DEVELOPI NG A COMPARATI VE SCALE OF DI FFERENT NOCI CEPTI VE AND NEUROPATHI C
PAI N THROUGH TW O PSYCHOPHYSI CAL METHODS
Pr iscilla Hor t ense1 Fát im a Apar ecida Em m Faleir os Sousa2
Hor t ense P, Sousa FAEF. Dev eloping a com par at ive scale of differ ent nocicept iv e and neur opat hic pain t hr ough t w o psy chophy sical m et hods. Rev Lat ino- am Enfer m agem 2009 m ar ço- abr il; 17( 2) : 207- 214.
The gener al aim of t his st udy w as t o cr eat e a com par at iv e scale of differ ent t y pes of pain t hr ough differ ent psy chophy sical m et hods and differ ent sam ples. The psy chophy sical m et hods used w er e m agnit ude est im at ion and cat egor y est im at ion. The par t icipant s w er e 30 pat ient s fr om differ ent out pat ient clinics, 30 physicians and 30 nurses. The result s were: 1) cancer pain, m yocardial infarct ion pain, renal colic, burn- inj ury pain, and labor pain w er e consider ed m or e int ense, r egar dless of t he psy chophy sical m et hod used or sam ple st udied; 2) The ranking of different pain int ensit ies, com paring t he different psychophysical m et hods used, result ed in significant agreem ent levels wit h Kendal values close t o 1.00; 3) There were divergences in t he percept ion of t he int ensit ies of som e t y pes of pain. These div er gences w er e especially obser v ed bet w een pr ofessionals and pat ient s.
DESCRI PTORS: pain m easu r em en t ; psy ch oph y sics
ESCALONAMI ENTO COMPARATI VO DE DI FERENTES DOLORES NOCI CEPTI VOS Y
NEUROPÁTI COS POR MEDI O DE MÉTODOS PSI COFÍ SI COS VARI ADOS
El obj et iv o gener al fue escalonar los difer ent es t ipos de dolor ex ist ent es, com par ándolos ent r e ellos, siendo invest igados por m edio de diferent es m ét odos psicofísicos. Los m ét odos psicofísicos ut ilizados fueron el m ét odo de est im ación de m agnit udes y el de est im ación de cat egor ías. Par t icipar on 30 pacient es de am bulat or io de difer ent es clínicas, 30 m édicos y 30 enfer m er os. Los r esult ados m ost r ar on que el dolor causado por : cáncer , in f ar t o d el m iocar d io, cólico r en al, q u em ad u r a y p ar t o, f u er on con sid er ad os los t ip os d e d olor d e m ay or int ensidad, independient em ent e del m ét odo psicofísico ut ilizado o de la m uest ra est udiada. El orden de posiciones d e in t en sid ad d e los d if er en t es t ip os d e d olor , com p ar an d o los d if er en t es m ét od os p sicof ísicos u t ilizad os, r esult ar on en niv eles de concor dancia significat iv a con v alor es de Kendal pr óx im os de 1 , 0 0 . Se encont r ar on divergencias en la percepción de las int ensidades de algunos t ipos de dolor, est as divergencias fueron observadas pr in cipalm en t e en t r e pr ofesion ales y pacien t es.
DESCRI PTORES: dim ensión del dolor ; psicofísica
ESCALONAMENTO COMPARATI VO DE DI FERENTES DORES NOCI CEPTI VAS E
NEUROPÁTI CAS POR MEI O DE MÉTODOS PSI COFÍ SI COS VARI ADOS
O obj et ivo geral foi escalonar os diferent es t ipos de dor exist ent es, com parat ivam ent e ent re si, sendo invest igados por m eio de difer ent es m ét odos psicofísicos. Os m ét odos psicofísicos ut ilizados for am o m ét odo de est im ação de m agnit udes e o de est im ação de cat egor ias. Par t icipar am 30 pacient es am bulat or iais de difer ent es clínicas, 30 m édicos e 30 enfer m eir os. Os r esult ados m ost r ar am que a dor no câncer , dor por infar t o do m iocár dio, a d or p or cólica r en al, d or p or q u eim ad u r a e a d or n o p ar t o f or am con sid er ad as os t ip os d e d or d e m aior int ensidade, independent e do m ét odo psicofísico ut ilizado ou da am ost r a est udada. As or denações de posições da int ensidade dos diferent es t ipos de dor, com parando os diferent es m ét odos psicofísicos ut ilizados, result aram em n ív eis d e con cor d ân cia sig n if icat iv a com v alor es d e Ken d al p r óx im os d e 1 , 0 0 . Hou v e d iv er g ên cias n a per cepção das int ensidades de alguns t ipos de dor , essas diver gências for am obser vadas pr incipalm ent e ent r e pr ofission ais e pacien t es.
DESCRI TORES: m edição da dor ; psicofísica
1Ph.D. in Nursing, Facult y, Cent ro Universit ário de Araraquara, Brazil, e- m ail: prihrt @yahoo.com .br; 2Associat e Professor, Escola de Enferm agem de Ribeirão Pret o, da Universidade de São Paulo, Cent ro Colaborador da OMS para o Desenvolvim ent o da Pesquisa em Enferm agem , Ribeirão Pret o, SP, Brazil, e- m ail: [email protected].
I NTRODUCTI ON
H
eal t h p r o f essi o n al s’ m ai n f u n ct i o n i s t o allev iat e pain an d su f f er in g. For t h at , t h ey n eed t og e t r i d o f b e l i e f s , p r e c o n c e p t i o n s a n d p r e v i o u s
in d iv id u al ex p er ien ces, an d u n d er st an d t h e p at ien t
w it h pain in h is( er ) t ot alit y as a u n iqu e bein g w it h
par t icu lar ch ar act er ist ics.
I n addit ion t o underst anding som eone’s pain,
it is also im port ant t o underst and t he person per se,
w hat t his per son per ceiv es and feels and how ( s) he
deals w it h t hese feelings( 1).
