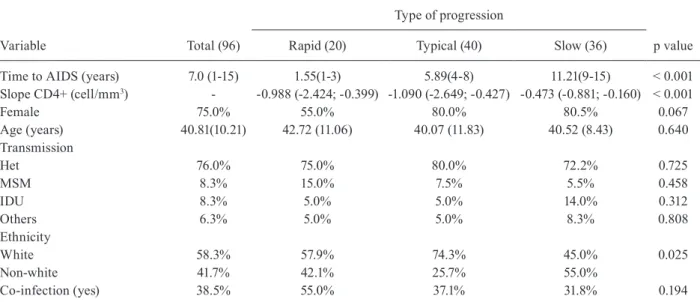
Association of NR1I2 gene polymorphisms and time of progression to AIDS
Texto
Imagem
Documentos relacionados
The probability of attending school four our group of interest in this region increased by 6.5 percentage points after the expansion of the Bolsa Família program in 2007 and
The aim of this study was to anal- yse the prevalence of HPV infection and the distribution of HPV types and HPV16 genetic variants in HIV-neg- ative and HIV-positive women with
Observations on the ecology of silvatic Triatominae are still fragmentary, principally because target species in control process are almost exclusively domestic.. Report of
Conclusions: Because of the limitations of this meta-analysis due to the small number of ran- domized clinical trials and patients included, the results should be taken cautiously,
This report is part of MAPLE Project, ERC – European Research Council Grant, 682125, which aims to study the Politicisation of the EU before and after the
Of the limitations of our study, we highlight the small number of patients assessed and the lack of quadripolar LV leads, which increase the likelihood of LV resynchronization
Some limitations of the present study must be mentioned. In function on the cross-sectional design, the main limitation of the study is the possible reverse causality bias in
Se quiséssemos um resultado mais preciso, preci- saríamos estudar as características de cada atleta em par- ticular: quão intensa é a força que consegue fazer quando há
