documentos relacionados
Smoking was the major factor associated with intermittent claudi- cation, and the elderly with intermittent claudication had a tendency toward a higher frequency of
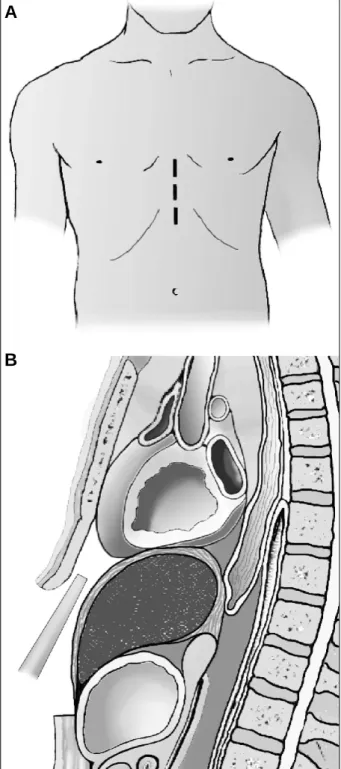
Fig. 2 - Case 2 - A and B) right ventriculography in cranial posteroanterior and left profile views: Note mild to moderate right ventricular hypoplasia with attenuation of
In the present case, in addition to the lack of a report in the medical literature about the association of these di- seases, this being probably the first case ever reported, the
1 - Radiografia de tórax mostrando área cardíaca normal, sinais de aumento atrial direito, trama vascular pulmonar diminuída, principalmente à esquerda, e hipoplasia do
Even though no difference existed in total mortality in 30 days (9.8% myocardial revascularization surgery vs 11.2% aortic valvular replacement and myocardial revasculariza-
Na Correlação Anatomoclínica publicada em Arq Bras Cardiol, vol 80 (nº 6), 643-8, 2003, as figuras dos eletrocardiogramas foram trocadas. Eis
No artigo Tratamento cirúrgico da coartação da aorta pela aortoplastia trapezoidal de Jarbas Dinkhuysen e cols., publicado em Arq Bras Cardiol 2004; 82: 9-17, foi omitida,
With respect to the article “Catheter Ablation of Atrial Fibrillation – Techniques and Results”, published in the October 2005 edition (Arq Bras Cardiol. 2005;85:295- 301), the