Pa i n i s co m p o se d o f t w o e l e m e n t s: “ t h e
original sensat ion and t he react ion t o t his sensat ion”,
t hat is, response t o a painful sensat ion depends on a
series of individual int rinsic and ext rinsic aspect s. Thus,
m easur ing a painful sensat ion is a com plex t ask( 2).
Th e h i s t o r y o f p a i n m e a s u r e m e n t w a s
a n a l y z e d a n d t h r e e b r a n c h e s o f a c t i v i t y w e r e
ident ified, which are: psychophysics, m ult idim ensional
q u est ion n air es u sin g st an d ar d ized d escr ip t or s an d
i n t e n si t y sca l e s( 3 ). Th e a u t h o r s r e p o r t t h a t su ch
h ist or ical con cer n ar ises fr om t h e n eed t o est ablish
r eliable, v alid an d sen sit iv e m easu r es t o defin e t h e
efficacy of analgesics and ot her t her apies.
There are som e st udies in t he psychophysics
a r e a f o c u s i n g o n p a i n p e r c e p t i o n , w h i c h u s e
ex p er i m en t al p ai n i n d u ct i o n i n d i f f er en t sam p l es,
a i m i n g t o c o m p a r e “ r e a c t i o n s t o s e n s a t i o n s ” .
Psy chophy sics defines t he t hr eshold and t oler ance t o
p ain b y in d u cin g ex p er im en t al p ain an d com p ar in g
e t h n i c a l g r o u p s , g e n d e r s a t d i f f e r e n t a g e s a n d
differ ent life habit s, am ong ot her s v ar iables( 4- 5).
I n addit ion, t he psy chophy sical m et hod can
be used in st udies on clinical pain t hat r esult s fr om
pat hological condit ions. The psychophysical law is also
k n ow n as St ev en s’ p ow er law . I t is r elat ed t o t h e
psy ch ological m agn it u de an d ph y sical in t en sit y of a
st im ulus and can be descr ibed by a pow er funct ion,
w hich r elat es st im ulus and subj ect iv e r esponse in a
cur v e( 6- 7).
This funct ion describes a sit uat ion in which a
geom et ric increase in physical m agnit ude corresponds
t o a g e o m e t r i c i n c r e a s e o n t h e s u b j e c t i v e o r
psy ch ological scale. I t s ex pon en t r ef lect s a r elat iv e
r at e of in cr ease bet w een t h e t w o scales an d, t h u s,
t he principle t hat equal rat ios bet ween st im uli produce
equal r at ios bet w een r esponses( 7 ).
I n t h e m a g n i t u d e e s t i m a t i o n m e t h o d ,
e l a b o r a t e d b y S t e v e n s ’ M o d e r n Ps y c h o p h y s i c s ,
in div idu als select an d u se a r an ge of n u m ber s t h at
r epr esent t heir subj ect iv e am plit ude. Opposed t o t his
m et hod is t he cat egor y est im at ion m et hod, in w hich
t h e ex p er im en t er ar b it r ar ily ch ooses t h e am p lit u d e
of cat egor ies( 6- 7).
Th is m et h od h as im p or t an t ch ar act er ist ics,
such as t he st r at egy t o m easur e subj ect iv e concept s
l i k e p a i n . So m e o f t h ese ch a r a ct er i st i cs a r e: t h e
pr oduct ion of scales as r at ios incr eases t he sensit iv it y
of m easur em ent ; r esult ing scales and j udgm ent s ar e
r epr oducible, st able, w it h r ecor ds of t est and r e- t est
and r eliabilit y coefficient s close t o 0.908; t he t est is
cost - ef f icien t b ecau se t h er e is n o loss of d at a an d
dat a can be indiv idually or collect iv ely collect ed( 6- 8).
Th e p sy ch op h y sical m et h od is u sed in t h is
st u dy t o im pr ov e t h e k n ow ledge on t h is su bj ect iv e
an d per cept u al ph en om en on . Th e differ en t t y pes of
pain , com par ed am on g t h em an d bet w een differ en t
sam ples ( pr ofessionals and pat ient s) w er e: low back
pain, headache, j oint pain, bur n- inj ur y pain, pain in
p e r i p h e r a l n e u r o p a t h y, p a i n i n r e p e t i t i v e m o t i o n
d isor d er, p ain in AI DS, p ost op er at iv e p ain , can cer
p ai n , l ab or p ai n , p ai n i n t em p or om an d i b u l ar j oi n t
d isor d er ( TMJ) , h er p es- zost er, t r ig em in al n eu r alg ia
( facial pain) , fibr om y algia, m y ocar dial infar ct ion pain,
r e n a l co l i c, p a i n i n st o m a ch u l ce r, b i l i a r y co l i c,
m en st r u al colic an d t oot h ach e.
OBJECTI VE
Dev elopin g a com par at iv e scale of differ en t
pain t y pes t hr ough differ ent psy chophy sical m et hods.
PAI N MEASUREMENT
Co m p a r i s o n b e t w e e n p s y c h o p h y s i c a l s c a l i n g
m e t h o d s : m a g n i t u d e e s t i m a t i o n a n d c a t e g o r y
est im at ion
The int ensit y of differ ent t y pes of pain w as
ev alu at ed t h r ou g h t w o in d ep en d en t p sy ch op h y sical
m e t h o d s : m a g n i t u d e e s t i m a t i o n a n d c a t e g o r y
est im at ion .
Ob j ect i v es
- t o com par e scaling of v ar ious pain t y pes bet w een
- t o com pare t he scale derived from ordinal j udgm ent s
( cat eg o r y est i m at es) w i t h t h e scal e d er i v ed f r o m
j udgm ent r at ios ( m agnit ude est im at es) in t he t hr ee
st u died sam ples;
- t o verify whet her rankings of pain int ensit ies deriving
f r o m t h e t w o m et h o d s a r e si m i l a r i n t h e st u d i ed
sam p l es.
