ARTICLE
Muscle biopsy in Pompe disease
Biópsia muscular na doença de Pompe
Lineu Cesar Werneck, Paulo José Lorenzoni, Cláudia Suemi Kamoi Kay, Rosana Herminia Scola
Pompe disease (PD), also known as glycogenosis type II or acid maltase deiciency, is a rare inherited disease caused by acid alpha-glucosidase (GAA) deiciency. his enzyme participates in the deg-radation of glycogen into glucose inside muscle ibers. Mutations in the GAA gene induce several degrees of enzyme deiciency, causing glycogen accumulation in muscle ibers lysosomes1.
he prevalence of PD ranges from 1:40,000 to 1:60,000 and is dependent on ethnic and geographical factors. Compared with other diseases, it is rarely observed in centers for neuromuscu-lar disorders2,3. he clinical manifestation varies with age and
the degree of enzyme deiciency, and three clinical forms are recognized: infantile or “classic”, clinical manifestation present in the irst months of life; childhood or “non-classic”, clinical manifestation present after the irst or second year of life; and adult or late onset, no clear cutof between these forms1.
he diagnosis of PD can be conirmed by evaluating GAA activity in a dried blood spot assay or in leukocyte or skin
ibroblast cultures in most cases4. A molecular analysis can also
be used to identify GAA mutations in highly suspected cases5.
However, for the childhood and adult forms, the clinical symp-toms, physical indings and laboratory features may indicate another muscle disorder, such as muscular dystrophy, or a met-abolic muscle disorder1,5,6. In cases with no family history of PD,
muscle biopsy is performed routinely in the diagnostic work-up. In this study, we analyzed the histological and histochem-ical indings of muscle biopsy specimens taken from Brazilian PD patients.
METHODS
A retrospective analysis of 4,500 muscle biopsies per-formed from 1979 to 2012 identiied 19 patients with a PD di-agnosis conirmed by the deiciency of GAA enzyme activity
Neuromuscular/Neurology Division, Internal Medicine Department, Hospital de Clínicas da Universidade Federal do Paraná, Curitiba PR, Brazil.
Correspondence: Lineu Cesar Werneck; Serviço de Doenças Neuromusculares, Hospital de Clínicas da Universidade Federal do Paraná / 3° andar / sala 310; 80060-900 Curitiba PR - Brasil; E-mail: [email protected]
Support: CNPq, Fundação Araucária and CAPES.
Conflict of interest: There is no conlict of interest to declare.
Received 01 November 2012; Received in inal form 05 November 2012; Accepted 13 November 2012.
ABSTRACT
Pompe disease (PD) can be diagnosed by measuring alpha-glucosidase levels or by identifying mutations in the gene enzyme. Muscle biop-sies can aid diagnosis in doubtful cases. Methods: A review of muscle biopsy from 19 cases of PD (infantile, 6 cases; childhood, 4 cases; and juvenile/adult, 9 cases). Results: Vacuoles with or without glycogen storage were found in 18 cases. All cases had increased acid phosphatase activity. The vacuole frequency varied (almost all ibers in the infantile form to only a few in the juvenile/adult form). Atrophy of type 1 and 2 ibers was frequent in all forms. Atrophic angular ibers in the NADH-tetrazolium reductase and nonspeciic esterase activity were observed in 4/9 of the juvenile/adult cases. Conclusion: Increased acid phosphatase activity and vacuoles were the primary indings. Most vacuoles were illed with glycogen, and the adult form of the disease had fewer ibers with vacuoles than the infantile or childhood forms.
Key words: Glycogen storage disease type II, muscle biopsy, immunohistochemistry, acid phosphatase, vacuoles.
RESUMO
O diagnóstico da doença de Pompe (PD) pode ser feito pela dosagem da enzima alfa-glicosidase ou pela mutação do seu gene codiica-dor. A biópsia muscular pode ajudar em casos duvidosos. Métodos: Revisão das biópsias musculares de 19 casos de PD (forma infantil, 6 casos; infantil tardia, 4; e juvenil/adulto, 9). Resultados: Encontrados vacúolos em 18 casos, com ou sem depósito de glicogênio. Todos mostraram aumento da fosfatase ácida. Os vacúolos estavam presentes na maioria das ibras nas formas infantis, menos frequentes nas formas juvenil e mais raros nas formas do adulto. A atroia de ibras dos tipos 1 e 2 ocorreram em todas as formas. Fibras atróicas na NADH-tetrazolium redutase e esterase não especíica foram observadas em 4/9 das formas infantil tardia/adulta. Conclusões: Os dados mais frequentes foram vacúolos, preenchidos por glicogênio com atividade aumentada da fosfatase ácida. A forma adulta apresenta menor número de vacúolos que as formas infantil e infantil tardia.
