2011 Mar-Apr;19(2):238-44
www.eerp.usp.br/rlae
Corresponding Author:
Tereza Cristina Cavalcanti Ferreira de Araujo Universidade de Brasília
Instituto de Psicologia. Laboratório de Saúde e Desenvolvimento Humano Campus Darcy Ribeiro
CEP: 70910-900 Brasília, DF, Brasil.
E-mail: [email protected] / [email protected]
Impact of the Clinical Management of Pain: Evaluation of Stress and
Coping Among Health Professionals
Maíra Ribeiro de Oliveira Negromonte
1Tereza Cristina Cavalcanti Ferreira de Araujo
2The specialist literature highlights that the clinical management of pain involves psychological
difficulties associated with the pursuit of the alleviation of the suffering of patients. Therefore,
an investigation was conducted into the perception of stress and coping strategies of 31
professionals of different categories from a severe burns care center (acute pain) and a pain
control and palliative care unit (chronic pain). For this, a sociodemographic questionnaire,
the Job Stress Scale (short version) and the Coping Strategies Inventory were applied.
Compared to other categories, the nursing technicians indicated more stress factors.
In compensation, they reported a greater diversity of coping strategies with significant
differences between the services. These results corroborate previous studies, which warn
of the adverse conditions that interfere in nursing practice. However, they also reveal the
availability of protective factors, indicating perspectives of preventive intervention for the
nursing team.
Descriptors: Pain; Bernout, Professional; Health Personnel.
Impacto do manejo clínico da dor: avaliação de estresse e enfrentamento entre proissionais de saúde
A literatura especializada destaca que o manejo clínico da dor comporta diiculdades psicológicas, associadas à busca de alívio do sofrimento dos pacientes. Sendo assim,
investigaram-se a percepção de estresse e as estratégias de enfrentamento de 31 proissionais de diferentes categorias, em um centro de atendimento a grandes queimados (dor aguda) e uma unidade de controle de dor e cuidados paliativos (dor crônica). Para tanto, aplicaram-se um questionário sociodemográico, a Job Stress Scale (versão resumida) e o Inventário de Estratégias de Coping. Comparativamente
às demais categorias, os técnicos de enfermagem indicaram mais fatores de estresse.
Em compensação, informaram maior diversidade de estratégias de enfrentamento com diferenças signiicativas entre os serviços. Esses resultados corroboram estudos anteriores, os quais alertam sobre as condições adversas que interferem na atuação em
enfermagem. Porém, também revelam disponibilidade de fatores de proteção, apontando
perspectivas de intervenção preventiva, destinada à equipe de enfermagem.
Descritores: Dor; Esgotamento Proissional; Pessoal de Saúde.
Impacto del manejo clínico del dolor en los profesionales de la salud: evaluación de estrés y enfrentamiento
La literatura especializada destaca que el manejo clínico del dolor produce diicultades psicológicas asociadas a las actividades realizadas para aliviar el sufrimiento de los
pacientes. Siendo así, se investigaron la percepción del estrés y las estrategias para
enfrentarlo en 31 profesionales de diferentes categorías en un centro de atención a
quemaduras de gran tamaño (dolor agudo) y una unidad de control del dolor y cuidados paliativos (dolor crónico). Para esto, se aplicó un cuestionario sociodemográico, la Job Stress Scale (versión resumida) y el Inventario de Estrategias de Coping. Comparado
con las demás categorías, los técnicos de enfermería indicaron más factores de estrés.
En compensación, informaron mayor diversidad de estrategias de enfrentamiento con diferencias signiicativas entre los servicios. Estos resultados corroboran estudios anteriores, los cuales alertan sobre las condiciones adversas que interieren en la actuación en enfermería. Sin embargo, también revelan la disponibilidad de factores de
protección, apuntando perspectivas de intervención preventiva destinadas al equipo de
enfermería.
Descriptores: Dolor; Agotamiento Profesional; Personal de Salud.