METHOD
Par t icip an t s: 3 0 p at ien t s f r om d if f er en t ou t p at ien t
clinics and 60 healt h professionals ( 30 physicians and
30 nur ses fr om t he Hospit al das Clinicas, Univ er sit y
of São Pau lo at Rib eir ão Pr et o Med ical Sch ool, SP,
Br azil) .
Ma t e r i a l : p e n a n d n o t e b o o k c o n t a i n i n g s p e c i f i c
inst r uct ions for each t y pe of psy chophy sical m et hod
on t he fir st page and a list of 2 0 differ ent t y pes of
pain and t heir r espect iv e definit ions on t he follow ing
p ag es.
Pr oced u r e: t h e p sy ch op h y sical m et h od s u sed w er e
m agnit ude est im at ion and cat egor y est im at ion.
Th e p a r t i c i p a n t s ’ t a s k i n t h e m a g n i t u d e
est im at ion m et hod consist ed of at t r ibut ing a num ber
( n u m e r i ca l v a l u e o f 1 0 0 ) t o e a ch t y p e o f p a i n ,
p r o p o r t i o n al t o t h e i n t en si t y o f p ai n i t p o ssesses
com par ed t o t h e st an dar d st im u lu s, w h ich w as low
back pain. For ex am ple, if t he par t icipant consider ed
a g iv en t y p e of p ain t w o t im es m or e in t en se t h an
low back pain , ( s) h e should at t r ibu t e a nu m ber t w o
t i m e s l a r g e r, t h a t i s , 2 0 0 . I f t h e p a r t i c i p a n t
co n si d er ed t h at a cer t ai n t y p e o f p a i n p o ssessed
h alf of t h e in t en sit y of low back pain , ( s) h e sh ou ld
at t r ib u t e a n u m b er r ep r esen t in g h alf of it , t h at is,
5 0 . Par t icipan t s est ablish ed 2 0 est im at ion s, on e for
each t y pe of pain .
I n t he second m et hod, t he par t icipant s’ t ask
w as t o scor e fr om one t o sev en, each differ ent t y pe
o f p ai n b ased o n t h e p er cei v ed i n t en si t y o f p ai n .
Pa r t i ci p a n t s w e r e a sk e d t o a ssi g n t h e m a x i m u m
scor e ( sev en ) t o t h e t y pe of pain w it h t h e h igh est
int ensit y and assign t he m inim um scor e ( one) t o t he
t y p e o f p a i n w i t h t h e l o w est i n t en si t y. Th e o t h er
in t er m ediar y scor es, t w o t o six , sh ou ld be u sed t o
indicat e int er m ediar y degr ees of int ensit y accor ding
t o p ar t icip an t s’ p er cep t ion s. Th e d if f er en t t y p es of
p ain w er e r an d om ly p r esen t ed t o each in d iv id u al.
Each in div idu al est ablish ed on e scor e for each t y pe
of pain .
Fo r t h e m a g n i t u d e e st i m a t e s, g e o m e t r i c
a v e r a g e s a n d s t a n d a r d d e v i a t i o n s o f g e o m e t r i c
av er ages for each t y pe of pain w er e com put ed. For
t h e c a t e g o r y e s t i m a t e s , a v e r a g e a n d s t a n d a r d
dev iat ions w er e also calculat ed for each t y pe of pain.
I n addit ion , Kr u sk al- Wallis’ n on - par am et r ic t est an d
Mann- Whit ney ’s t est w er e com put ed t o com par e pain
i n t e n s i t i e s b e t w e e n s a m p l e s . K e n d a l l ’ s W w a s
com put ed t o com par e concor dance bet w een t he used
m et h o d s.
RESULTS
Th e r e su l t s p r e se n t e d i n Ta b l e s 1 a n d 2
cor r espon d t o t h e scalin g of dif f er en t pain t y pes in
decr escen t or der, t h at is, f r om t h e pain con sider ed
of h igh est in t en sit y t o t h e on e con sider ed of low est
i n t e n si t y. Th e sca l i n g i s p r e se n t e d a cco r d i n g t o
t h r e e s t u d i e d s a m p l e s : o u t p a t i e n t s ’ g r o u p ,
p h y sician s’ g r ou p s an d n u r ses’ g r ou p . Scalin g w as
p e r f o r m e d t h r o u g h t w o m e a s u r e m e n t m e t h o d s :
m a g n i t u d e e s t i m a t e s ( Ta b l e 1 ) a n d c a t e g o r y
est im at es ( Tab le 2 ) .
The t y pes of pain t he out pat ient s consider ed
of highest int ensit y, bot h in t he m agnit ude est im at ion
and cat egor y est im at ion m et hods, w er e cancer pain,
r en al colic, m y ocar d ial in f ar ct ion p ain an d p ain in
A I D S . Th e t y p e s o f p a i n c o n s i d e r e d o f h i g h e s t
in t en sit y by t h e ph y sician an d n u r sin g gr ou ps w er e
equiv alent . They w er e: cancer pain, r enal colic, labor
pain, m y ocar dial infar ct ion pain and bur n- inj ur y pain
( Tables 1 and 2) .
I t is w or t h m ent ioning t hat cancer pain w as
consider ed by t he t hr ee sam ples as one of t he m ost
i n t e n s e p a i n t y p e s i n t h e t w o m e t h o d s u s e d
( m agnit ude est im at ion and cat egor y est im at ion) and
w as consider ed t he m ost int ense in t he out pat ient s’
and nur ses’ gr oups and t he second m ost int ense in
t h e ph y sician s’ gr ou p.
Th e t y p e s o f p a i n c o n s i d e r e d o f l o w e s t
i n t e n s i t y b y t h e o u t p a t i e n t g r o u p , b o t h i n t h e
m agnit ude est im at ion and in t he cat egor y est im at ion
m et hods, were pain by repet it ive m ot ion disorder, pain
in TMJ disorder, low back pain and headache; for t he
physicians’ group, t hey were repet it ive m ot ion disorder
m enst rual colic; and for t he nurses’ gr oup, t hey w er e
m en st r u al co l i c, l o w b ack p ai n , r ep et i t i v e m o t i o n
disor der pain , pain in TMJ disor der an d t oot h pain .