Palavras-Chave: Doença de depósito de glicogênio tipo II, biópsia muscular, imunohistoquímica, fosfatase ácida, vacúolos.
in a dried blood spot assay, leukocytes, muscle tissue or skin ibroblast cultures. In some cases, molecular analyses identi-ied a pathogenic mutation5. Consent to analyze the muscle
biopsy was obtained for each patient in the outpatient clinic or during patient admission to the hospital. he patients were classiied according to the age of symptom onset (Table 1): in-fantile (6 cases), childhood (4 cases) and adult onset (9 cases). he reason for the muscle biopsy difered between the three groups: infantile form, PD manifestation with severe hypo-tonia, weakness and heart involvement; childhood form, dif-ferential diagnosis with Duchenne muscular dystrophy; and adult form, diferential diagnosis with limb-girdle muscular dystrophy. Table 2 shows the results of the laboratory analy-ses (muscle enzyme levels) and electromyography for all cas-es prior to the muscle biopsy.
Muscle biopsy was performed at the quadriceps or bi-ceps brachial muscles. In three cases, the muscle biopsy was performed twice due to technical problems. Muscle bi-opsies were frozen in liquid nitrogen, and fresh-frozen cryo-stat sections were stained for hematoxylin-eosin, modiied Gomori trichrome, oil red O, periodic acid-schif (PAS), cre-syl violet and sirius red. he following histochemical reac-tions were performed according to standard procedures7:
ATPase at pH 4.3, 4.6 and 9.4; NADH-tetrazolium reductase;
nonspeciic esterase; myophosphorylase; acid phospha-tase; alkaline phosphaphospha-tase; succinate dehydrogenase; cyto-chrome-c oxidase; and adenylate deaminase.
RESULTS
Table 3 shows the histological and histochemical abnor-malities according to the diferent forms of PD.
he most common abnormalities found included vacuo-lated muscle ibers, PAS-positive vacuoles and increased acid phosphatase activity in muscle ibers.
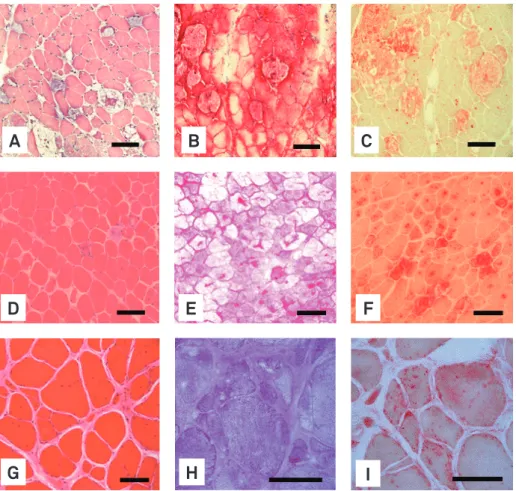
Vacuoles were present in almost all cases, but were ab-sent in one adult case. he vacuoles varied in size accord-ing to the clinical form and disease duration. In the infantile form, when the biopsy was performed in the irst months of life, the vacuoles were small with a large sarcoplasm. In bi-opsies from several-month-old infants, the vacuoles were large and had replaced most of the sarcoplasm. In the child-hood- and adult-onset clinical forms, the vacuoles were smaller than in the infantile form in some cases, allowing a large portion of the iber to develop with an apparently nor-mal structure. hese vacuoles stained positive for PAS, al-though the vacuoles material were occasionally washed out due to the preparation techniques (alcohol and xylol). he acid phosphatase activity was abnormal in all cases, with fo-cal increased activity in the sarcoplasm or vacuoles or dif-fuses activity (positive ibers) (Fig 1). Two cases had vacuoles without glycogen, and their GAA levels were below the nor-mal range in the muscle tissue (2.60 and 3.33 nmoles/min/gm, normal 8.13±2.06 nmoles/min/gm). In some of the adult cas-es, only a few ibers had vacuoles (Figs 2–4).