Introduction
Patients who suffer from chronic pain, and severe
burn patients that experience acute pain, are usually
assisted by a multidisciplinary team composed of
physicians, nurses, physical medicine professionals, and
psychologists, among others(1-2). Treating these patients
constitutes a challenging and often frustrating task for
the agents involved. It is noteworthy that the stress levels of caregivers are inluenced by the reactions of
the patients, who may present depression or anxiety(3)
before treatments that induce many collateral effects
with little immediate relief of suffering(2,4). Added to this
is the overload of work and the dificulties caused by their participation in a team composed of professionals
of heterogeneous training(5-6). In fact, the specialized
literature reveals increasing interest in the care of those
who perform the role of caregivers(7-8). This trend is
due, in part, to the veriication of pathological reactions triggered by the act of caring. It is worth insisting that
besides affecting the patient, the experiences provoked
by pain contaminate their family and the rest of their
socio-emotional context, including the professionals
in attitude of the health professionals themselves,
who have started to admit their need for care in some
circumstances(8), also contributes to the development of
studies on the subject.
According to the transactional model(10), it is
not possible to comprehend the stress by examining
the environmental events and the responses of the
individual separately. Both should be comprehended as
a transaction, in which each individual seeks to adjust
to the quotidian challenges(11). Thus, the exchanges
between people and the environment occur through a
cognitive evaluation, in which the following are analyzed:
whether the situation threatens the well-being; whether the resources are suficient to cope; and, during the
cycle, whether the chosen strategy is effective(12). In the
1970s, Robert Karasec and other pioneering researchers
showed that working relationships represent a generator
source of stress with health repercussions. They proposed
a bidimensional model that relates psychological
demand and the control of the risks of becoming ill.
According to its supporters, the psychological demand
refers to quantitative factors such as time and speed in
performing the work, and qualitative factors, such as conlicts arising from contradictory requests. The control corresponds to making possible the use of intellectual
abilities and decision making regarding how to conduct
the work activity(13). Therefore, the coexistence of high
psychological demands with low control generates
professional distress and may have a negative impact
on the health of the worker(14). These conditions typically
characterize the practice of the health professionals,
who are subjected to constant tension due to the nature
of their actions with people whose physical, mental
and social integrity is affected, as well as due to the
need to manage complex institutional issues associated
with public policies and the exchange between different
professional categories(7).
Coping is commonly deined as cognitive and behavioral efforts to deal with (reduce, dominate
or tolerate) the external demands of the
individual-environment relationship, which are evaluated as
overloading or exceeding the personal resources(15). This
deinition comes from the model proposed by Lazarus
and Folkman(10), which advocates coping as a process
resulting from reciprocal responses between individuals
and their context over a period of time(16). This is a
moderator of the events evaluated as stressful, which
can reduce the severity of the symptoms(17). The coping
strategy would be considered effective when the behavior
alleviated the uncomfortable feelings raised by threats
or losses. It would be considered ineffective, when it
was not possible to deal with the stressful situation in
a successful manner, which could trigger psychological
and physiological imbalances(18).
In summary, in view of the scientiic and professional interest in the area of health, an investigation was carried
out into the perception of stress and coping strategies
adopted by the professionals of specialized teams in the
monitoring of patients with acute and chronic pain.
Method
Participants
The purposive sample was constituted by
professionals of different categories from a severe
burns monitoring service (SBMS) and a chronic pain
and palliative care service (CPPCS). Table 1 presents the
main characteristics of these participants.
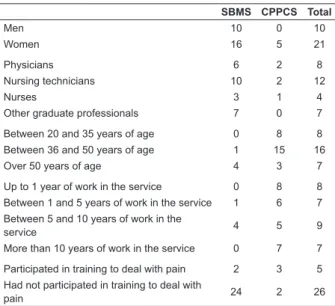
Table 1 - Characterization of the professionals
SBMS CPPCS Total
Men 10 0 10
Women 16 5 21
Physicians 6 2 8
Nursing technicians 10 2 12
Nurses 3 1 4
Other graduate professionals 7 0 7
Between 20 and 35 years of age 0 8 8 Between 36 and 50 years of age 1 15 16 Over 50 years of age 4 3 7
Up to 1 year of work in the service 0 8 8 Between 1 and 5 years of work in the service 1 6 7 Between 5 and 10 years of work in the
service 4 5 9
More than 10 years of work in the service 0 7 7
Participated in training to deal with pain 2 3 5
Had not participated in training to deal with
pain 24 2 26
Instruments
Sociodemographic questionnaire for characterization of the sample
Coping Strategies Inventory of Folkman and
Lazarus (adapted into Portuguese)(19), comprising 66
items that classifythe coping strategies into eight factors
(confrontation, distancing, self-control, social support,
accepting responsibility, escape-avoidance, problem
solving and positive reappraisal) and according to the
intensity (I did not use this strategy, I used it a little, I
used it, and I used it very much).