Kr usk al- Wallis’ non- param et r ic t est w as used
for each t y pe of pain, com par ing t he st udied sam ples
in each of t h e m et h od s u sed . Wh en t h e d if f er en ce
b et w een sam p les w as st at ist ically sig n if ican t , w it h
p < 0 . 0 5 , Ma n n - W h i t n ey ’ s p a i r ed t est w a s u sed t o
co m p a r e p a i n sco r es b et w een sa m p l es ( p a t i en t
s-p h y si ci a n s; s-p a t i e n t s- n u r se s; n u r se s- s-p h y si ci a n s) .
Tables 1 an d 2 sh ow t h e p- v alu es f or each t y pe of
pain. Nex t , t he t y pes of pain t hat pr esent ed scor es
w it h st at ist ically sign ifican t differ en ces bet w een t h e
st u died sam ples ar e pr esen t ed.
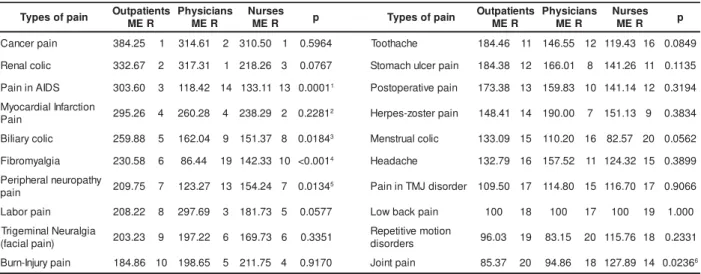
Tab le 1 – Geom et r ic av er ag e of m ag n it u d e est im at es ( ME) f or t h e d if f er en t t y p es of p ain b y r an k in g ( R)
accor ding t o out pat ient s, phy sicians and nur ses HCFMRP/ USP, 2007
1- Pain in AI DS – st at ist ically significant differences bet ween pat ient s- physicians and bet ween pat ient s- nurses, p< 0.017. 2- Myocardial infarct ion pain – st at ist ically significant differences bet ween pat ient s- nurses, p< 0.017.
3- Biliary colic – st at ist ically significant differences bet ween pat ient s- nurses, p< 0.017. 4- Fibrom yalgia – st at ist ically significant differences bet ween pat ient s- physicians, p< 0.017.
5- Peripheral neuropat hy pain – st at ist ically significant differences bet ween pat ient s- physicians, p< 0.017. 6- Joint pain – st at ist ically significant differences bet ween pat ient s- nurses, p< 0.017.
Table 2 – Geom et ric average of cat egory est im at es ( CE) for t he different t ypes of pain by ranking ( R) according
t o out pat ient s, phy sicians and nur ses. HCFMRP/ USP, 2007
1- Pain in AI DS – st at ist ically significant differences bet ween pat ient s- physicians, bet ween pat ient s- nurses and bet ween physicians- nurses, p< 0.017. 2- Fibrom yalgia – st at ist ically significant differences bet ween pat ient s- physicians and bet ween physicians- nurses, p< 0.017.
3- Joint pain – st at ist ically significant differences bet ween pat ient s- physicians and bet ween physicians- nurses, p< 0.017. 4- Low back pain – st at ist ically significant differences bet ween pat ient s- physicians, p< 0.017.
5- Repet it ive m ot ion disorders – st at ist ically significant differences bet ween physicians- nurses, p< 0.017. n i a p f o s e p y
T OutpatientsCER PhysiciansCER NursesCER p
n i a p r e c n a
C 6.20 1 6.13 2 6.33 1 0.6203
n i a p n o it c r a f n i l a i d r a c o y
M 6.10 2 5.57 4 6.03 2 0.1124
S D I A n i n i a
P 5.83 3 3.80 15 4.77 9 <0.0011
n i a p y r u j n i -n r u
B 5.83 4 5.13 5 5.60 4 0.3673
c il o c l a n e
R 5.63 5 6.17 1 5.70 3 0.1881
a i g l a y m o r b i
F 5.37 6 3.33 19 4.77 8 <0.0012
) n i a p l a i c a f ( a i g l a r u e n l a n i m e g i r
T 5.27 7 5.10 6 4.60 11 0.2171
n i a p r o b a
L 5.20 8 5.93 3 5.17 5 0.1332
c il o c y r a il i
B 4.90 9 4.40 12 4.70 10 0.3506
n i a p e v it a r e p o t s o
P 4.87 10 4.67 8 4.93 6 0.4530
e h c a h t o o
T 4.83 11 4 14 4.07 17 0.0533
n i a p y h t a p o r u e n l a r e h p i r e
P 4.83 12 4 11 4.77 7 0.0598
n i a p r e t s o z -s e p r e
H 4.57 13 4.50 10 4.47 13 0.9248
n i a p t n i o
J 4.37 14 3.67 17 4.57 12 0.00303
n i a p r e c l u h c a m o t
S 4.33 15 4.80 7 4.40 14 0.9171
e h c a d a e
H 4.27 16 4.67 9 4.20 15 0.9608
n i a p k c a b w o
L 4.13 17 3.47 18 4.10 16 0.03234
r e d r o s i d J M T n i n i a
P 4.07 18 4.27 13 3.93 18 0.7705
c il o c l a u r t s n e
M 4. 19 3.77 16 3.33 20 0.2584
s r e d r o s i d n o it o m e v it it e p e
R 3.77 20 3.13 20 3.87 19 0.02715
n i a p f o s e p y
T Outpatients R E M s n a i c i s y h P R E M s e s r u N R E
M p Typesofpain
s t n e i t a p t u O R E M s n a i c i s y h P R E M s e s r u N R E M p n i a p r e c n a
C 384.25 1 314.61 2 310.50 1 0.5964 Toothache 184.46 11 146.55 12 119.43 16 0.0849
c il o c l a n e
R 332.67 2 317.31 1 218.26 3 0.0767 Stomachulcerpain 184.38 12 166.01 8 141.26 11 0.1135
S D I A n i n i a
P 303.60 3 118.42 14 133.11 13 0.00011 Postoperaitvepain 173.38 13 159.83 10 141.14 12 0.3194
n o it c r a f n I l a i d r a c o y M n i a
P 295.26 4 260.28 4 238.29 2 0.22812 Herpes-zosterpain 148.41 14 190.00 7 151.13 9 0.3834
c il o c y r a il i
B 259.88 5 162.04 9 151.37 8 0.01843 Menstrualcoilc 133.09 15 110.20 16 82.57 20 0.0562
a i g l a y m o r b i
F 230.58 6 86.44 19 142.33 10 <0.0014 Headache 132.79 16 157.52 11 124.32 15 0.3899
