r e v b r a s r e u m a t o l . 2017;57(1):88–91
ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Brief
communication
Ultrasound
color
histogram
assessment
allows
better
view
of
echotexture
damage
O
histograma
de
imagens
coloridas
permite
melhor
visualizac¸ão
de
danos
ecotexturais
pelo
ultrassom
José
Alexandre
Mendonc¸a
PontifíciaUniversidadeCatólicadeCampinas(PUC-Campinas),DepartamentodeReumatologia,Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20January2014
Accepted7December2014
Availableonline23November2015
The technological advances have resulted in significant
improvementsinthequalityanddefinitionof
ultrasonogra-phy(US)asanevaluationtoolofjointstructures,andithas
beenfrequentlyusedinthepropedeuticaidforavarietyof
rheumatologicdiseases.1–4 RecentfindingsonjointUS
war-rant a broad spectrum of indications from assessment of
jointsynovitis(SYN),tendinitis,bursitis,inflammatory
activ-ity follow-up, aspiration monitoring, guided injections for
therapeuticand diagnostic punctures.5,6 US resultsquality
dependsonthecharacteristicsoftheequipmentandonits
operator, requiring knowledge of anatomy, pathology and
techniquesallowedbytheequipment.7
Jointultrasound(US),likeotherimagingmethodscanaidin
diagnosis,progressofthediseaseandidentificationofactual
declineinsignsandsymptomsofmanydiseases.8,9
Theradiographicevaluationdetectsbonestructural
dam-agebelatedly,whiletheUSshowsearlyjointchangesandthus
facilitatestheinitialdiagnosisofrheumatoidarthritis(RA).10
ThemusculoskeletalUSisanimagingmethodthatcanbe
con-sideredasensitivetoolcomparedtoradiographyandoffers
E-mail:[email protected]
similaraccuracycomparedtothemagneticresonance,being
usefulbothfordetectingandfollowinginflammatoryactivity,
andfortheassessmentofstructuraldamageinvarioustypes
ofarthropathies.11–15
Theuseofgrayscale(GS)hasprovedtobeareliable
instru-menttocheckstructuralchanges,settingdifferentdegreesof
lesioninRAandpsoriaticarthritispatients,therebyevaluating
theactivityofthesediseasesthroughthecharacterizationof
thesynovitis.TheUShasprovedtobeimportantinthe
mon-itoringoftreatmentwithhigh-complexitydrugs,suchasthe
biologicalones.16 Additionally,GSprovestobeableto
eval-uatetheextentofeffusion,andsynovialproliferation,even
signalingthediseasestage,namelyaninitialsynovitisoran
alreadyestablishedone.Thus,UScancomplementtraditional
clinicalevaluationresourcesinpatientswithmusculoskeletal
conditions,reducingthesubjectivityoftheclinical
examina-tion.TheUShasalsoprovedtobemoresensitivethanclinical
evaluationsfordetectingenthesitisinpatientswith
ankylos-ingspondylitis17andcanbeasensitive,andalmostspecific
techniquetodetect softtissueorjoint calcifications.18 Itis
http://dx.doi.org/10.1016/j.rbre.2015.05.001
2255-5021/©2015ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
rev bras reumatol.2 0 1 7;57(1):88–91
89
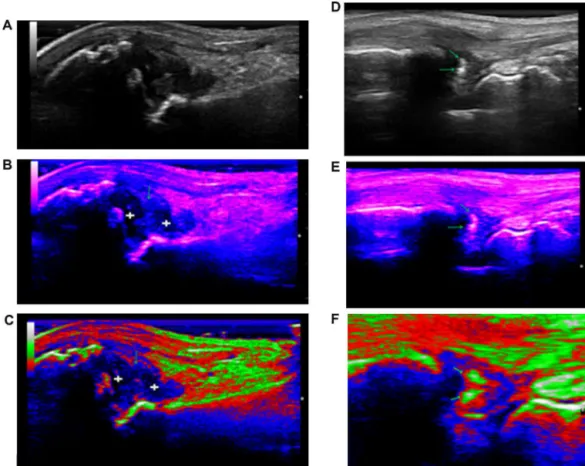
Fig.1–(A–C)Synovitisin1stmetacarpophalangealjointinapatientwithpsoriaticarthritis;A:synovitisassessmentby grayscale(GS).BandC:Assessmentofthesameimages,exudative(+sign)andproliferative(arrow)synovitis,byIndigo andRGBpatterns,throughcolormap–Mode–BHistogram,respectively.(D-F,Calcificationsinthetriangularfibrocartilage complexofthewrist(TFC)inapatientwithchondrocalcinosis);D-F:Evaluationofcalcifications(arrows),inwristTFC,byGS, IndigoandRGB,throughcolormap–Mode–BHistogram,respectively.
importanttouseahighfrequencylinearprobethatranges
from18MHztoGSintheevaluationofsmalljointsandsurface
structures.
