INTRODUCTION
The immediat e implant placement af t er t oot h ext ract ion has been report ed t o be as predict able as placing implant s int o healed sit es (1); but wit h advant ages such as reduced number of surgical procedures (2- 8), reduct ion of t he overall t reat ment t ime and also a possible preservat ion of t he morphological cont our of t he ridges (3, 6). However, in regard t o t his last considerat ion, some st udies in animals have shown cont radict ory result s, describing pronounced resorpt ion of t he buccal, and t o some ext ent , t he lingual bone plat es af t er implant placement in f resh ext ract ion socket s (9, 10). Novaes Jr. (11) showed t hat t he morphological and vascular charact erist ics of t he bone crest s may have an import ant impact on t he bone remodeling process t hat occurs immediat ely af t er implant at ion. Through a hist ological analysis of specimens sect ioned in buccal- lingual direct ion, t hey observed t hat t he widt h of bot h bone plat es increased f rom t he coronal t hird t o t he most apical t hird, being t he buccal plat es always signif icant ly t hinner when compared t o t he lingual bone plat es. M ore specif ically, t hey described t he coronal port ion of t he buccal bone plat e as ext remely delicat e, w hich is in agreement w it h previous observat ions (10, 12), and t his charact erist ic may explain almost in part why t he buccal bone plat es are more easily resorbed. They showed some slides where t he buccal bone plat es appeared wit hout or wit h very f ew marrow spaces. In f act , t he buccal bone plat es w ere const it ut ed, in a st at ist ically signif icant way, by a higher cort ical bone when compared t o t he lingual bone plat es, in f irst and second coronal t hirds; t his bone densit y analysis was obt ained by t he subt ract ion of t he bone marrow area f rom t he t ot al bone area. Int erest ingly, t hey also evidenced in some hist ological observat ions, marrow
ARTHUR BELÉM NOVAES JR.
1, RAQUEL REZENDE MARTINS DE BARROS
2, VULA PAPALEXIOU
3,
ADRIANA LUISA GONÇALVES DE ALMEIDA
4>
1
Professor and Chairman of Periodontology, Department of Oral Surgery and Periodontology, School of Dentistry of Ribeirão Preto of the University of
São Paulo, SP, Brazil
2
Post-doctoral student, Department of Oral Surgery and Periodontology, School of Dentistry of Ribeirão Preto of the University of São Paulo, SP, Brazil
3Professor of Periodontology, Center of Biologic and Health Science, School of Dentistry, Catholic Pontifical University, PR, Brazil.
4Graduated in Biology and Microscopic and Image Analysis Laboratory Technician of the Department of Oral Surgery and Periodontology, School of
Dentistry of Ribeirão Preto of the University of São Paulo, SP, Brazil
Buccal bone loss after immediate implantation
can be reduced by the flapless approach
KEY WORDS
Animal model; Bone resorption; Flapless surgery;
Immediate implants.
ABSTRACT
Aim
The aim of this study was to evaluate the buccal bone
remodeling after immediate implantation with flap or flapless
approach.
Material and Methods The mandibular bilateral premolars of 3
dogs were extracted and immediately three implants were placed
in both hemi-arches of each dog. Randomly, one hemi-arch was
treated with the flapless approach, while in the contra lateral
hemi-arch tooth extractions and implant placement were done
after mucoperiosteal flap elevation. Non-submerged healing of 12
weeks was provided for both groups. Histomorphometric analysis
was done to compare buccal and lingual bone height loss, bone
density and bone-to-implant contact in the groups. Fluorescence
analysis was performed to investigate the dynamic of bone
remodeling in the different groups.