y h t a p o r u e n l a r e h p i r e P n i a
p 209.75 7 123.27 13 154.24 7 0.01345 PaininTMJdisorder 109.50 17 114.80 15 116.70 17 0.9066
n i a p r o b a
L 208.22 8 297.69 3 181.73 5 0.0577 Lowbackpain 100 18 100 17 100 19 1.000
a i g l a r u e N l a n i m e g i r T ) n i a p l a i c a f
( 203.23 9 197.22 6 169.73 6 0.3351
n o it o m e v it it e p e R s r e d r o s i
d 96.03 19 83.15 20 115.76 18 0.2331
n i a p y r u j n I -n r u
Th er e w er e im por t an t div er gen ces bet w een
st u d i ed sam p l es i n b o t h m et h o d s an d d i f f er en ces
b et w een p at ien t s an d p r of ession als ar e h ig h lig h t ed
( p at ien t s- p h y sician s, p at ien t s- n u r ses) . Th ese d at a
suggest t hat professionals and pat ient s have different
percept ions regarding t hese t ypes of pain. We observe
t h a t n u m e r i c a l v a l u e s i n b o t h m e t h o d s a r e
u n d e r e s t i m a t e d b y p r o f e s s i o n a l s . Co m p a r e d t o
p a t i e n t s, p r o f e ssi o n a l s a l m o st a l w a y s p r e se n t e d
sm aller v alu es.
We highlight t hat pain in AI DS present ed t he
h i g h est n u m b er o f d i v er g en ces b et w een sam p l es.
Th e r e w e r e d i f f e r e n c e s b e t w e e n p a t i e n t s a n d
physicians and pat ient s and nur ses in t he m agnit ude
est im at ion m et hod and differ ences bet w een pat ient s
and physicians, pat ient s and nurses and also bet ween
p h y si ci an s an d n u r ses i n t h e cat eg o r y est i m at i o n
m et h od .
Cancer pain was considered t he m ost int ense
pain in t he m aj orit y of t he st udied sam ples and in t he
differ ent psy chophy sical m et hods used. Cancer pain
is a f r equ en t sy m pt om in pat ien t s w it h can cer an d
present s significant int ensit y. This daily pain m anifest s
it self in m ore t han one place in t he body and, when it
is n ot con t in u ou s, it r em ain s f or sev er al h ou r s per
day. Pain occurs in pat ient s wit h cancer t hrough several
discom for t s, such as “ cut aneous lesions, unpleasant
o d o r s, a n o r ex i a , ca ch ex i a , l a ck o f sl eep , f a t i g u e,
an x iet y, depr ession , ex per ien ce of feelin g m u t ilat ed
a n d d i sf i g u r e d , a n t i ci p a t o r y m o u r n i n g , e co n o m i c
har dship, spir it ual dist r ess”( 9).
A st u dy( 1 0 ) com par ed t h e dif f er en t t y pes of
pain u sin g t h e Visu al An alogu e Scale ( VAS) for t h e
int ensit y of pain ( sensit ive dim ension) and for t he level
of discom f or t ( af f ect iv e dim en sion ) cau sed by su ch
st im uli. St udy part icipant s were: 87 pat ient s wit h low
back pain, 20 pat ient s wit h pain in shoulder and neck,
3 8 p a t i e n t s w i t h m y o f a sci a l t e m p o r o m a n d i b u l a r
disorder pain, 19 wit h causalgia, 17 wit h cancer pain
an d 2 3 in ch ildbir t h . Resu lt s r ev ealed t h at pat ien t s
wit h cancer pain and pat ient s wit h non- cancer chronic
p ain p r esen t ed h ig h r at es of p ain in t h e af f ect iv e
d i m en si o n ( l ev el o f d i sco m f o r t ) , w h i l e p at i en t s i n
ch i l d b i r t h a n d w i t h e x p e r i m e n t a l l y i n d u ce d p a i n
p r esen t ed l ow er r at es i n t h e sen si t i v e d i m en si on .
These findings suggest t hat t he per cept ion of pain is
r elat ed t o life- t hr eat ening pr ocesses, w hich incr eases
t h e e x p e r i e n ce o f p a i n w h e n co m p a r e d t o n o n
-t hr ea-t ening pr ocesses ( childbir -t h and ex per im en-t ally
in d u ced p ain ) . An ot h er ob ser v at ion r ef er s t o p ain
during childbirt h. Wom en who focused on t he birt h of
t h ei r ch i l d p r esen t ed l o w er r a t es i n t h e a f f ect i v e
dim ension t han t hose who sim ply focused on t he pain
it self. I t suggest s t hat t he int erpret at ion of t he process
cau sin g t h e pain in f lu en ces it s per cept ion an d t h at
t he ext ent t o w hich it represent s a t hreat t o life and
q u alit y of lif e in cr eases t h e af f ect iv e d im en sion of
clinical pain.
We highlight t hat m y ocar dial infar ct ion pain
is am on g t h e f iv e m ost in t en se p ain t y p es in t h is
st udy. How ever, none of t he st udied sam ples rat ed it
higher t han cancer pain. “ Som eone w ho ex per iences
a h ear t at t ack h as t h e sam e ch an ces o f d y i n g o f
anot her at t ack in t he shor t cour se as som eone w ho
has cancer of dy ing of cancer in t he shor t cour se”( 11).
