REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Association
of
clonidine
and
ropivacaine
in
brachial
plexus
block
for
shoulder
arthroscopy
Raphael
Faria-Silva
∗,
Daniel
Câmara
de
Rezende,
Juarez
Mundim
Ribeiro,
Telmo
Heleno
Gomes,
Braulio
Antônio
Maciel
Faria
Mota
Oliveira,
Fábio
Maciel
R.
Pereira,
Ildeu
Afonso
de
Almeida
Filho,
Antônio
Enéas
Rangel
de
Carvalho
Junior
HospitalFelícioRocho,BeloHorizonte,MG,Brazil
Received4January2013;accepted10June2013 Availableonline28November2014
KEYWORDS
Localanesthetics; Clonidine; Arthroscopy; Postoperativepain
Abstract
Backgroundandobjectives: Arthroscopyforshoulderdisordersisassociated withsevereand difficult tocontrol pain,postoperatively. Theaddition ofclonidine to local anestheticsfor peripheralnerveblockhasbecomeincreasinglycommon,thankstothepotentialabilityofthis drugtoreducethemassoflocalanestheticrequiredandtoprolonginganalgesiapostoperatively. Thepresentstudyaimedtoevaluatethesuccessofbrachialplexusblockforarthroscopicrotator cuffsurgeryusinglocalanestheticwithorwithoutclonidine.
Method: 53patientsofbothgenders,between18and70yearsold,AmericanSocietyof Anes-thesiologistsIorII,whowerescheduledtoundergoarthroscopicshouldersurgerywereselected. Patientswerethenrandomizedintotwogroups.Theverbalnumericalpainscaleandthe pres-enceofmotorblockwereobtainedinthepost-anestheticrecoveryroomand6,12,18and24h postoperatively.
Results:The associationofclonidine(0.15mg)toasolutionof0.33%ropivacaine(30mL)in brachialplexusblockforshoulderarthroscopyhasnotdiminishedthevisualnumericpainscale values, northeneedforopioidrescuepostoperatively.Therewasalowerincidenceof nau-sea/vomitingpostoperativelyandasignificantmotorblocktimeprolongationinthegroupof patientswhoreceivedclonidineasadjuvant.
Conclusions: Theuseofbrachialplexusblockwithlocalanestheticforanalgesicpostoperative controliswellestablishedintheliterature.Theadditionofclonidineinthedoseproposedfor prolongationoftheanalgesiceffectandreductionofopioidrescueprovedunhelpful. ©2014SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](R.Faria-Silva).
http://dx.doi.org/10.1016/j.bjane.2013.06.022
PALAVRAS-CHAVE
Anestésicoslocais; Clonidina;
Artroscopia; Dorpós-operatória
Associac¸ãodeclonidinaeropivacaínanobloqueiodeplexobraquialparaartroscopia deombro
Resumo
Justificativaeobjetivos: Aartroscopiaparaafecc¸õesdoombroassocia-seadordeforte inten-sidadeno pós-operatório, de difícil manejo. A adic¸ão de clonidinaao anestésico local em bloqueios periféricostornou-se progressivamente maiorgrac¸asà potencialhabilidade dessa drogade reduzir amassa deanestésicoslocais necessáriose prolongar aanalgesiano pós-operatório. O presente estudo teve como objetivo avaliar osucesso do bloqueio de plexo braquialparaacirurgiaartroscópicademanguitorotadorcomousodeanestésicolocal asso-ciadoounãoàclonidina.
Método: Foramselecionados53pacientesdeambosossexos,entre18e70anos,ASAIouII,que seriamsubmetidosàcirurgiadeombroporartroscopia.Ospacientesforamentãorandomizados emdoisgrupos.Aescalanuméricaverbaldedoreapresenc¸adebloqueiomotoreramobtidas nasaladerecuperac¸ãopós-anestésica(SRPA)comseis,12,18e24horasdepós-operatório.
