jcoloproctol(rioj).2016;36(2):115–118
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
Report
Granular
cell
tumor
of
anal
border
Angelo
Fontes
Araújo
a,∗,
Igor
Blohem
Vasconcelos
a,
Jadeilton
Jipso
de
Souza
Dias
a,
Luciano
Santana
de
Miranda
Ferreira
a,
Rodrigo
Guimarães
Andrade
b,
Paulo
César
Boente
Santos
aaCentrodeOncologiaeHematologiadaBahia(CEHON),Salvador,BA,Brazil bLaboratórioStudart&Studart(LSS),Salvador,BA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received3March2015 Accepted3March2015 Availableonline22March2016
Keywords:
Analcanal Granularcelltumor Neoplasms Casereports
a
b
s
t
r
a
c
t
Theobjectiveofthisreportistodescribeacaseofgranularcelltumoroftheanalborderand toreviewthemostrelevanttopicsoftheliteratureonthesubject.Oursisafemalepatient,57 yearsold,withanasymptomaticnoduleintheanalborderfor2years.Surgicalexcisionwas performed,withahistopathologicaldiagnosisofgranularcelltumor.Thefirstdescriptionof thistumorwascarriedoutin1926byAbrikossoff.Thetechniquesofimmunohistochemistry andelectronmicroscopyallowedustodetermineitsorigininSchwanncells.Thesearerare tumors,mostoftendiagnosedbetweenthe4thand6thdecadeoflifeand,ingeneral,are benignformations–only2%ofthemaremalignant.Thesetumorscanoccurinanypartof thebody,althoughtheyaremorecommonintheoralmucosa,dermisandsubcutaneous tissue.Thetreatmentsolelybysurgeryhasacurativeeffect,anditsrecurrenceisunusual. Thelocationintheanal/perianalareaoccursevenmorerarely,andwefoundonly48cases previouslydescribedintheliterature.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Tumor
de
células
granulares
de
borda
anal
Palavras-chave:
Canalanal
Tumordecélulasgranulares Neoplasias
Relatosdecasos
r
e
s
u
m
o
O objetivodeste relato é descreverum caso de tumor de células granulares de borda analerevisarostópicosmaisrelevantesdaliteraturaacercadotema. Trata-sedeuma pacientedosexofeminino,57anos,comhistóricodenódulonabordaanalassintomático há2anos.Foirealizadaressecc¸ãocirúrgicadalesão,comdiagnósticohistopatológicode tumordecélulasgranulares.Aprimeiradescric¸ãodestetumorfoiem1926por Abrikos-soff.Astécnicasdeimunohistoquímicaedemicroscopiaeletrônicapermitiramdeterminar asuaorigemnascélulasdeSchwann.Sãotumoresraros,maisfrequentesentrea4a
e6a décadadevidae,nogeral,benignos,apenas2%sãomalignos.Podemocorrerem qual-querpartedocorpo,emborasejammaiscomunsnamucosabucal,dermeetecidocelular
∗ Correspondingauthor.
E-mail:[email protected](A.F.Araújo).
http://dx.doi.org/10.1016/j.jcol.2015.03.004
116
jcoloproctol(rioj).2016;36(2):115–118subcutâneo. O tratamento cirúrgico isolado é curativo e a recorrência incomum. A localizac¸ãonoânus/canalanal/perianaléaindamaisrara,sendoencontradosapenas48 casospreviamentedescritosnaliteratura.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este éumartigoOpenAccesssobalicençadeCCBY-NC-ND
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The first histopathological description of the granular cell tumorwasperformedin1926byAbrikossof.Thesearerare tumors,predominantlybenign.Theoccurrenceofmalignant granularcelltumorsbarelyreaches2%,requiringobservation ofhistologicalfeaturesofmalignancyandevidenceof metas-tasesforitsdiagnosis.1,2
Thesetumorscanshowawidedistributionthroughoutthe body,althoughthemostaffectedareasarethebuccalmucosa, dermis and subcutaneous tissue. Granular cell tumors are morefrequentbetweenthe 4th and 6th decade oflife.3 In mostcaseseries, thetumorprevailsamongmales,ranging from64.5%to68%.2,4 Isolatedsurgicaltreatmentiscurative anditsrecurrenceisunusualandasageneralruleoccursin thesamelocal,beingassociatedwithanincompleteresection oftheprimarylesion.2–4
Herewereportthecaseofagranularcelltumoroftheanal marginanddiscussthemostrelevantaspectsofliteratureand thosepresentedbythiscase.