This aut hor st r esses t hat m et aphor s link ed t o cancer
i m p l y p r o cesses l i n k ed t o a sen t en ce o f d eat h , a
“ c u r s e ” , a d i s e a s e c o n s i d e r e d a n “ i n v i n c i b l e
dest r u ct or ”( 1 1 ).
An in t er est in g com p ar ison b et w een can cer
and car diov ascular diseases cor r obor at es t he r esult s
of t his st udy: “ of all diseases, cancer is t he one t hat
causes t he st r ongest psy chological im pact . Not only
because of im m inent deat h, which is t he dest iny of all
o f u s, b u t b ecau se o f i t s p r o g r essi v e an d p ai n f u l
appr oxim at ion, w it h pot ent ial nat ur al or post - t her apy
m ut ilat ion. The risk of sudden deat h of cardiovascular
diseases is less scar ing. The per cept ion t hat cancer
is incur able, coupled w it h fear of it s pot ent ial r adical
t herapy and im ages of body alt erat ions caused by it s
t r eat m ent , is t er r ify ing”( 12).
Obser v ing Tables 1 and 2, one can per ceive
t hat , for t he out pat ient s’ group, pain in AI DS occupies
t he t hir d posit ion, bot h in t he m agnit ude est im at ion
and cat egor y est im at ion m et hods. I t is int er est ing t o
not ice t he out pat ient gr oup’s concer n w it h t his t y pe
of pain.
Pain in AI DS does not figur e am ong t he t en
m ost int ensiv e t y pes of pain in any of t he m et hods
used for t he phy sician gr oup and occupies t he nint h
place accor ding t o t he nur ses’ gr oup in t he cat egor y
e st i m a t i o n m e t h o d . Th i s t y p e o f p a i n p r e se n t e d
st at ist ically sign if ican t dif f er en ces bet w een pat ien t s
an d ph y sician s an d bet w een pat ien t s an d n u r ses in
t h e m a g n i t u d e e s t i m a t i o n m e t h o d . Th e r e w e r e
st a t i st i ca l l y si g n i f i ca n t d i f f e r e n ce s i n a l l sa m p l e s
( pat ient s- phy sicians; pat ient s- nur ses and phy
sicians-n u r ses) isicians-n t h e cat eg or y est im at iosicians-n m et h od . Th ese
f in din gs r ev eal div er gen ces bet w een t h e per cept ion
Gr eat er concer n w it h cancer pain t han pain
i n AI D S i s p er cei v ed . Th e i n d i v i d u a l w i t h ca n cer,
accor din g t o t h e st igm a cr eat ed f or su ch diseases,
“ does not deserve” such suffering and, t hus, is wort hy
of pit y and at t ent ion. I ndiv iduals w it h AI DS, on t he
ot her hand, ar e not w or t hy of such feelings because
of t heir “ behav ior s t hat could pot ent ially lead t o t he
d isease”.
A recent st udy( 13) found t hat 67% of a sam ple
r ep r esen t at i v e o f a p o p u l at i o n o f ad u l t s w i t h HI V
r epor t ed pain dur ing t he four w eek s pr ev ious t o t he
int erview. The aut hors st ress t hat t he pain relat ed t o
HI V is cau sed by dir ect ef f ect s of t h e v ir u s on t h e
ce n t r a l a n d p e r i p h e r a l n e r v o u s sy st e m , i m m u n e
s u p p r e s s i o n , t r e a t m e n t s a n d s e v e r a l d i s o r d e r s
associat ed t o t he v ir us pr esence.
Pain in AI DS has ot her im por t ant aspect s t o
be t ak en in t o accou n t , su ch as pr ej u dice r elat ed t o
t he sy ndr om e, disfigur em ent , self- est eem disor der s,
r ej ect ion of f am ily an d f r ien ds, r em ov al f r om w or k
and leisur e act iv it ies. Cancer pain and pain in AI DS
pr esent sim ilar aspect s.
However, t he social aspect of pain percept ion
sh ou ld b e k ep t in m in d . Based on t h e an aly sis of
r esu l t s f o u n d i n t h e st u d y, w e can i n f er t h at t h e
m eaning of t his painful phenom enon is also influenced
by t he societ y it self, t hat is, it is affect ed by t he st igm a
cr eat ed for t he disease t hat causes it .
Labor pain also occupies t he t hir d and fift h
p osit ion s w h en con sid er in g p h y sician s an d n u r ses,
r espect iv ely. For t h e ou t pat ien t s’ gr ou p, it occu pies
t he eight h posit ion. An ant hr opological st udy, car r ied
out t hrough t he et hnographic m et hod wit h part icipant
obser v at ion and sem i- st r uct ur ed int er v iew , aim ed t o
exam ine childbirt h at a public m at ernit y of a Brazilian
capit al, focusing on t he per spect ive of young w om en
and adolescent s. Result s revealed t hat w om en report
t hat labor is dom inat ed by fear, loneliness and pain.
“ By t he w ay, it confir m s st or ies t hese w om en hear d
abou t labor pain ou t of t h e h ospit al, w h et h er f r om
r elat ives and fr iends, or t he m edia in general”. They
st r ess t he absence of a com panion dur in g labor for
inst it ut ional r easons, w hich w ould pr oduce a gr eat er
sen se o f secu r i t y an d b et t er co p i n g . Th e au t h o r s
consider t hat cult ur al m eanings ar e insepar able fr om
phy sical sensat ions( 14).
The st udy m ent ioned abov e can help in t he
d iscu ssion of t h e r esu lt s ap p oin t ed h er e. Alt h ou g h
labor pain is relat ed t o childbirt h and not t o a disease
or life- t hr eat ening pr ocess, it w as consider ed one of
t he m ost int ense pain t ypes. We have t o bear in m ind
t hat t he approach of t he childbirt h process in Brazil is
pr ecar ious and generat es feelings of fear, loneliness
and abandonm ent , which lead t o higher t ension levels
and increased painful percept ion. Anot her observat ion
is t hat pain consider ed of low er int ensit y, like t hose
caused by r epet it ive m ot ion disor der s, j oint pain and
low back pain, are t ypes of pain wit h high prevalence
in t h e popu lat ion , w it h h igh f r equ en cy in daily lif e,
and cause physical and social incapacit y( 15- 17). However,
t hey are not life t hreat ening and are relat ed t o work,
gender, age, st r ess, sedent ar iness, am ong ot her s.