Negromonte MRO, Araujo TCCF.
Portuguese(14), encompassing 17 items for the evaluation
of demand, control and social support perceived by the
worker, which are measured on a Likert scale of four
points (ranging between often and never/almost never
or between strongly agree and strongly disagree).
Procedures for collecting and analyzing data
The study was previously approved by a Research
Ethics Committee and the agreement of the professionals
was obtained by signing the Terms of Free Prior Informed
Consent (TFPIC). Initially, the Sociodemographic
Questionnaire was applied followed by the scale and the
inventory, respectively. For data analysis, the statistical
package SPSS version 17.0 was used. As the distribution
of participants in the majority of groups based on the
antecedent variables, was less than 15, the use of
nonparametric tests was chosen to obtain descriptive,
comparative statistics and, in a few cases, correlations.
Results
Stress
Regarding the psychological demands, the scores
obtained ranged from 12 to 22, with an associated mean
Figure 1 - Distribution of the Job Stress Scale factors for the professional groups
of 17.7. These values indicate the existence of demands
at higher levels than the expected median (15). Similarly,
the factor control reached values between 16 and 29 and
an associated mean of 22.9, also above the expected
median (18). Regarding social support, considered to be
a moderating factor of work stress, a mean value of 18.2 was veriied, which is slightly higher than the expected median (between 12 and 18). Comparing the four groups identiied in the professional categories (antecedent variable) with the factors proposed by the Job Stress Scale, statistically signiicant differences were found in the dimensions control and social support (Figure 1).
With regard to the factor control, it was ascertained
that the mean values indicated by the graduate professionals were signiicantly different from those estimated by the nursing technicians. In other words,
physicians, nurses and other graduate categories
reported having more control over the work activity
than nursing technicians. However, physicians and
nurses perceived receiving more social support than
nursing technicians and other graduate professionals. No signiicant differences were veriied between the two
teams surveyed with regard to the factors of the Job
Stress Scale.
Coping
All factors relating to the Coping Inventory achieved
means congruent with the median values expected.
The coping strategies used most often encompassed
the following factors in ascending order:
escape-avoidance, confrontation, self-control, problem solving,
withdrawal, social support, accepting responsibility and
positive reappraisal.
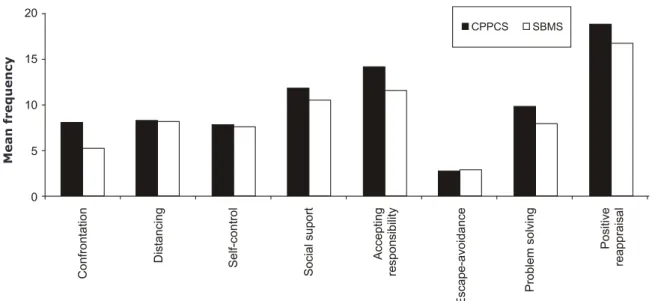
As illustrated in Figure 2, signiicant differences were found between the members of the SBMS (acute
pain) and the CPPCS (chronic pain) in relation to the
confrontation and resolution of problems (U=29, p=0.05
and U=22, p=0.02, respectively). It is important to
highlight that the professionals of the CPPCS reported
using more of the strategies grouped in these factors.
M
e
an
f
req
u
en
c
Figure 2 - Distribution of the Coping Inventory factors by service
From the data gathered through the
Sociodemographic Questionnaire regarding the
participation, or not, in speciic training for the clinical management of pain, differences in the factor problem solving were identiied. That is, in general, the professionals who responded positively to the enquiry
adopted more strategies linked to problem solving than
those who did not mention this training program.