Results
There was a significant association between the surgical
flap and the extent of bone resorption around immediate
implants. The loss of buccal bone height was significantly lower in
the flapless group when compared to the flap group (0.98 mm x
2.14 mm, respectively, p<0.05). The coronal and apical buccal
bone densities of the flap group were significantly higher when
compared to the lingual components, showing anatomical
differences between the bone plates. Fluorescence analysis
showed no major differences in bone healing between the flap
and flapless groups, supporting that the higher loss of buccal bone
height is linked to the anatomic characteristics of this plate and to
the negative influence of the detachment of the periosteum in
immediate implant therapy.
spaces in direct cont act t o t he periost eum in t he buccal bone plat e, sust aining t he hypot hesis t hat one of t he main f unct ions of t he periost eum and periodont al ligament blood vessels is t o supply nut rient s and cells t o t he alveolar bone (13).
Convent ionally, immediat e implant at ion surgeries give emphasis t o some import ant precaut ions such as less t raumat ic t oot h ext ract ion and implant primary st abilit y, and are usually done wit h sulcular incisions and mucoperiost eal f lap elevat ion. However, it is known t hat t he displacement of t he periost eum and alveolar bone denudement result in an acut e inf lammat ory response and consequent ly in bone resorpt ion (14- 16). Ost eoclast s were observed on surgical exposed alveolar bone areas during t he f irst t wo weeks of wound healing (17). Besides, a relevant inf ormat ion t o consider is t hat , alt hough a pronounced loss of t he buccal bone w all w ere f requent ly described af t er mucoperiost eal surgeries applied in periodont al t reat ment of dent at e areas, t he same was not observed on t he t hicker lingual wall (16, 18, 19).
Kim et al. (20) compared t he vascularit y of peri-implant mucosa bet ween f lap and f lapless peri-implant surgeries in a dog model and showed t hat t he sof t t issue around implant s in f lapless sit es appeared t o be f ree f rom signs of inf lammat ion, while approximat ely half of t he implant s in t he f lap sit es exhibit ed a surrounding edemat ous t issue t hat bled when gent ly probed. Addit ionally, t he number of vessels observed was 51.4 ± 9.2 in t he f lapless group and 38.2 ± 8.1 in t he f lap group, and t his dif f erence was st at ist ically signif icant . Based on t hese f indings, t hey suggest ed t hat t he more richly vascularized peri- implant mucosa provided by t he f lapless procedure is direct ly relat ed t o an increased blood supply around t he implant , which may st rengt hen t he resist ance t o inf lammat ion.
The purpose of t he present st udy was t o evaluat e if t he f lapless approach can int erf ere in t he buccal bone remodeling af t er immediat e implant at ion in mongrel dogs, analyzing t he hist omorphomet ric paramet ers of bone height loss, bone densit y and bone- t o- implant cont act af t er 12 weeks of healing and also t he dynamic of bone remodeling in f our dif f erent t imes along t his period t hrough f luorescence analysis.
M ATERIALS AND M ETHODS
Surgical procedure
The st udy prot ocol was approved by t he Inst it ut ion’s Animal Research Commit t ee of t he School of Dent ist ry of Ribeirão Pret o- Universit y of São Paulo and was perf ormed in t hree young adult male mongrel dogs t hat weighed approximat ely 16 kg. The
animals present ed int act maxillas, no general occlusal t rauma, and no oral viral or f ungal lesions and were in good general healt h, wit h no syst emic involvement as det ermined by a vet erinarian f ollowing clinical examinat ion.
Food was wit hheld in t he night preceding surgeries. The animals w ere pre- anaest het ized w it h acepromazine 0,2% - 0,05 mg/kg IM . Af t er t hat an int ravenous cat het er was placed in t he f oreleg f or induct ion wit h t hiopent al 2,5% - 5 a 8 mg/Kg IV. Animals were t hen moved t o t he operat ing room and maint ained on gas anest hesia (1–2% isof lurane/O2 t o ef f ect ). Convent ional dent al inf ilt rat ion anest hesia was used at t he surgical sit es. The animals received a slow const ant rat e inf usion of lact at ed Ringer’s solut ion (10–20 ml/kg/h IV) t o maint ain hydrat ion during surgery. These procedures were made and accompanied by a vet erinarian.