Case
report
Femalepatient,57yearsold,Africandescent,teacher, mar-ried.Apreviouslyhealthypatientwithoutclinicalandsurgical comorbiditiesandnorelevantfamilyhistory;complainedof anasymptomaticnodulelocatedintheanalmarginforabout twoyears.She deniedchanges in herbowel habits and in characteristicsofevacuations.On examination,ahardened perianalformationmeasuringabout2cm,inthe5.00o’clock position,wasobserved.
Surgical excision was indicated. Preoperative evaluation with colonoscopy, chest X-ray and laboratory tests found no abnormalities.Thus, the entiremacroscopiclesion was resectedatsurgery.
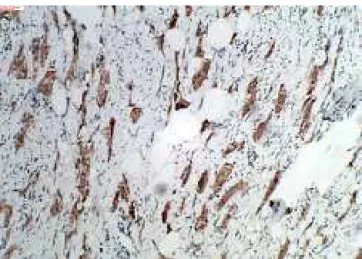
In the macroscopic pathology, two surgical frag-ments of mucosa, with 3.2cm×1.3cm×1.6cm and 1.3cm×0.7cm×0.4cm,respectively,wereevaluatedtogether. Themicroscopyrevealedananalmucosalinedbystratified squamous epithelium without atypia, displaying typical irregular acanthosis featuresin the epithelium adjacent to thetumor.Inthecorium,wefoundcellproliferationwitha largeand granular cytoplasm,with regular nuclei, forming small groups amid intense fibrosis (Figs. 1 and 2). There wasno necrosisor significantmitotic activity.Theprocess wascompromisingtheadjacentadipose tissueandskeletal muscle,inadditiontolateralanddeepsurgicalmargins.The immunohistochemistrywaspositiveintheneoplasticcellsto S100,CD68(Figs.3and4),neuralspecificenolase,inhibinand calretinin;andnegativeforpan-cytokeratin(AE1andAE3).
Fig.1–Tumorcells,lowmagnification,hematoxylin-eosin staining(40×).
Imaging studies (abdominal computed tomography and magneticresonanceimagingofthepelvis)carriedoutafter surgeryshowedonlypostoperativechangesintheanalarea.
Discussion
Virtually,granularcelltumorscanoccur inanyanatomical location,andalthoughmorecasesarelocatedintheskinand subcutaneoustissue,thetongueissinglythemostcommon site.In5–8.5%ofthecases,thetumorsaremultiple.Rarely theseformationsarediagnosedbeforethesurgicalexcision orwhenobtainingabiopsyofsuspiciouslesions.2,4,5
Thepresence ofthis tumorinthe gastrointestinal tract variesfrom5%to19%.2,4 Amongthetumorsoftheperianal
jcoloproctol(rioj).2016;36(2):115–118
117
Fig.3–Immunohistochemistry:groupsofpositivetumor cellsforS100protein(100×).
region,theremayberectalbleeding;butmostofthempresent aspainfulnodulesthatmaybeconfusedwithabscess.Many oftheseformationsarediagnosedincidentallyduringan eval-uationofotherchanges,suchashemorrhoidsandperianal fissures.6,7
Amongthedescribedhistopathologicalfeatures,onecan highlightthe positivityinimmunohistochemistryforS-100 proteinand CD-68.TheS-100 proteinisexpressed in vari-oustumors(neural tumors,melanomas, sarcomas ofclear cells,histiocytosis,andothers),andthepositivity,inthecase herepresented,supportsthe neuraloriginofthelesion,as it is currently accepted in the literature. Despite this ori-gin,thetumorcellssharemanymorphologicalandstructural characteristicsofmacrophages;thus,thesecellsarepositive forCD-68,amacrophage/histiocyticmarkerpar excellence. Anotherimportantaspectisthefrequentassociationofthese tumorswithsomedegreeofpseudoepitheliomatous hyper-plasiaoftheoverlyingepithelium,whichcanbeaconfounding factorwithsquamouscellcarcinoma.4,6
Malignantgranularcelltumorsare rare (2% ofcases).1,2 Some histological characteristics favoring the diagnosis of malignancyare:thepresenceofnecrosis,avesicularnucleus with anobvious nucleolus (in benign tumors, the nucleus
Fig.4–Groupsofpositivetumorcellsin immunohistochemistryforCD-68(100×).