Kendall’s coefficient of concordance ( Kendall’s
W ) w a s co m p u t e d f o r b o t h sca l e s i n t h i s st u d y.
Ken dall’s coefficien t r an ges bet w een - 1 an d 1 , w it h
n egat iv e v alu es in dicat in g an in v er sely pr opor t ion al
relat ion bet ween variables, t hat is, as t he values of a
v a r i a b l e i n cr ea se, t h e v a l u es o f a n o t h er v a r i a b l e
d e c r e a s e . Po s i t i v e v a l u e s i n d i c a t e a d i r e c t l y
p r op or t ion al r elat ion b et w een v ar iab les, t h at is, as
t he values of a variable increase t he values of anot her
var iable also incr ease. Values close t o zer o, negat iv e
or posit ive, indicat e independence bet w een variables,
t hat is, t he behavior of a variable does not influence
t he ot her.
Ken dall’s coef f icien t of con cor dan ce applied
t o t h e est im at es, com p ar in g t h e d if f er en t m et h od s
( m agn it u de est im at ion an d cat egor y est im at ion ) for
t he different t ypes of pain, result ed in W= 0.68 for t he
ou t p at ien t g r ou p f r om d if f er en t ou t p at ien t s clin ics,
W= 0.89 for t he physicians, and W= 0.78 for t he nurses.
I t indicat es t hat t he r ank of pain int ensit y obt ained
f r om t h e est im at ion of t h e t w o m et h od s p r esen t s
concor dance for t he t hr ee gr oups and also t hat t he
est im at es ar e st at ist ically significant , p< 0. 001.
Ther e ar e som e essent ial differ ences in t he
obt ained scales. I t is possible t o est ablish t he r ank ,
t he differ ences and especially t he r at ios bet w een t he
degrees of pain int ensit y in t he m agnit ude est im at ion
m et hod. I n t he cat egor y est im at ion m et hod, on t he
ot her hand, it is only possible t o est ablish t he r ank
and differ ences bet w een pain int ensit ies. I n t he r ank
est im at ion m et hod, only t he r ank of pain int ensit ies
can be obt ained.
Au t h or s of a p r ev iou s st u d y( 1 8 ) st r ess t h at
t here are t wo m ain problem s wit h t he use of cat egory
scales. Fir st , because t he num ber of cat egor ies w it h
which st im uli are j udged is fixed t he m et hod int roduces
som e biases. This is t he r eason w hy cat egor y scales
am plit ude of cat egor ies and fr equency of st im uli. I n
t he case of pain m easurem ent , a large source of error
is t h e em bar r assm en t cau sed t o t h e par t icipan t by
t h e im p osit ion of an u p p er lim it at t h e en d of t h e
con t in u u m of p ain , t h at is, at t h e en d of t h e p ain
m easur em ent scale. Second, cat egor y scales do not
perm it st at em ent s regarding difference rat ios bet ween
t h e obt ain ed m easu r es. I t is possible t o say t h at a
m easure is larger t han t he ot her or subt ract one from
t he ot her, but it is not possible t o infer t o what ext ent
one m easur e is lar ger or sm aller t han t he ot her.
I n t he cat egor y est im at ion m et hod, it is not
possible t o k now t he r at ios bet w een pain int ensit ies,
t hat is, one cannot t ell t o what ext ent cancer pain is
considered m ore or less int ense t han burn- inj ury pain.
We can say, by observing Table 2, t hat m enst rual colic
( ME= 317. 31) is consider ed by t he phy sicians’ gr oup
a b o u t t w i ce m o r e i n t en se t h a n p r eo p er a t i v e p a i n
( ME= 1 5 9 . 8 3 ) ; w h ile t h e n u r ses’ g r ou p con sid er ed
cancer pain ( ME= 310.50) t wice m ore int ense t hat pain
in per ipher al neur opat hy ( ME= 154. 24) .
Th ese com par ison s can also be car r ied ou t
bet w een t h e gr ou ps. For ex am ple, w e can st at e t h at
p a i n i n AI D S i s co n si d er ed t w o a n d a h a l f t i m es
m or e in t en se by t h e ou t pat ien t s’ gr ou p ( ME= 3 0 3 . 6 0 )
t h a n b y t h e p h y si ci a n s’ g r o u p ( ME= 1 1 8 . 4 2 ) , a n d
t w i ce m o r e i n t e n se t h a n t h a t co n si d e r e d b y t h e
nur ses’ gr oup ( ME= 1 3 3 . 1 1 ) . I t also pr esen t s sim ilar
i n t e n s i t y b e t w e e n n u r s e s ( M E= 1 3 3 . 1 1 ) a n d
ph y sician s ( ME= 1 1 8 . 4 2 ) . Sev er al ot h er com par ison s
b e t w e e n s a m p l e s a n d w i t h i n s a m p l e s c a n b e
per for m ed, since t he r at io scale allow s for t his k ind
o f co m p ar i so n .
CONCLUSI ONS
- Cancer pain, m yocardial infarct ion pain, renal colic,
bur n- inj ur y pain and labor pain w er e consider ed t he
m ost int ense t ypes of pain, regardless of t he m et hod
used or sam ple st udied, in addit ion t o pain in AI DS,
considered by t he out pat ient s’ group one of t he m ost
int ense pain t y pes.
- Pain in t em porom andibular j oint disorder, j oint pain,
r epet it iv e m ot ion disor der pain, m enst r ual colic and
low back pain were considered t he least int ense t ypes,
r egar dless of t he m et hod used or sam ple st udied.