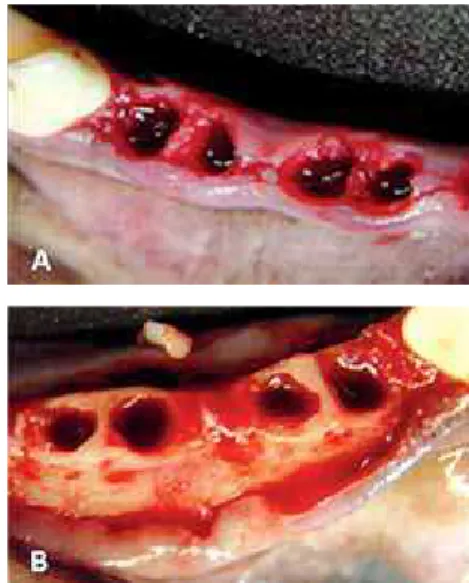
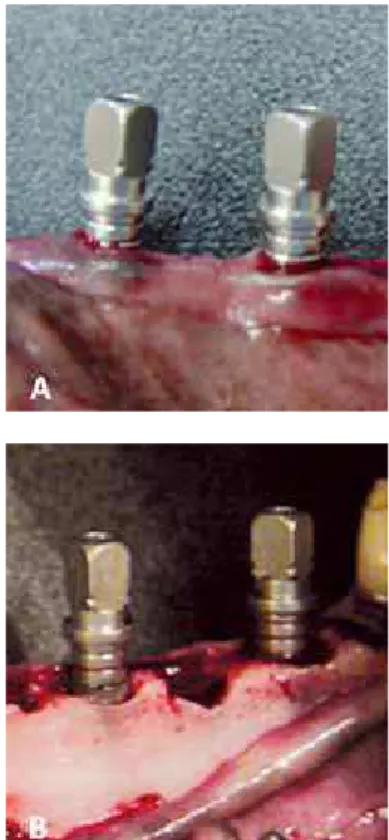
The surgical procedures f or t he mandibular premolar ext ract ions were done in each hemi- arch of each dog. Randomly, one of t he sides was t reat ed wit h t he f lapless approach (experiment al group) (f ig. 1A), w hile t he cont ralat eral side w as t reat ed w it h mucoperiost eal f laps (f ig. 1B). The t eet h were sect ioned in a bucco- lingual direct ion at t he bif urcat ion so t hat t he root s could be individually ext ract ed, wit hout damaging t he bony walls, using a periot ome. Af t er alveolar debridement , t hree Ankylos implant s measuring 3.3 x 9.5 mm (diamet er and lengt h, respect ively) were immediat ely insert ed in t he mesial socket of t he correspondent t hree pre- molars in bot h hemi- arches of each dog, t ot aling 18 implant s in t he experiment . The implant s were placed at t he level of bone crest and a gap of 1mm f rom t he buccal cort ical wall t o t he implant was always lef t (f ig. 2) wit hout invading t he lingual bone plat e wit h
t he drill or t he implant . Subsequent ly, healing caps of 1.5 mm of height were adjust ed in order t o provide a non- submerged healing in bot h groups. The f laps of t he cont rol group were reposit ioned and sut ured wit h absorbable sut ures (Vicryl, Et hicon, Inc., Johnson & Johnson Company, São José dos Campos- SP, Brasil), while t he sof t t issues were accommodat ed and t hen sut ured in t he experiment al group. No graf t ing mat erials were used in t he gaps bet ween t he buccal plat es and t he implant s.
The animals received painkillers and ant i-inf lammat ory agent s. A broad spect rum ant ibiot ic (penicillin and st rept omycin 20,000 IU; 1.0 g/10 kg IM ) was administ ered immediat ely post - surgery and re- dosed af t er 4 days. The animals were maint ained on a sof t diet f or 14 days when t he sut ures were removed. The healing was evaluat ed weekly and plaque cont rol was maint ained by f lushing t he oral cavit y wit h chlorhexidine gluconat e. The remained t eet h were cleaned mont hly wit h ult rasonic point s and all implant s remained non- submerged during t he experiment al period.