Resultados: A associac¸ão de clonidina(0,15mg)àsoluc¸ão deropivacaína 0,33% (30mL)no bloqueiodeplexobraquialparaartroscopiadeombronãodiminuiuosvaloresdaescalavisual numéricadedor,nemanecessidadederesgatecomopioidesnopós-operatório.Houveuma menorincidênciadenáuseasevômitosnopós-operatório(NVPO)eaumentoconsideráveldo tempodebloqueiomotornogrupodepacientesquerecebeuclonidinacomoadjuvante.
Conclusões:Ousodobloqueiodeplexobraquialcomanestésicolocalparacontroleanalgésico pós-operatório estáconsolidado naliteratura. A adic¸ãode clonidinanadose propostapara prolongamentodoefeitoanalgésicoereduc¸ãoderesgatecomopioidesmostrou-sepoucoútil. ©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Brachial plexus blocks are indicated for anesthesia and analgesia in endoscopic procedures of the upper limb, shoulder, and clavicle. This anesthetic technique enables surgical procedureswithshort hospitalstay (noovernight stay)or anesthesiafor proceduresonan outpatientbasis, withconsequent costreduction.Itsanalgesic efficacyand lowincidenceofsideeffectsareimportantcharacteristics. Whenlongactinglocalanestheticsareused,evenatasingle dose,analgesiatimerangesbetween10and18h.Brachial plexusblockallowspainlessmanipulationinphysiotherapy, oftencriticalforrehabilitation.
Postoperativepainis perhapsthe maincomplicationof shoulderarthroscopyinvolvingtherotatorcuff.1The
periph-eralnerve block can provide adequate analgesia in early postoperativeperiodforupto20h.2Thesuccessofbrachial
plexusblockdependsonthevolumeofanestheticusedand onthesolutionconcentration.Theconcentrationisthemain determinantofmotorblockade.3
Clonidine,analpha-agonistwithpartialactiononalpha-2 receptors,hasbeenusedforyearsasacentrallyacting anti-hypertensive. Literaturereports on thepotential benefits ofadding clonidinetolocal anesthetics arecontroversial. The addition of clonidine to intermediate or long-acting localanesthetics forperipheral nerveor plexusblock pro-longsthedurationofanalgesiaandmotor blockfor about 2h.
Theuseofthisdruginblockadesincreasedprogressively due to its ability to reduce the mass of local anesthetic
required, as well as to prolong postoperative analgesia.4
This potentiatingeffectwasalsoseenwhenclonidinewas added to bupivacaine.5 Parenteral clonidine, muscle or
intravenouslyadministered,didnotshowthesamebenefit inperipheralnerveblockcomparedwithitslocaluse.5Most
resultsfound for clonidineshowsnoadverse effects,such ashypotensionorprolongedsedationwithitsuseinregional block.6,7Thecombinationofclonidinewithbupivacaine,for
example,prolongedtheanalgesiceffectofregional block-adefor3---4hwhenusedinthepoplitealfossainfootand anklesurgeries.2
However, Duma et al.8 reported that clonidine added
tolong-actinglocalanesthetic(bupivacaineor levobupiva-caine)produced noprolongedanalgesic effectonbrachial plexus block and increased the variability of patient response to local anesthetics, particularly to blockade latency. Moreover, the optimal dose of clonidine as an adjunct to blockade has not yet been defined.8 Dose
escalationisrelatedtoalargernumberofadverseeffects, mainlyrelatedtothedrugsystemicabsorption.
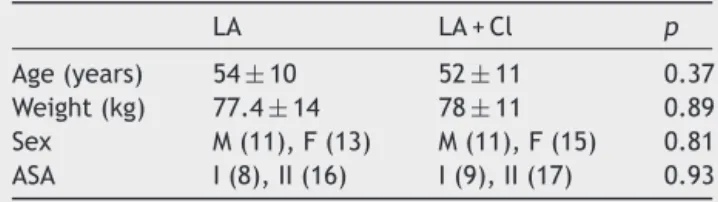
Table 1 Anthropometric data, gender distribution, and ASAphysicalstatus.