Ultrasonographywithhigh frequencylineararrayprobe,
besidesallowingabetterresolutionintheGS,isabletoidentify
colorimagesstandards, betterhighlightingmusculoskeletal
echotexturedamagealreadypresent.Thisisthecaseofcolor
imageswithRGBpattern,whichareformedbyinformationof
additiveprimarycolors,suchasred(R–Red),green(G–Green)
andblue(B–Blue),“orange”,“indigo”,“magenta”,“blue”and
“yellow”, generating a histogram, considered unique for a
given image, a simple method, offered by US machine, a
resourcethatbelongstotheB-modesoftware.
Thehistogrammodificationtechniquesareknownas
dot-to-dottechniques,sincethegraylevelvalueofacertainpixel
afterprocessingdependsonitsoriginalvalueonly.Incontrast,
intheprocessingtechniquesforcompletionofcolorimages,
theresultingvaluedepends,insomeway,onthepixels
sur-roundingtheelementoftheoriginalpixel.
Severaltechniquesofpixelsdistribution modification in
the GScan be implemented from the concept ofintensity
transformations,meaningthat an originalimage ina new
shadeofgray,inthetargetimage,increasingitscontrastand
resolutionofthelesionunderstudy.
Thelinearintensitytransformationconceptcanbeusedto
implementafunctionthatautomaticallyexpandsthescaleof
animagegrayscalesothatitfillsallthepossiblegaps.This
feature iscalledauto-scaling.For asystemwhich operates
withimagesat256levelsofgray,anauto-scalefunctioncanbe
implementedforeachpixelwithagraytoneandeachtoneof
differentcolor.Theequalizationofahistogramisatechnique
whereoneseekstoredistributethegrayscalevaluesofpixels
inanimage;therefore,anancillaryfunctionisused,whichis
calledtransformationfunction,forthissameimageincolor.
Theobjectiveofcolormodelsistoallowcolorspecification
inauniversallyacceptedstandardformat.19Thedetectionof
synovitis(SYN)andcalcifications(calcif)throughahistogram,
that is, patternsofcolor images, incontrast withGS, may
facilitatetheidentificationofechographicstructuraldamages,
givingbetteraccuracyinmeasurementsandmoreaccurate
diagnosisofthelesionstudied,especiallyinsituationsthat
generatedoubtinimageanalysis.RGBpatterncanbestshow
anexudativeSYNofaproliferativeSYN,whenwehave,ina
singlestructure,amixedtypeofsynovialtissuedamage,but
alsocanbetterdetectcalcifbecausethisechotexturedamage,
inthispattern,showsechotexturethatisidenticaltothe
cor-ticalbone,differentiatingthesefindingswhentheyareinsoft
90
rev bras reumatol.2 0 1 7;57(1):88–91Fig.2–(A–C)Areameasurements,incm2ofcalcificationsinthetriangularfibrocartilagecomplexofthewristinapatient
withChondrocalcinosis–calcificationsassessmentbygrayscalepatterns,IndigoandRGB,respectively,confirmedthe presenceof“white”echotexture,identicaltothecorticalulnarbone.
Thus,weevaluated10patients,meanage40.7yearsold,
2malesand8females.Atotalof104SYNand calcif
mea-surementsincm2wereperformedinthedorsalradiocarpal
joint (DRR); triangular fibrocartilage complex (TFC); dorsal
metacarpophalangeal joints (MCP) and lateral and medial
kneesuprapatellarrecesses.Fourpatientsexhibited
chondro-calcinosis, 5patients osteoarthritis and 1patient psoriatic
arthritis.ForeachmeasurementinGStherewasone
measure-mentperformedforeachcolorimagepattern,heldatdifferent
timesandblind,inorderthatthepreviousmeasuresarenot
seenorremembered.FortheSpearmancorrelationanalysis,
thesoftwareIBMSPSSStatistics19wasused.
Mean±SDofimagepatterns:RGB(Red,GreenandBlue)
SYN 16.96±0.25cm2; Indigo SYN 6.43±0.07cm2, RGB
Cal-cif 0.03±0.00cm2; Indigo Calcif 0.06±0.03cm2; GS SYN
16.13±0.35cm2andGSCalcif0.56
±0.01cm2.
Correlationsofcolorimagespatterns:RGBDRRSYNand
IndigoDRRSYN:r=1.0,p<0,001;IndigoDRRSYNand RGB
suprapatellarSYN:r=1.0,p<0.001;RGBMCPSYNandIndigo
MCPSYN:r=1.0,p<0.001;IndigoDRRcalcifandRGBTFCcalcif:
r=1.0,p<0.001(Fig.2).
TheRGBand Indigo measurement standardswhen
cor-related with GS for SYN and calcifs were not statistically
significant(p=0.333–0.667).ColorimagespatternsofGS,
rep-resentedbythehistogram,evaluatesSYNandcalcifthrough
RGB,“orange”,“indigo”,“magenta”,“blue”and“yellow”,and
RGBandIndigopatternsseemtobetterdelimitthese
echo-texturedamage,throughbettervisualization,detectedbyarea
measurementsincm2.