During t he healing period f luorescence bone markers were administ ered (21) t o observe t he dynamics of bone f ormat ion. One week af t er implant placement ,
calcein green (75 mg /Kg body w eight - Sigma Chemical Co., St Louis, M O, USA) was int ravenously administ ered; at t he second week, it was administ ered 300 mg of red alizarin S/Kg body weight (Sigma); af t er 4 w eeks it w as administ ered 150 mg oxyt et racyclin HCl/Kg body weight (Sigma); and f inally af t er 12 weeks 75 mg calcein blue/Kg body weight (Sigma) were also administ ered. All dyes were prepared immediat ely bef ore use wit h 2% sodium bicarbonat e or saline. Af t er preparat ion, pH was adjust ed t o 7.4 and t he solut ion was f ilt ered t hrough a 0.45 Ìm f ilt er (Schleider & Schuell GmbH, Dassel, Germany). Each dog received a t ot al dose of 3 ml.
Hist ological processing
The animals were sedat ed and t hen sacrif iced wit h an overdose of t hiopent al t welve weeks af t er implant placement . The hemi- mandibles w ere removed, dissect ed and f ixed in 4% phosphat e- buf f ered f ormalin pH 7, f or 10 days, and t ransf erred t o a solut ion of 70% et hanol unt il processing. The specimens w ere dehydrat ed in increasing concent rat ions of alcohol up t o 100%, inf ilt rat ed and embedded in LR Whit e resin (London Resin Company, Berkshire, England), and hard- sect ioned in bucco-lingual direct ion using t he t echnique described by Donat h & Breuner (22). The most cent ral sect ions were st ained wit h St evenel’s blue and Alizarin red S f or hist omet ric analysis using opt ic microscopy.
Hist omorphomet ric analysis
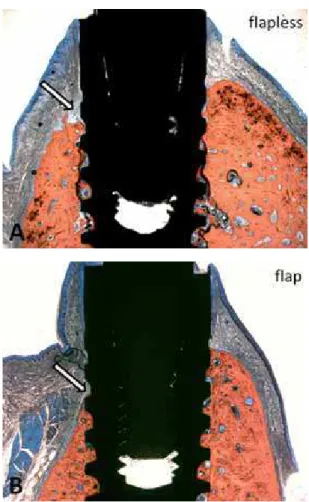
Longit udinal buccal- lingual hist ological sect ions f rom each implant were capt ured t hrough a video camera Leica DC 300F (Leica M icrosyst ems GmbH, Nussloch, Germany) joined t o a st ereomicroscope Leica M ZFL III (Leica M icrosyst ems GmbH, Nussloch, Germany). The images were analyzed t hrough t he Image J program (Nat ional Inst it ut es of Healt h, Bet hesda,USA). The buccal bone wall resorpt ion was det ermined in relat ion t o t he lingual bone wall as a linear measurement (relat ive measurement ) (Fig. 3, 4). A horizont al imaginary line was drawn in order t o evidence t he height of t he lingual bone plat e, and t hen t he measurement of t he buccal bone wall resorpt ion was obt ained vert ically f rom t hat line t o t he peak of t he buccal bone plat e. The buccal and lingual bone plat es were also measured f rom t he shoulder of t he implant t o t he f irst bone- t o- implant cont act (absolut e measurement ). The percent ages of bone- t o- implant cont act (BIC) w ere calculat ed t hroughout t he implant perimet er, f rom t he f irst coronal bone- t o- implant cont act , considering t he mineralized bone in direct cont act wit h t he implant surf ace. The bone densit y was det ermined wit hin t wo rect angles, one of t hem adjacent t o t he implant surf ace (BDA), and t he ot her as mirror image of t he f irst , but dist ant t o t he implant surf ace (BDD). This
Fig. 2
The implants were immediately inserted in the mesial alveolus of
an excit at ion level bet ween 450- 490 nm, N2- 1 f or red alizarin S t hat has an excit at ion level bet ween 515- 560 nm, D f or oxyt et racyclin HCl t hat has an excit at ion level bet ween 355- 425 nm and A f or calcein blue t hat has an excit at ion level bet ween 340- 380 nm. All t he images were adjust ed and analyzed t hrough t he Image J program (Nat ional Inst it ut es of Healt h, Bet hesda, USA) t o det ermine t he percent ages of bone marked.