LA LA+Cl p
Age(years) 54±10 52±11 0.37
Weight(kg) 77.4±14 78±11 0.89
Sex M(11),F(13) M(11),F(15) 0.81 ASA I(8),II(16) I(9),II(17) 0.93
Valuesareexpressedasmean±SDorabsolutevalues. LA,localanesthetics;LA+Cl,localanestheticassociatedwith clonidine;ASA,AmericanSocietyofAnesthesiologists.
Method
ThisstudywasapprovedbytheInstitutionalEthicsResearch
Committee(HFR-CEP).
Initially,53patientsofbothsexes,agedbetween18and 70 years,classifiedby the AmericanSociety of Anesthesi-ologists(ASA)astypeIorII,scheduledtoundergoshoulder arthroscopy(Table1)wereselected.Patientswererandomly allocated to two groups. The investigator responsible for postoperative evaluationwasblinded togroup allocation. Allpatientssignedaninformedconsent.
Patientswithcardiac,respiratory,liverorkidneydisease; allergytolocalanestheticsandtheirdiluents;neuropathies or cognitivedeficits;bodymass indexhigherthan 45;and skin infection at the site of blockade, or contralateral hemidiaphragm paralysis were excluded from the study. Smokingwasnotacriterionforselectionofpatientsinthis studydesign.
The expectedeffects of using high doses of clonidine, suchassedationanddrymouth,werenotevaluatedinthis study,aspatients wereundergeneral anesthesia immedi-atelyaftertheblockade.Possiblecardiovasculareffectsof alpha-2agonistwerealsonotevaluatedbecausethegeneral anesthesiamaintenancedrugs(sevofluraneandsufentanil) couldbeconfoundingfactors.
Tocalculatethesample,weconsiderapowerof90%and asignificancelevelof5%,whichresultedinasamplesizeof 23patientspergroup.
During anesthesia, patients were monitored with elec-trocardiogram (DII,V5),pulseoximetry,noninvasiveblood pressure,capnography,andinhaledgasanalyzer. Premedi-cationwasperformedwith2mgintravenous(IV)midazolam. After brachial plexus block, balanced general anesthesia wasinducedwiththefollowingdrugs:propofol(3mgkg−1);
sufentanil (0.5gkg−1); cisatracurium (0.15mgkg−1);
sevoflurane(1MAC);dexamethasone(10mg);ondansetron (4mg);dipyrone(2000mg);ketoprofen(100mg);morphine (used only if required for rescue analgesia, 50gkg−1).
Localanesthetic solutionwas dilutedwith1% ropivacaine (10mL) (Cristália Laboratório Farmacêutico) and sterile bidistilledwater(20mL),totalingavolumeof30mLtobe injected.
Postoperatively on the ward, all patients received a fixed dose of IV dipyrone (2000mg) every 6h. Morphine (50gkg−1) wasused asrescue analgesia, whenever
nec-essary.
Protocol1:Effectof0.33%ropivacaineon postoperativeanalgesiainpatientsundergoing arthroscopicshouldersurgery
Initially, 26 patients were selected for control group. Brachialplexus blockwasperformedwithelectricalnerve stimulator (Stimuplex DIG; BBraun) and specific needle (StimuplexA50,BBraun).Afterproperlocationofthe injec-tion site, 30mL of 0.33% ropivacaine solution was used. Generalanesthesiawasperformedaftertheblockade.
Attheendofsurgery,presenceofpainwasassessedusing averbalnumericalpainscale(0:nopain,10:worstpossible pain).DuringPACUstay,iftherewasneedforrescue with IVmorphineatadosegreaterthan0.1mgkg−1,thepatient
wasexcluded fromthe protocol, and plexus blockfailure wasconsidered.
Verbalnumericalpainscaleandpresenceofmotorblock wereobtained in PACU and at six, 12, 18, and 24h after surgery.