Discussion
The overall results obtained from the Job Stress
Scale indicated high levels of psychological demands.
Conversely, they also highlighted higher levels of control
in the work and social support received. Such a situation,
in which high psychological demands are associated with
high control, reveals that the participants experience
their work actively. That is, although the psychological
demands are excessive, they are less harmful, since
the worker can develop strategies to cope with the dificulties(14). Furthermore, the adverse conditions
of the work context of the studied teams also seem
to ease when high levels of positive social interaction
are detected. However, when analyzing each of the professional categories separately, speciicities emerged. Thus, while the indexes related to the perception of
psychological demands were presented as equally high for all categories, differences were veriied between control and social support in the area of nursing. It is worth relecting that the low mean scores achieved by the nursing technicians can be comprehended by
considering the persistence of a strong hierarchy in the
health services, despite the nefarious consequences of
this mode of organization, already widely discussed in
the literature(20). In the case of the nurses who achieved
higher values, it must be remembered that they assume
the administrative coordination of the services and the
leadership of the nursing staff. Due to this function,
they concentrate much of the information regarding
the operation of the service and the clinical condition
of the patients, by increasing their interaction with
the other members of the multidisciplinary team and
ensuring greater autonomy in establishing their work
routines. This peculiarity can clarify the data found in
this category.
It is worth mentioning that, in the SBMS, the
burn remains as an acute pathological condition that
demands, at least in the initial phases of care, actions
geared primarily to maintaining the vital signs of the
patient. In the CPPCS there are peculiarities inherent
in the outpatient context in which complaints related
to chronicity predominate, such as the terminality,
which require a high complexity of care(2). In these
circumstances, the high levels of social support
perceived by the professionals can be generated by
feelings of intense frustration due to the recurrence
of therapeutic weaknesses(9), which ultimately favor
an approach known as integrative metatheory. This is
a perspective where the different dimensions interact
in the health-disease process and enable effective
multidisciplinary practice(20). Similarly, it can be observed
that the chronicity provokes changes that mainly affect
the relationship of the physician with the other health
professionals and with the patient(2).
M
ean
f
re
q
u
e
n
c
Negromonte MRO, Araujo TCCF.
Regarding the factors of the Coping Inventory, when
the services were compared, some distinctions were
observed: professionals of the SBMS tend to use fewer
strategies categorized as confrontation and problem
solving than the professionals of the CPPCS. It should
be considered that, on one hand, the SBMS is a large
service, composed of an extensive and differentiated
team that provides 24 hours care (clinical, surgical
and rehabilitation). Due to this diversity and coverage,
a shared, yet paradoxically impersonal, responsibility
is assumed, which expresses itself through reduced
individual use of strategies focused on confronting the
situation and problem solving. On the other hand, in the
CPPCS, patients often receive prescription medication or
guidelines of conduct in each of the consultations with
the various professionals, and it is expected that the
strategies for confronting the situation and problems
solving are more frequent.
Finally, a comparison of the stress and coping
indicators infer that high levels of control in the work are linked preferentially to strategies classiied as problem solving. Similarly, the presence of high psychological
demands suggests the use of strategies focused on
positive reappraisal. It is also relevant to note that
both the Job Stress Scale and the Coping Inventory
determined the availability of an effective social support
network in the work context.
Conclusion
This study showed that the nursing technicians
are subjected to more stress than the other categories,
including nurses. In compensation, the nursing categories
mobilize a greater diversity of coping strategies. These
results warn of the adversities that interfere in nursing practice. Protective factors were also identiied, which can support proposals for preventive intervention aimed
at the nursing team. In other words, it is essential to
strengthen the coping strategies already employed and
to introduce other modalities indicated by the literature
and acceptable in the context of each team, depending
on their specialization in the care of patients with acute
or chronic pain. It is equally crucial to organize and offer continuing education courses, aimed at the qualiication and training of these teams, which are based on previously
developed studies. Further studies are recommended to
better elucidate the conditions that promote and hinder the effective and eficient multidisciplinary teamwork in the context of services that treat patients with pain. It
is essential to evaluate more fully and accurately the
impact of the clinical management of pain on the health
of the professionals and consequently on the quality of
life and well-being of the users.