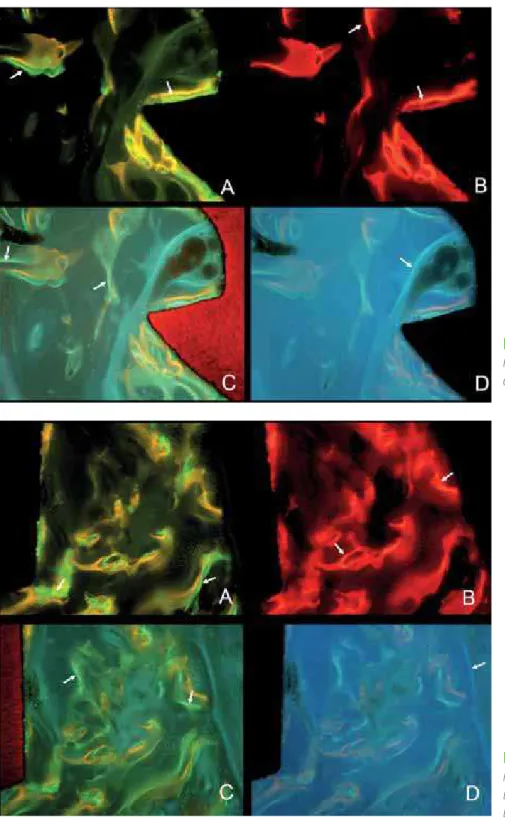
The bone marked was det ermined in t wo dif f erent posit ions along t he implant s, at coronal and apical levels in bot h buccal and lingual sides, using t he same pre- det ermined rect angle f or all t he specimens (f ig. 5, 6). The quant it y of bone marked represent ed t he percent ages of f luorescent bone in relat ion t o t he t ot al area. A single examiner, wit h no knowledge of t he experiment al groups made t he measurement s. analysis was done in t wo dif f erent posit ions of t he
implant s, one coronal and ot her apical, permit t ing an int ra- group evaluat ion. The bone densit y measurement s evaluat ed t he percent ages of mineralized bone in relat ion t o t he percent ages of marrow cavit ies. A single examiner, w it h no knowledge of t he experiment al groups made t he measurement s.
Fluorescence analysis
Fluorescence microscopic images were longit udinally capt ured f rom each implant t hrough a video camera Leica DC 300F (Leica M icrosyst ems GmbH, Nussloch, Germany) joined t o a st ereomicroscope Leica M ZFL III (Leica M icrosyst ems GmbH, Nussloch, Germany), using appropriat ed barrier f ilt ers. The f ilt ers of wavelengt hs used was I3 f or calcein green t hat has
Fig. 4
As in Figure 3, in (A) there is a representative image of
the flapless group, while in (B) a representative image of the flap
group. Note again the difference of vertical bone loss between
them. In these images is more evident the higher bone density
found in the buccal bone plates (on the left) when compared to
the lingual bone plates (on the right), which is easily seen by the
different number and dimension of marrow spaces found in
them.
Stevenel’s blue and Alizarin red S stain; magnification x 10.
St at ist ical analysis
M ean values and st andard deviat ions w ere calculat ed. The dat a were grouped using t he dogs as unit s f or analysis. The mean dif f erences bet ween t he groups f or each hist omorphomet ric paramet er were analyzed t hrough t he M ann- Whit ney nonparamet ric t est wit h a conf idence level of 95%. Besides f or t he f luorescence analysis, all measurement s w ere st at ist ically evaluat ed using t he non- paramet ric analysis of variance, Kruskal- Wallis, and Dunn t est
w as used f or mult iple comparisons among t he means. The conf idence level was 95%.