Protocol2:Effectof0.33%ropivacaineand clonidine(0.15mg)onpostoperativeanalgesiain patientsundergoingarthroscopicshouldersurgery
Initially, 27 patients were selected for control group. Brachial plexus blockade was performed with electrical nervestimulator(StimuplexDIG;BBraun)andspecific nee-dle (Stimuplex A50, BBraun). After proper location of the anesthetic injection site, 30mL of 0.33% ropivacaine solutionand0.15mgofclonidine(CristáliaLaboratório Far-macêutico)wereused.Then,thepatientunderwentgeneral anesthesia.
Verbalnumericalpainscaleandpresenceofmotorblock were obtained in PACU and at six, 12, 18 and 24h after surgery.
Statisticalanalysis
Forcontinuousquantitative variables,the valuesare pre-sentedasmean±standarddeviationandcomparisonswere performedusingStudent’spairedt-test(normalvariables). Forordinalqualitativevariables,thevaluesarepresentedas medianandinterquartilerange,followedbyWilcoxontest (nonparametric variables) (Software GraphPadPrism 6.0). Thestatisticalsignificancecriterionwassetatp<0.05.
Results
Incontrol group,twopatients wereexcluded from analy-sis(onewaslosttopostoperativefollow-up,onewaslater consideredasASAIII).Inclonidinegroup,onepatientwas excluded fromanalysisbecause we considered that there wasablockadefailure(receivedmorphine>0.1mgkg−1in
PACU).
PACU 0
LA LACl
2 4 6 8 10
Time
Verbal rating pain scale
6h 12h 18h 24h
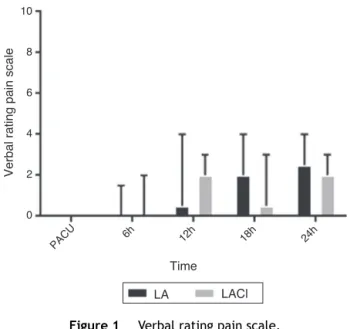
Figure1 Verbalratingpainscale.
wasnocomplicationrelatedtotheanesthetictechniquein anypatientundergoingtheexperimentalprotocol.
Brachial plexus block with 0.33% ropivacaine (30mL) provided satisfactory postoperative analgesia to patients studiedatallmeasuredtimes,asshowninFig.1.Thevisual analogpainscalereachedamedianvalueoftwoafter18h ofsurgery,whichisconsistentwiththehalf-lifeof ropiva-caine.Thesevaluesdonotdifferfromthoseusuallyfound intheliteratureforthistypeofprocedure.4Regardingthe
need formorphine rescue analgesia,themean numberof doses in this group was two (Table 2). Six patients (25%) hadpostoperativenauseaandvomiting(PONV)evenafter receiving adequate prophylaxis with dexamethasone and ondansetron.Themeandurationofmotorblockinthisgroup aftersurgerywas1.6h.Themeanhospitalstaywas20h.As almostallpatientsweredischargedbeforetheendofthe protocol,itwascontinuedbyactivesearchthroughphone call(20patientsincontrolgroupand22inclonidinegroup). In the second group, brachial plexus block with 0.33% ropivacaine(30mL)combinedwithclonidine(0.15mg) pro-videdsatisfactorypostoperativeanalgesiatopatientsatall measuredtimes,asshowninFig.1.Thevisualanalogpain scale wasnotstatisticallydifferent fromcontrolgroup at anystudiedtimes.
Regardingtheneedforrescueanalgesiawithmorphine, themeannumberofdosesinthisgroupwas1.1(Table2), also with no statistical difference compared to control
Table 2 Number of morphine rescue doses, incidence
of PONV, and mean time of motor block duration and hospitalization.
LA LA+Cl p
Morphinedoses(50gkg−1) 2
±2.9 1.1±1.4 0.16
PONV(n) 6 1 0.04
Motorblock(h) 1.6±2.5 7.4±5.2 0.01 Hospitalization(h) 20.7±6.5 18.8±3 0.24
Valuesareexpressedasmean±SD.