ispyknotic),atrendfortheformationofspindlecells,and some mitoticactivity. Someauthors suggest the classifica-tionoftumorsinthosewithuncertainmalignantpotential, if these formations have any of the above characteristics, besidesfavoringamorerigorousclinical follow-upand the surveyforoccultmetastases.1
Malignanttumorsaffect(morethanbenigntumors)deep softtissues,esophagus,larynx,peritonealcavityand periph-eralnerves.Themajormetastaticsitesarelymphnodes(70%) andlung(50%).Malignantvariantshaveanaggressive behav-ior,witharateoflocalrecurrenceof70%,andresultindeath in65%ofcasesafteranaverageof2.5yearsafterdiagnosis. Amongthedifferentialdiagnosesofmalignantgranularcell tumors,alveolarsofttissuesarcomaandrhabdomyosarcoma canbeparticularlycitedand,lesscommonly, dermatofibrosar-coma,malignantfibroushistiocytomaandmelanoma.1
Literature
series
Lebranchuetal.publishedthelargestseriesofgranularcell tumors, with263 cases,of which15 were multiple and 12 wereassociatedwithmalignanciesofotherhistological fea-tures,butwithnocasesofmalignantgranularcell.Therewas onlyonecaseofrecurrenceafteranincompleteresection.Men wereaffectedin68%ofthetimeandthemainsiteswere:skin (38%),esophagus(19%)andtongue(10%).Ninecasesoccurred inthedigestivetract(21.03%oftotal)andonly1intherectum
and1intheanus2(Table1).
Lacketal.reviewed118tumorsin110patientsandfound ahigherprevalenceofAfricandescent(29%)patients,64.5% inmen,44%locatedintheskinandsubcutaneoustissue.The predominanceofmenwasattributedtoapossibleselection biasofpatientswhocamefrommilitaryhospitals.Onlysix cases were locatedin the rectum/anus, which isthe most commonsiteinthegastrointestinaltract,followedby esoph-agus(2cases) andstomach(1case) (Table1).Inthis series, recurrencewas8%;andinallcases,thesurgicalmarginwas compromisedinthefirstresection.However,theabsenceof recurrencewasnumericallyhigher,evenincaseswitha pos-itivesurgicalmargin.4
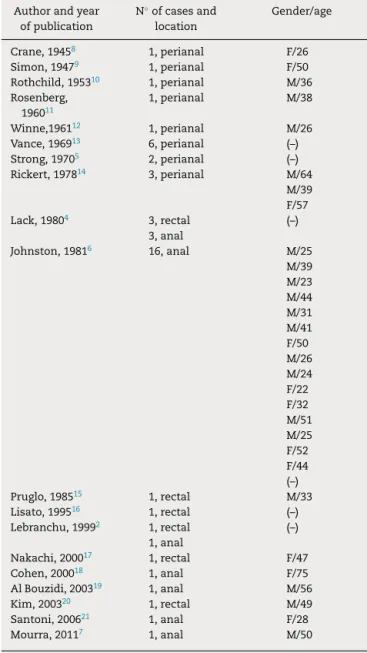
Thelargestnumberoftumorsintheperianalregionwas reportedinaseriesonlyofthegastrointestinaltract:16cases inatotalof74.Intotal,only48casesofgranularcelltumors intheperianalregionhavebeendescribedintheliterature, highlightingthescarcityofthetumorinthissite.Amongthese cases,63.3%(19/30)occurredinmalesubjects,andthemean andmedianageswere40.9yearsand39years,respectively6
(Table1).
118
jcoloproctol(rioj).2016;36(2):115–118Table1–Descriptionofcasesofgranularcelltumors locatedintherectum/analcanalintheliterature.