RESULTS
Clinical and hist ological observat ions
Healing was unevent f ul f or all animals and no implant w as lost . All implant s became osseoint egrat ed af t er t he 12- week post operat ive
Fig. 5
Different bone markers at the coronal
level of the implant. A: calcein green; B: red
alizarin; C: oxytetracyclin; D: calcein blue
period. The marginal gaps bet ween t he buccal walls and t he implant s disappeared wit hout t he migrat ion of connect ive t issue in bot h groups.
Hist omorphomet ric analysis
The loss of buccal bone height was st at ist ically lower in t he f lapless group when compared t o t he f lap group (0.98 ± 0.45 mm x 2.14 ± 0.34 mm) (p< 0.0001). Addit ionally t he comparisons of t he absolut e values of bone loss around t he implant s f or t he f lapless and f lap groups show ed st at ist ically signif icant dif f erences bet ween t he buccal bone resorpt ion of t he experiment al groups (2.46 ± 0.42 mm x 3.83 ± 0.21 mm, f lapless and f lap, respect ively) (p< 0.0001), but not bet ween t he lingual remaining bone height s (1.48 ± 0.27 mm x 1.70 ± 0.31 mm, f lapless and f lap, respect ively). The comparisons wit hin t he groups showed st at ist ically signif icant dif f erences bet ween t he buccal and lingual bone resorpt ion in t he f lapless (2.46 ± 0.42 mm x 1.48 ± 0.27 mm, buccal and lingual, respect ively) (p< 0.0001) and f lap groups (3.83 ± 0.21 mm x 1.70 ± 0.31 mm, buccal and
lingual, respect ively) (p< 0.0001). The loss of t he buccal bone in t he f lap group was more t han 100% great er t han t he lingual bone.
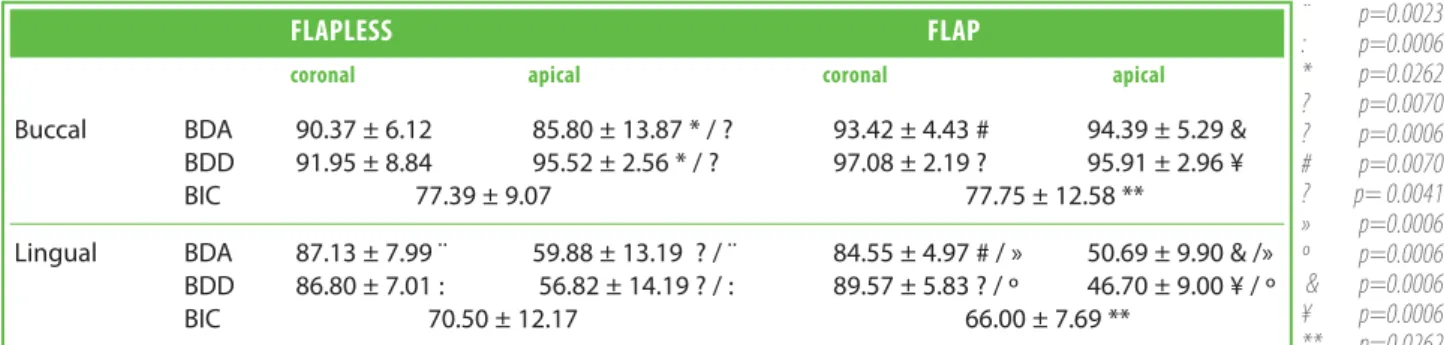
The buccal bone densit y was numerically higher in all t he paramet ers evaluat ed when compared t o t he lingual bone densit y (Fig. 3. 4). These dif f erences were st at ist ically signif icant f or all t he comparisons t est ed, except f or t he f lapless coronal buccal bone densit y (t able 1).