LA,localanesthetics;LA+Cl,localanestheticassociatedwith clonidine;PONV,postoperativenauseaandvomiting.
group. Regarding PONV, there was incidence in only one patient(3%)despite thestandard prophylaxis established. Themeandurationofresidualmotorblockadeaftertheend ofsurgerywas7.4h(approximately4.5timeslonger).The meanhospitalstaywas18.8h.Asinglepatientinthisgroup washospitalized for morethan one night,but thereason wasnotassociatedwithanesthesia.
Discussion
Thecombinationofclonidine(0.15mg)toasolutionof0.33% ropivacaine(30mL)inbrachialplexusblockforarthroscopic shoulder surgerydidnotdecreasethevaluesofthe visual numericpainscaleortheneedforpostoperativerescuewith opioids,aresultconsistentwithotherpublicationsthatused clonidine, evenat doses higherthan the one usedin this study.9---11
Adjuvant drugs are aimed at prolonging analgesia, improve quality or reduce the latency of blocksby local anesthetic. Adrenaline (in a concentration of 1:400,000---1:200,000), clonidine (0.5---1.0gkg−1), or opioids
(mor-phine, sufentanil, fentanyl, buprenorphine) may beused, however,withnoexcessivesedationorhypotension.12---14
Clonidineantinociceptivemechanismsarecontroversial, particularly regarding synergy with local anesthetics for peripheralblocks,asperipheralnerveaxonshavenoalpha-2 adrenergicreceptors.Despitehavingoriginallybeenusedas anantihypertensiveandnasaldecongestant,clonidineisan alpha-2adrenergicagonistusedasanadjuvanttolocal anes-thetics,particularlyinopioid-dependentpatients.15Nervous
conductiondelayorblockadethroughsodiumchannelsmay explaintheoriginofclonidine-inducedantinociception.The presenceofalpha-2agonistsreceptorsinperipheralnerves can be decisivein analgesic potentiation, but the results arestillcontroversial.16,17 Otherpossiblemechanismsmay
includelocalvasoconstrictoreffectoranalgesic effectson the central nervous system.5 Some authors suggest that
inflamedtissuesareconcomitantwithincreasedsensitivity of A-deltaandC painfibers,which iswhythe additionof clonidinewouldbepotentiallybeneficial.18
Thereisasignificantinteractionofclonidineadditionto localanesthetics in ocular blocks(retrobulbar,peribulbar, andsubtenon),whichleadstoakinesiaandprolongationof analgesia.19 Itsanalgesic potentiationhas been described
when it wasadministered in the intrathecal and epidural space(spinalanesthesia),particularlyassociatedwith short-actinglocalanesthetics.20
Regardingtheidealdrugcombination,clonidineappears tohavegreater adjuvantbenefitwithintermediate-acting localanesthetics,suchaslidocaineandmepivacaine.A sys-tematic literature review evaluated 27 studies, of which 15 had positive and 12 negative results on the addition of clonidine.16 It seemsthat there are noside effects at
doses up to 0.15mg. Moreover, clonidine seems tobe of greater benefitwhen added toupper compared to lower limbblocks.16
There is evidence in the literature that favors the addition of clonidine to reduce the latency of peripheral nervous block with ropivacaine when this drug is used for anesthesia.21 However, the results are controversial
reportedthatclonidineincreasedtheanalgesiceffecttime ofropivacaineby20%afterlowerlimbsurgery.
In ourstudy,wefound alowerincidenceof PONV.The smokingvariablewasnotstudied,aknownprotectivefactor againstPONV,22whichmayinterferewiththeresults.
Clonidine, when given orally as premedication, was effectiveasanadjuvantdrugtoreducePONVinophthalmic pediatric surgery.23 Similar effect was also seen in
oto-logic surgery24 and to prevent postoperative nausea and
tremorsof elderly patientsundergoing neuraxialblocks.25
As asingledrug for PONVprophylaxis, itseffectis notas evident.26 Clonidine alsoshowedbenefitinreducingPONV
when usedin theanesthetic induction of patients under-going mastectomy,27 without an increase of sedation or
theemergence ofother significantadverse effects.In the genesisofPONVappearstobeanadrenergicautonomic dys-functioncomponent,forwhichreasontheuseofclonidine appeartobebeneficial.28
Clonidine is a medication of lower cost than the antiemeticdrugsactingthrough5-HT3,suchasondansetron anditssimilar.However,webelievethatitsrealbenefitas asingledrugforPONVprophylaxisissmallandalsothatitis notusedroutinelyinmostanesthesiaservicesforthis pur-pose. Furthermore,this drug potentialantiemetic benefit can beobtained byoral or venous administrationwithout theneedtoaddittothelocalanestheticsolution.