Other abnormalities were also observed. Most cases had variations of iber diameter with difuse iber atrophy, but it was more common in the infantile and childhood forms. Scattered atrophic ibers were common in the adult form; a trophy of i-ber types 1 and 2 was present in all forms, but hypertrophy of Table 1. Age of onset and disease duration in 19 cases of
Pompe disease.
Infantile Childhood Adult onset
Number of cases 6 4 9 Gender
Males 5 3 5
Females 1 1 4 Age at the time
of evaluation 0.54±0.28 (2–10) months 9.5±1.91 (7–11) years 28.22±9.74 (14–40) years Age of onset 0.18±0.14
(0–4) months
3.0±2.0 (1–5) years
20.80±7.35 (13.8–35) years Disease duration 0.35±0.23
(1–8) months
6.0±3.5 (2–8) years
7.41±6.56 (0.2–20) years
Table 2. Serum muscle enzyme levels and electromyography in 19 cases of Pompe disease.
Infantile Childhood Adult onset
Number of cases 6 4 9
Creatine kinase
(Fold increase above normal range)
3.12±2.27 (1–7) 2.50±3.0 (0–6) 13.44±22.39 (0–72) Lactic dehydrogenase
(Fold increase above normal range)
1.54±2.10 (0–5) 0.25±0.50 (0-1) 2.79±3.90 (0–9) Aldolase
(Fold increase above normal range)
3.11±3.12 (0–6) 0.21±0.42 (0–0.83) 2.53±4.67 (0–12) Aspartate aminotransferase
(Fold increase above normal range)
3.05±1.00 (2–4) 2.67±4.61 (0–8) 5.14±8.63 (0–18) Alanine aminotransferase
(Fold increase above normal range)
1.41±0.75 (1–2) 2.67±4.61 (0–8) 0.75±1.06 (0–2) Electromyography
Myopathic 2 2 7
Denervation 1 1 1
Mixed 0 0 1
Infantile Childhood Adult onset
Number of cases 6 4 9
Muscle studied
Quadriceps 6 3 6
Biceps 0 1 3
HE-Gomori
Proliferation connective tissue 0 1 2 Adipose tissue iniltration 0 1 2 Variation in iber diameter 5 4 9
Small group atrophy 0 1 0
Diffuse iber atrophy 5 4 0 Scattered iber atrophy 0 0 6 Angulated iber atrophy 0 0 2 Round atrophic ibers 5 4 7
Fiber hypertrophy 0 0 3
Internal nuclei 2 1 5
Nuclear clumps 0 0 1
Necrosis 1 0 4
Phagocytosis 1 0 2
Fiber splitting 0 0 1
Sarcoplasmic masses 0 1 0
Basophilic ibers 0 0 1
Vacuolated ibers 6 4 8
PAS
Vacuoles positive 6 2 7
Oil Red O
Increased lipid drops (type 1 ibers) 0 0 1
Deposit in vacuoles 0 1 0
External deposition 1 0 0
Sirius Red
Increased endomysial tissue 0 1 3 ATPases
Type 1 predominance 0 1 2
Type 2 predominance 1 0 0
Types 1 and 2 hypertrophy 0 0 3
Type 1 atrophy 2 2 6
Type 2 atrophy 2 4 7
NADH-Tetrazolium reductase
Angular atrophic ibers 0 0 3
Focal increase 1 3 2
Moth-eaten 0 1 3
Core like structure 0 1 0
Whirling 0 0 1
Snake coils 0 0 1
Ring ibers 0 0 1
Nonspeciic esterase
Angular atrophic ibers 0 1 4 Interstitial positive mononuclear cells 1 0 0 Acid Phosphatase
Increase iber focal activity 6 4 9
Positive ibers 5 1 7
Interstitial mononuclear cells 0 0 1 Macrophages in necrotic ibers 0 0 1 Alkaline Phosphatase
Positive ibers 0 0 1
Increased interstitial activity 0 0 1 Succinic Dehydrogenase
Increased in periphery 1 0 1
Focal increase 0 1 1
Cytochrome c-oxidase
Increased in periphery 1 0 0
Negative ibers 0 1 0
Table 3. Histological and histochemical abnormalities identiied in muscle biopsies from 19 cases of Pompe disease.*
Fig 1. Vacuoles of several size and location, variable amount of glycogen storage and acid phosphatase activity in adult-onset clinical forms of Pompe disease.