Authorandyear ofpublication
N◦ofcasesand
location
Gender/age
Crane,19458 1,perianal F/26
Simon,19479 1,perianal F/50
Rothchild,195310 1,perianal M/36 Rosenberg,
196011
1,perianal M/38
Winne,196112 1,perianal M/26
Vance,196913 6,perianal (–) Strong,19705 2,perianal (–) Rickert,197814 3,perianal M/64
M/39 F/57 Lack,19804 3,rectal
3,anal
(–)
Johnston,19816 16,anal M/25
M/39 M/23 M/44 M/31 M/41 F/50 M/26 M/24 F/22 F/32 M/51 M/25 F/52 F/44 (–)
Pruglo,198515 1,rectal M/33
Lisato,199516 1,rectal (–)
Lebranchu,19992 1,rectal 1,anal
(–)
Nakachi,200017 1,rectal F/47
Cohen,200018 1,anal F/75
AlBouzidi,200319 1,anal M/56
Kim,200320 1,rectal M/49
Santoni,200621 1,anal F/28
Mourra,20117 1,anal M/50
(–),informationnotavailable;M,male;F,female.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. JardinesL,CheungL,LiVolsiV,HendricksonS,BrooksJJ.
Malignantgranularcelltumors:reportofacaseandreviewof
theliterature.Surgery.1994;116:49–54.
2.LebranchuVB,AssociationSeptentrionaledesACP.Latumeur
àcellulesgranuleuses.Épidémiologiede263cas.ClinExp
Pathol.1999;47:26–30.
3.DupuisC,CoardKCM.Areviewofgranularcelltumoursat
theuniversityhospitaloftheWestIndies:1965–2006.West
IndianMedJ.2009;58:138–41.
4.LackEE,WorshamGF,CallihanMD,CrawfordBE,ChunB,
KlappenbachS,etal.Granularcelltumor:aclinicopathologic
studyof110patients.JSurgOncol.1980;13:
301–16.
5.StrongEW,McDivittRW,BrashfieldRD.Granularcell
myoblastoma.Cancer.1970;25:415–522.
6.JohnstonMJ,HelwigEB.Granularcelltumorsofthe
gastrointestinaltractandperianalregion:astudyof74cases.
DigDisSci.1981;26:807–16.
7.MourraN,WerbrouckA,BauerP.Analregion:anunusual
locationofgranularcelltumour.IntJColorectalDis.
2011;26:811–2.
8.CraneAR,TremblayRG.Myoblastoma(granularcell
myoblastomaormyoblasticmyoma).AmJPathol.
1945;21:357–75.
9.SimonMA.Granularcellmyoblastoma(myoblasticmyoma,
rhabdomyomegranulo-cellulaire).AmJClinPathol.
1947;17:302–13.
10.RothchildTP,CraryRH.Granularcellmyoblastoma:areport
offivecases.AnnSurg.1953;137:530–8.
11.RosenbergI.Perianalgranularcellmyoblastoma:reportofa
case.JIntCollSurg.1960;33:346–9.
12.WinneBE,BaconHE.Myoblastomaoftheanalcanal.Dis
ColonRectum.1961;4:206–14.
13.VanceSF,HudsonRP.Granularcellmyoblastoma:
clinicopathologicalstudyofforty-twopatients.AmJPathol.
1969;52:208–11.
14.RickertRR,HarkeyIG,KantorEB.Granularcelltumors
(myoblastomas)oftheanalregion.DisColonRectum.
1978;21:413–7.
15.PrugluIuV,Krasil’shchukDZ,SivtsovaNL,DorofeevVI.
Granular-celltumoroftherectum.ArkhPatol.1985;47:
74–7.
16.LisatoL,BianchiniE,RealeD.Granularcelltumorofthe
rectum:descriptionofacasewithunusualhistological
features.Pathologica.1995;87:175–8.
17.NakachiA,MiyazatoH,OshiroT,ShimojiH,ShiraishiM,Muto
Y.Granularcelltumoroftherectum:acasereportandreview
oftheliterature.JGastroenterol.2000;35:631–4.
18.CohenMG,GreenwaldML,GarbusJE,ZagerJS.Granularcell
tumor–auniqueneoplasmoftheinternalanalsphincter:
reportofacase.DisColonRectum.2000;43:
1444–6.
19.AlBouzidiA,ChohoK,CherradiN,RimaniM,HarketA,
AmartiRiffiA,etal.Tumeuranalebénigneàcellules
granuleuses.PresseMed.2003;32:221–2.
20.KimDH,KimYH,KwonNH,SongBG,JungJH,KimMH,etal.
Acaseofgranularcelltumorintherectum.KoreanJ
GastrointestEndosc.2003;27:88–91.
21.SantoniBALM,PintoFES,MachadoL,FerrazED,CuetoGGD,
SallesRC,etal.TumordeCélulasGranularesnoCanalAnal:
RelatodeCasoeRevisãodeLiteratura.RevBrasColoproctol.