Therewasaconsiderableincreaseinmotorblock dura-tioninpatientsreceivingclonidineasanadjuvant.Thereis evidencein the literatureonprolongation of motorblock ofbupivacaineandmepivacainebyalpha-2agonist.6,29The
questiontobeposedisabouttheactualbenefitofthis pro-longedmotorblock,astheneedforrescue withopioidsis notreduced.Inouropinion,postoperativeprolongedmotor blockonlyincreasespatientanxiety,withoutprovidingreal anestheticorsurgicalbenefit.Thisopinionisalsosharedby other authors.30 In selected cases,it may evendelay the
recoveryprocess,whenwe considertherealpossibilityof earlyphysiotherapy.
There was no difference regarding patient’s hospital-ization.Therefore,clonidinedidnot affecttheprocedure operatingcost.
The use of brachial plexus block with local anesthetic forpostoperativeanalgesicmanagementisconsolidatedin the literature. However, the addition of clonidine at the dose proposedtoprolong theanalgesic effectandreduce the rescue with opioids in the present study population provedtobeoflittlebenefitforbrachialplexusblockThere are other drugs whose additive utility remains uncertain (tramadol, calcium channel blockers, neostigmine, dexa-methasone,hyaluronidase, NaHCO3)and that may be the
subjectoffuturestudies.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.CruvinelMC,CastroCH,SilvaYP.Estudocomparativodaeficácia analgésicapós-operatóriade20,30ou40mLderopivacaínano
bloqueiodeplexobraquialpelaviaposterior.RevBras Aneste-siol.2007;57:500---13.
2.YadeauJT, LasalaVR. Clonidineand analgesicduration after popliteal fossa nerve blockade: randomized, double-blind, placebo-controlledstudy.AnesthAnalg.2008;106:1916---20. 3.FredricksonMJ.Importanceofvolumeand concentrationfor
ropivacaineinterscaleneblockinpreventingrecoveryroompain andminimizingmotorblockaftershouldersurgery. Anesthesi-ology.2010;112:1374---81.
4.ElSaiedAH,Steyn MP.Clonidineprolongstheeffectof ropi-vacaineforaxillarybrachialplexusblockade.CanJAnaesth. 2000;47:962---7.
5.Helayel PK,Boos GL,JahnsMT. Efeitosda clonidinapor via musculareperineuralnobloqueiodonervoisquiáticocom ropi-vacaínaa0,5%.RevBrasAnestesiol.2005;55:483---90.
6.Eledjam JJ, Deschodt J. Brachial plexus block with bupi-vacaine: effects of added alpha-adrenergic agonists: com-parison between clonidine and epinephrine. Can J Anaesth. 1991;38:870---5.
7.Casati A, Magistris L. Small-dose clonidine prolongs post-operative analgesia after sciatic-femoral nerve block with 0.75% ropivacaine for foot surgery. Anesth Analg. 2000;91: 388---92.
8.DumaA,UrbanekB,SitzwohlC,etal.Clonidineasanadjuvant tolocalanaestheticaxillarybrachialplexusblock:a random-ized,controlledstudy.BrJAnaesth.2005;94:112---6.
9.EstevesS, SáP,Figueiredo D,et al. Durationand qualityof postoperativeanalgesiaafterbrachialplexusblockforshoulder surgery: ropivacaine0.5%versus ropivacaine0.5%plus cloni-dine.RevEspAnestesiolReanim.2002;49:302---5.
10.TrifaM,BenKhalifaS, JendoubiA,et al.Clonidinedoesnot improvequalityofropivacaineaxillarybrachialplexusblockin children.PaediatrAnaesth.2012;22:425---9.