(A–C) Hematoxylin-eosin; (D–F) Periodic acid-schiff; (G–I) Acid phosphatase. Bar 100 micra.
A
B
C
D
E
F
G
H
I
iber types 1 and 2 occurred only in two adult cases. Internal nuclei and necrosis were found in half of the adult cases.
Seventeen of the 19 cases had a histological diagnosis of vacuolar myopathy, 1 with hypertrophy of type 1 and 2 fibers with focal increased acid phosphatase activity and another with chronic and active myopathy with focal in-creased acid phosphatase activity. These last two cases had a low blood GAA level, one of whom had no deoxyri-bonucleic acid (DNA) mutation detected.
DISCUSSION
In PD, GAA is unable to breakdown glycogen, leading to its accumulation in lysosomes. As the amount of glycogen in-creases in the lysosomes, they become larger and occasional-ly rupture their membranes, releasing and dispersing the free glycogen into the sarcoplasm, which displaces and disrupts the contractile apparatus. he glycogen accumulates in the sarcoplasm and causes secondary damage to the muscle cell8.
Muscle iber damage of muscle cell is not only by glycogen deposition. he accumulation of glycogen in vacuoles induces an autophagy (self-eating) process of the muscle iber, with formation of autophagic vacuoles originating from lysosomal
degradation. hese autophagic vacuoles acts in the sarco-plasm, damaging the muscle ibers, and contains heteroge-neous material from the cytoplasm, organelles degradation products, myeloid structures and lipofuccin detected by elec-tron microscopy. hese large autophagic vacuoles can occupy more than half of the iber diameter and interrupt the iber contractile apparatus8-10. Experimentally, in type 1 ibers, the
lysosomes are lined up and appear connected and enlarged, which is typical of Pompe disease. However, in type 2 ibers, they are randomly distributed, do not touch and become very large, with the appearance of large autophagic vacuoles11.
In our patients, the most common abnormalities in the mus-cle biopsies were vacuolated ibers illed with PAS-positive ma-terial (glycogen) and increased acid phosphatase activity, that was focal or difuse (positive ibers), similar to previous studies12.
Fig 2. Pompe disease (infantile form). Most of ibers sarcoplasm replaced by vacuoles illed with glycogen and with high activity of acid phosphatase. (A to C) two months-old; (D to F) ten months-old.
(A) Hematoxylin-eosin; (B and E) Periodic acid-schiff; (C and F) Acid phosphatase; (D) Modiied Gomori trichrome. Bar 100 micra.
Fig 3. Pompe disease (childhood form). Variations in iber diameter, ibers with and without vacuoles (small and large), vacuoles illed with glycogen, increased activity of acid phosphatase (focal or into vacuoles). (A to C) 7 years-old; (D to F) 11 years-old.
(A) Modiied Gomori trichrome; (B and E) Periodic acid-schiff; (C and F) Acid phosphatase; (D) Hematoxylin-eosin. Bar 100 micra.
A
B
C
D
E
F
A
B
C
D
E
F
he number of vacuolated ibers varies with the clinical type and disease duration. One of our cases had less than 1% vacuolated ibers, and no vacuoles were found in another, which has previ-ously been described. he vacuole frequency has been reported to range from present in nearly all ibers in the infantile form to 75% in the childhood form and 10–50% in adult patients. In in-fantile cases, the type 1 and 2 ibers are equally involved, while in the childhood and adult forms, the vacuoles are predominant in type 1 ibers in some cases and in type 2 ibers in others12-14.
he majority of our childhood and adult cases had a trophy of type 1 and 2 ibers, while three of nine adult cases
had hypertrophy of both iber types. hese data are similar to those reported in the literature13.