- Ran k in g of in t en sit ies f or dif f er en t t y pes of pain ,
com paring t he different psychophysical m et hods used,
r esult ed in a significant lev el of concor dance.
- Th i s st u d y p er m i t t e d d ee p er r ef l e ct i o n s o n t h e
percept ion of t he painful phenom enon and it s m eaning
in our cult ur e, com par ing pr ofessionals and pat ient s
t h r o u g h a v a l i d a n d r el i a b l e m et h o d . Th er e w er e
div er gences in t he per cept ion of int ensit ies of som e
t y p e s o f p a i n , m a i n l y b e t w e e n p r o f e ssi o n a l s a n d
pat ien t s ( ph y sician s- pat ien t s, n u r ses- pat ien t s) .
- A pr ofile of per cept ion of differ ent t y pes of pain in
our societ y was est ablished. The dat a collect ed raised
o r i g i n a l c h a r a c t e r i s t i c s f o r t h i s s t u d y. S u c h
char act er ist ics ar e show n t hr ough t he com par ison of
differ ent t y pes of pain j udged by differ ent sam ples.
REFERENCES
1 . Car v alh o AMP. En f r en t am en t o d a d or : con t r ib u ições d a p sicolog ia. Rev. Dor : Pesq u isa, Clín ica e Ter ap êu t ica 2 0 0 5 j an / fev / m ar ; 6 ( 1 ) : 5 2 5 - 9 .
2. Engel GL. Psychogenic pain and t he painprone pat ient . Am J Med 1 9 5 9 ; 2 6 ( 6 ) : 8 9 9 - 9 1 8 .
3. Noble B, Clark D, Meldrum M, Have H, Seym our J, Winslow M, Paz S. The m easurem ent of pain, 1945- 2000. J Pain Sym pt Man ag . 2 0 0 5 Jan u ar y ; 2 9 ( 1 ) : 1 4 - 2 1 .
4. Girdler SS, Maixner W, Naft el HA, St ewart PW, Moret z RL, Ligh t KC. Cigar et t e sm ok in g, st r ess- in du ced an algesia an d p a i n p e r c e p t i o n i n m e n a n d w o m e n . Pa i n 2 0 0 5 A p r i l ; 1 1 4 ( 3 ) : 3 7 2 - 8 5 .
5. Cam pbell CM, Edw ards RR, Fillingim RB. Et hnic differences in responses t o m ult iple experim ent al pain st im uli. Pain 2005 Jan u ar y ; 1 1 3 ( 1 - 2 ) : 2 0 - 6 .
6- St ev ens SS. On t he psy chopy sical law . Psy chol Rev 1957 May ; 6 4 ( 3 ) : 1 5 3 - 8 1 .
7 . Per eira LV, Sousa FAEF. Psy chophy sical evaluat ion of t he
d escr i p t o r s o f p a i n i n t h e p o st o p er a t i v e. Rev La t i n o - a m En f er m ag em 2 0 0 7 ; 1 5 ( 3 ) : 4 7 4 - 9 .
8 . Fal ei r o s So u sa FAE, Ho r t en se, P. So ci al p er cep t i o n o f nursing professional assessed by different scales. Rev Lat ino-am En f er m ag em 2 0 0 6 ; 1 4 ( 6 ) : 8 5 7 - 6 2 .
9. Pim ent a CAM, Fer r eira K. Dor no doent e com câncer. I n: Pim ent a CAM, Mot a DDCF, Cr uz DALM, or ganizador es. Dor e cu i d ad o s p al i at i v o s: En f er m ag em , m ed i ci n a e p si co l o g i a. Bar uer i, SP: Manole; 2 0 0 6 . p. 1 2 4 - 6 6 .
1 0 . Pr i c e D D , H a r k i n s S W, B a k e r C. S e n s o r y - a f f e c t i v e r e l a t i o n s h i p s a m o n g d i f f e r e n t t y p e s o f c l i n i c a l a n d ex per im en t al pain . Pain 1 9 8 7 Mar ch ; 2 8 ( 3 ) : 2 9 7 - 3 0 7 . 11. Sont ag S. Doença com o m et áfora. Rio de Janeiro: Graal; 1 9 8 4 .
14. Mccallum C, Reis AP. Re- significando a dor e super ando a so l i d ã o : e x p e r i ê n ci a s d o p a r t o e n t r e a d o l e sce n t e s d e classes populares at endidas em um a m at ernidade pública de Sal v ad o r, Bah i a, Br asi l . Cad . Saú d e Pú b l i ca 2 0 0 6 j u n h o ; 2 2 ( 7 ) : 1 4 8 3 - 9 1 .
1 5 . Saast am oin em P, Lein o- Ar j as P, Laak son en M, Lah elm a E. Socio- econ om ic d if f er en ces in t h e p r ev alen ce of acu t e, chr onic and disabling chronic pain am ong ageing em ployees. Pai n 2 0 0 5 Ap r i l ; 1 1 4 ( 3 ) : 3 6 4 - 7 1 .
1 6 . Alex an d r e GC, Nad an ov sk y P, Lop es CS, Faer st ein E.
Prevalência e fat ores associados à ocorrência da dor de dent e q u e i m p e d i u a r e a l i za çã o d e t a r e f a s h a b i t u a i s e m u m a população de funcionár ios públicos no Rio de Janeir o, Br asil. Cad. Saú de Pú blica 2 0 0 6 m aio; 2 2 ( 5 ) : 1 0 7 3 - 8 .
17. Chung JWY, Wong TKS. Prevalence of pain in a com m unit y popu lat ion . Pain Med 2 0 0 7 Jan u ar y ; 8 ( 3 ) : 2 3 5 - 4 2 .
18. Sousa FAEF, Da Silva JA. A m ét r ica da dor ( dor m et r ia) : p r o b l em as t eó r i co s e m et o d o l ó g i co s. Rev D o r : Pesq u i sa, Clín ica e Ter apêu t ica 2 0 0 5 j an / f ev / m ar ; 6 ( 1 ) : 4 6 9 - 5 1 3 .