11.Pinto Neto W, IssyAS, Sakata RK. Estudocomparativoentre clonidinaassociadaàbupivacaínaebupivacaínaisoladaem blo-queiodeplexocervicalparaendarterectomiadecarótida.Rev BrasAnestesiol.2009;59:387---95.
12.CandidoKD,FrancoCD,KhanMA,etal.Buprenorphineadded to the local anesthetic for brachial plexus block to provide postoperative analgesiainoutpatients.Reg Anesth Pain Med. 2001;26:352---6.
13.BazinJE,MassoniC,BruelleP,etal. Theaddition ofopioids to local anaesthetics in brachial plexus block: the com-parative effects of morphine and sufentanil. Anaesthesia. 1997;52:858---62.
14.Novelo B,RojasE,Romero I.Bloqueodelplexobraquialcon lidocaina másopioidespara disminuireltiempode latencia. RevMexAnest.1996;19:28---31.
15.Gaumann DM, Brunet PC, Jirounek P. Hyperpolarizing after potentialsinCfibersandlocalanestheticeffectsofclonidine andlidocaine.Pharmacology.1994;48:21---9.
16.McCartney CJ, Duggan E,Apatu E.Should we addclonidine to localanesthetic for peripheral nerve blocking? A qualita-tivesystemicreviewoftheliterature.RegAnesth PainMed. 2007;32:330---8.
17.Yoshitomi T, Kohjitani A, Maeda S, et al. Dexmedetomidine enhancesthelocalanestheticactionoflidocaineviaan alpha-2Aadrenoceptor.AnesthAnalg.2008;107:96---101.
18.Iohom G, Machmachi A, Diarra DP, et al. The effects of clonidine added to mepivacaine for paronychia surgery underaxillarybrachialplexusblock.AnesthAnalg.2005;100: 1179---83.
19.WoldemussieE,WijonoM,PowD.Localizationofalpha2 recep-torsinoculartissues.VisNeurosci.2007;24:745---56.
21.HutschalaD,MascherH,SchmettererL,etal.Clonidineadded tobupivacaineenhancesandprolongsanalgesiaafterbrachial plexusblockviaalocalmechanisminhealthyvolunteers.EurJ Anaesthesiol.2004;21:198---204.
22.AbreuMP.Controledenáuseasevômitos.Antieméticos.In: Can-gianiLM,etal.,editors.Tratadodeanestesiologia.SãoPaulo: Atheneu;2006.p.1361---72.
23.HandaF,FujiiY.Theefficacyoforalclonidinepremedicationin thepreventionofpostoperativevomitinginchildrenfollowing strabismussurgery.PaediatrAnaesth.2001;11:71---4.
24.TaheriA,JavadimaneshMA,AshrafH.Theeffectoforal cloni-dinepremedicationonnauseaandvomitingafterearsurgery. MiddleEastJAnesthesiol.2010;20:691---4.
25.ZhaoH,Ishiyama T,Oguchi T,etal. Effectsofclonidineand midazolamonpostoperativeshivering,nausea,and vomiting. Masui.2005;54:1253---7.
26.Gulhas N, Turkoz A, Durmus M, et al. Oral clonidine premedicationdoesnotreducepostoperativevomitingin chil-drenundergoingstrabismussurgery.ActaAnaesthesiolScand. 2003;47:90---3.
27.Oddby-MuhrbeckE,EksborgS,BergendahlHT,etal.Effectsof clonidineonpostoperativenauseaandvomitinginbreastcancer surgery.Anesthesiology.2002;96:1109---14.
28.PalmerGM, Cameron DJ. Useof intravenous midazolamand clonidineincyclicalvomitingsyndrome:acasereport.Paediatr Anaesth.2005;15:68---72.
29.PöppingDM.Clonidineasanadjuvanttolocalanestheticsfor peripheralnerveandplexusblocks:ameta-analysisof random-izedtrials.Anesthesiology.2009;111:406---15.