ThisidentificationofstructuraldamagebytheUS,usinga
colorhistogram,hasneverbeenpreviouslydonethiswayfor
rheumaticdiseases.Furtherstudiesareneededtostrengthen
theseUSfindings.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. FilippucciE,IagnoccoA,MeenaghG,RienteL,DelleSedieA, BombardieriS,etal.Ultrasoundimagingforthe
rheumatologist.ClinExpRheumatol.2006;24:1–5.
2. GrassiW,SalaffiF,FilippucciE.Ultrasoundinrheumatology. BestPractResClinRheumatol.2005;19:467–85.
3. KaneD,GrassiW,SturrockR,BalintPV.Musculoskeletal ultrasound–astateoftheartreviewinrheumatology.Part2:
Clinicalindicationsformusculoskeletalultrasoundin rheumatology.Rheumatology.2004;43:829–38.
4.KaneD,BruynG,ArnoldE,GrassiW.Arheumatologist’s perspectiveonmusculoskeletalultrasoundinrheumatology: commentontheeditorialbyRoemeretal.ArthritisRheum. 2006;55:341–2.
5.D’AgostinoMA,AyralX,BaronG,RavaudP,BrebanM, DougadosM.Impactofultrasoundimagingonlocal corticosteroidinjectionsofsymptomaticankle,hind-,and mid-footinchronicinflammatorydiseases.ArthritisRheum. 2005;53:284–92.
6.KoskiJM,HelleM.Ultrasoundguidedsynovialbiopsyusing portalandforceps.AnnRheumDis.2005;64:926–9.
7.FerriM,FinlayK,PopowichT,StampG,SchuringaP,Friedman L.Sonographyoffull-thicknesssupraspinatustears:
comparisonofpatientpositioningtechniquewithsurgical correlation.AJRAmJRoentgenol.2005;184:180–4.
8.LuukkainenRK,SaltyshevM,KoskiJM,HuhtalaHS. Relationshipbetweenclinicallydetectedjointswellingand effusiondiagnosedbyultrasonographyin
metatarsophalangealandtalocruraljointsinpatientswith rheumatoidarthritis.ClinExpRheumatol.2003;21:632–4.
9.NaredoE,BonillaG,GameroF,UsonJ,CarmonaL,LaffonA. Assessmentofinflammatoryactivityinrheumatoidarthritis: acomparativestudyofclinicalevaluationwithgreyscaleand powerDopplerultrasonography.AnnRheumDis.
2005;64:375–81.
10.GrassiW,FilippucciE,FarinaA,SalaffiF,CerviniC. Ultrasonographyintheevaluationofboneerosions.Ann RheumDis.2001;60:98–103.
11.KarimZ,WakefieldRJ,ConaghanPG,LawsonCA,GohE, QuinnMA,etal.Theimpactofultrasonographyondiagnosis andmanagementofpatientswithmusculoskeletal
conditions.ArthritisRheum.2001;44:2932.
12.ScheelAK,BackhausM.Prospective7yearfollowupimaging studycomparingradiography,ultrasonography,andmagnetic resonanceimaginginrheumatoidarthritisfingerjoints.Ann RheumDis.2006;65:595–600.
13.BackhausM,KamradtT,SandrockD,LoreckD,FritzJ,WolfKJ, etal.Arthritisofthefingerjoints:acomprehensiveapproach comparingconventionalradiography,scintigraphy,
ultrasound,andcontrast-enhancedmagneticresonance imaging.ArthritisRheum.1999;42:1232–45.
14.SzkudlarekM,NarvestadE,KlarlundM,Court-PayenM, ThomsemHS,ØstergaardM.Ultrasonographyofthe metatarsophalangealjointsinrheumatoidarthritis: comparisonwithmagneticresonanceimaging,conventional radiography,andclinicalexamination.ArthritisRheum. 2004;50:2103–12.
15.BrownAK,ConaghanPG,KarimMA.Anexplanationforthe apparentdissociationbetweenclinicalremissionand continuedstructuraldeteriorationinrheumatoidarthritis. ArthritisRheum.2008;58:2958–67.
rev bras reumatol.2 0 1 7;57(1):88–91
91
scale,andpowerDopplerultrasoundassessmentofthe responsetoetanercept.AnnRheumDis.2005;64: 899–905.
17.BalintPV,KaneD,WilsonH,McInnesI,SturrockR.
Ultrasonographyofenthesealinsertionsinthelowerlimbin spondyloarthropathy.AnnRheumDis.2002;61:905–10.
18.FredianiB,FilippouG,FalsettiP,LorenziniS,BaldiF,AcciaiC, etal.Diagnosisofcalciumpyrophosphatedihydratecrystal depositiondisease:ultrasonographiccriteriaproposed.Ann RheumDis.2005;64:638–40.