References
1. Baszanger I. Pain: its experience and treatment. Soc
Sci Med. 1989;29(3):181-215.
2. Lima MAG, Trad L. Dor crônica: objeto insubordinado.
Hist Ciênc Saúde - Manguinhos. 2007;15(1):117-33.
3. Castro MMC, Quarantini L, Batista-Neves S, Kraychete
DC, Daltro C, Miranda-Scippa A. Validade da escala
hospitalar de ansiedade e depressão em pacientes com
dor crônica. Rev Bras Anestesiol. 2006;56(5):470-7.
4. Teixeira MJ, Figueiró JAB, Yeng LT. Tratamento
multidisciplinar em doentes com dor. In: Carvalho
MMMJ. Dor: um estudo multidisciplinar. São Paulo (SP):
Summus; 1999. p. 87-139.
5. Queiroz E, Araujo TCCF. Trabalho em equipe: um
estudo multimetodológico em instituição hospitalar de
reabilitação. Interam Psychol. 2007;41(2):221-30.
6. Costa CB Neto. Fatores do processo de tomada
de decisão da equipe de saúde numa instituição de
tratamento a irradiados por fonte ionizante: um estudo
de caso [dissertação de mestrado]. Brasília (DF):
Instituto de Psicologia da Universidade de Brasília;
1994. 315 p.
7. Campos EP. Equipe de saúde: cuidadores sob tensão.
Epistemo-somática. 2006;3(2):195-222.
8. Carvalho V. A equipe de saúde e suas vicissitudes
emocionais. In: Pimenta CAM, Mota DDCF, Cruz DALM.
Dor e cuidados paliativos. São Paulo (SP): Manole;
2006. p. 103-23.
9. Maciel MGS. Dor crônica no contexto dos cuidados
paliativos. Prática Hosp. [internet]. 2004 [acesso:
30 outro 2010];6(35). Disponível em: http://www.
praticahospitalar.com.br/pratica%2035/paginas/
materia%2005-35.html
10. Lazarus RS, Folkman S. Stress, apraisal and coping.
9th.ed. New York: Springer; 1984. 445 p.
11. Straub RO. Estresse. In: Straub RO. Psicologia da
saúde. Porto Alegre (RS): Artmed; 2004. p. 115-49.
12. Lazarus RS. [Do estresse psicológico às emoções:
uma história de mudança de pontos de vista]. Ann Rev
Psychol. 1993;44:1-22. Inglês.
13. Ulhoa MA, Moreno CRC. Fatores psicossociais
no trabalho e cortisol: breve revisão. Interfacehs.
2009;4(3):63-73.
14. Alves MGM, Chor D, Faerstein E, Lopes CS, Werneck,
Pública. 2004;38(2):164-71.
15. Folkman S, Lazarus RS, Dunkel-Schetter C, DeLongis
A, Gruen RJ. [Dinâmicas de um encontro estressante:
avaliação cognitiva, enfrentamento e resultados do
encontro]. J Person Soc Psychol.
1986;50(5):992-1003. Inglês.
16. Gimenes MGG. A teoria do enfrentamento e
suas implicações para os sucessos e insucessos da
psiconcologia. In: Gimenes MGG. A mulher e o câncer.
Campinas (SP): Psy; 1997. p. 111-48.
17. Murta SG, Laros JA, Tróccoli BT. Manejo de estresse
ocupacional na perspectiva da área de avaliação de
programas. Est Psicol. 2005;10(2):167-76.
18. Lorencetti A, Simonetti JP. As estratégias de
enfrentamento de pacientes durante o tratamento
de radioterapia. Rev. Latino-Am. Enfermagem.
2005;13(6):944-50.
19. Savoia MG, Santana P, Mejias NP. Adaptação do
Inventário de Estratégias de Coping de Folkman e Lazarus
para o português. Psicol USP. 1996;17(7):227-38.
20. Reis JC. Modelo metateórico da psicologia da
saúde para o século XXI: interação ou integração
biopsicossocial? Análise Psicol. 1999;17(3):415-33.
Receiveed: Mar. 16th 2010