Muscle biopsy may be requested in cases of suspected PD, but it is not routine. Typically, the histological diagnosis of childhood or adult PD is made during the investigation of Duchenne muscular dystrophy with a normal DNA analysis for dystrophin, limb girdle muscular dystrophy or adult-onset myopathies, as in our cases and previously reported by several authors1,5,6. In the past, most infantile cases already had a
Fig 4. Pompe disease (adult form). Variations in iber diameter, vacuolated ibers illed with glycogen, increase activity of acid phosphatase (focal, diffuse and positive ibers) and splitting ibers. (A to C) 22 years-old; (D to F) 32 years-old; (G to I) 41 years-old.
(A) Hematoxylin-eosin; (B) Periodic acid-schiff; (C) Acid Phosphatase. Bar 100 micra.
A
B
C
D
E
F
G
H
I
was important to conirm the diagnosis. However, muscle bi-opsy is now infrequently performed in infantile cases because it has been replaced by the determination of GAA activity using a dried blood spot assay that is conirmed in blood leukocytes4.
Muscle biopsy abnormalities in PD vary with the level of GAA deiciency, the clinical type (which is related to the enzyme level) and the disease duration. he most important indings of
our study are as follows: (1) vacuoles with or without glycogen deposition (PAS+); (2) increased acid phosphatase activity, ei-ther in vacuoles or focal areas; (3) the adult form has fewer vacu-oles in the muscle ibers, and their histological indings resemble limb-girdle muscular dystrophy; (4) focal increases of acid phos-phatase activity in the muscle ibers of patients with limb-girdle syndrome raise the possibility of Pompe disease.
1. Bembi B, Cerini E, Danesino C, et al. Diagnosis of glycogenesis type II. Neurology 2008;71:S4-S11.
2. Ausems MG, Verbiest J, Hermans MP, et al. Frequency
of glucogen storage disease type II in The Netherlands: implication for diagnosis and genetic counseling. Eur J Hum Genet 1999;7:713-146.
3. Pinto R, Caseiro C, Lesmo M, et al. Prevalence of lysosomal storage disease in Portugal. Eur J Hum Genet 2004;12:87-92.
4. Wang RY, Bodamer OA, Watson MS, Wilcox WR; Work Group on
Diagnostic Conirmation of Lysosomal Storage Disease. Lysosomal storage diseases: diagnosis conirmation and management of presymptomatic individuals. Genet Med 2011;13:457-84.
5. Oba-Shinjo SM, da Silva R, Andrade FG, et al. Pompe disease in a Brazilian series: clinical and molecular analyses with identiication of nine new mutations. J Neurol 2009;256:1881-1890.
6. Angelini C, Nascimbeni AC. Late-onset GSDII with novel GAA gene mutation. Clin Genet 2007;71:374-375.
7. Werneck LC. The value of muscle biopsy in neurology: a study of 290 biopsies. Rev Bras Clin Ter 1981;10:S2-S24.
8. Lewandowska E, Wierzba-Bobrowicz T, Rola R, et al. Pathology of skeletal muscle cells in adult-onset glycogenosis type II (Pompe disease): ultrastructural study. Folia Neuropathol 2008;46:123-133.
9. Malicdan MC, Noguchi S, Nonaka I, Saftig P, Nishino I. Lysosomal myopathies: an excessive build-up in autophagosomes is too much to handle. Neuromuscul Disord 2008;28:521-529.
10. Shea L, Raben N. Autophagy in skeletal muscle: implication for Pompe disease. Int J Clin Pharmacol Ther 2009;47:S42-S47.
11. Raben N, Roberts A, Plotz PH. Role of autophagy in the pathogenesis of Pompe disease. Acta Mycologica 2007;26:45-48.
12. Schoser BGH, Müller-Höckert J, Horvath R, et al. Adult-onset glycogen storage disease type 2: clinic-pathological phenotype revisited. Neuropathol Applied Neurobiol 2007;33:544-559.
13. Papapetropoulos T, Paschalis C, Manda P. Myopathy due to juvenile acid maltase deiciency affecting exclusively the type 1 ibres. J Neurol Neurosurg Psychiatr 1984;47:213-215.
14. Van den Berg LEM, Vries JM, van der Ploeg AT, Reuser AJJ, Doorn PA. A case of adult Pompe disease presenting with severe fatigue and selective involvement of type 1 muscle ibers. Neuromuscul Disord 2011;21:232-234.