Alt hough t he buccal bone densit y was numerically higher f or t he f lap group compared t o t he f lapless group, t hese dif f erences w ere not st at ist ically signif icant f or bot h coronal and apical paramet ers (t able 1).
The comparisons bet ween coronal and apical bone densit y were st at ist ically signif icant only f or t he lingual bone f or bot h f lapless and f lap groups, wit h t he apical bone having a lower densit y (t able 1). There were no st at ist ically signif icant dif f erences bet ween adjacent and dist ant bone densit ies f or all t he possible comparisons (t able 1).
All t he implant s present ed considerable good
Table 1
Percentages of bone density adjacent (BDA) and distant (BDD) and bone-to-implant contact (BIC) described as mean ± SD.
¨ p=0.0023 : p=0.0006 * p=0.0262 ? p=0.0070 ? p=0.0006 # p=0.0070 ? p= 0.0041 » p=0.0006 º p=0.0006
& p=0.0006 ¥ p=0.0006 ** p=0.0262
FLAPLESS
FLAP
coronal apical coronal apical
Buccal BDA 90.37 ± 6.12 85.80 ± 13.87 * / ? 93.42 ± 4.43 # 94.39 ± 5.29 & BDD 91.95 ± 8.84 95.52 ± 2.56 * / ? 97.08 ± 2.19 ? 95.91 ± 2.96 ¥
BIC 77.39 ± 9.07 77.75 ± 12.58 **
Lingual BDA 87.13 ± 7.99 ¨ 59.88 ± 13.19 ? / ¨ 84.55 ± 4.97 # / » 50.69 ± 9.90 & /» BDD 86.80 ± 7.01 : 56.82 ± 14.19 ? / : 89.57 ± 5.83 ? / º 46.70 ± 9.00 ¥ / º
BIC 70.50 ± 12.17 66.00 ± 7.69 **
Table 2
Fluorescence analysis. Comparisons between flapless and flap groups considering the percentage of each bone marker
administered during different time periods of bone healing.
BUCCAL
LINGUAL
coronal apical coronal apical
Calcein green flap 0 8.66 5.41 6.6
flapless 1.76 9.83 9.02 6.54
p value p>0.05 p>0.05 p>0.05 p>0.05
Alizarin red flap 1.05 21.1 21.71 15.83
flapless 9.83 26.07 13.36 12.76
p value p>0.05 p>0.05 p>0.05 p>0.05
Oxytetracyclin flap 0 5.71 3.62 2.16
flapless 1.26 5.31 4.36 1.5
p value p>0.05 p>0.05 p>0.05 p>0.05
Calcein blue flap 0 2.4 1.12 2.27
flapless 1.49 2.89 1.79 1.45
indicat ions of bone t o implant cont act and t he result s were remarkably similar bet ween t he groups. The buccal BIC in bot h groups is numerically higher when compared t o t he lingual BIC result s, and st at ist ically signif icant in t he f lap group (t able 1). The analysis under f luorescent microscopy showed bone remodeling in t he groups evaluat ed. The old bone always appeared darker and wit hout labeling. Calcein green appeared in very well delineat ed green bands (f ig. 5, 6A) as did in red t he alizarin red marker, which in some specimens also showed a smeared dif f use pat t ern (f ig. 5, 6B); oxyt et racyclin showed t hin yellow- green lines (f ig. 5, 6C) and f inally calcein blue was charact erized by a sof t blue color in a very dif f use pat t ern (f ig. 5 and 6D). In many specimens t he secondary ost eons were demonst rat ed by t he deposit ion of t he labels in a concent ric arrangement . The bone marker quant if icat ions sequent ially represent ed t he healing pat t ern of each dif f erent group. The percent ages of newly f ormed bone in t he dif f erent part s are described in t ables 2, 3 and 4. Table 2 represent s t he analysis bet ween t he f lap and
f lapless groups considering t he dif f erent part s, while t ables 3 and 4 show t he result s of t he int ra- group analysis, separat ely.
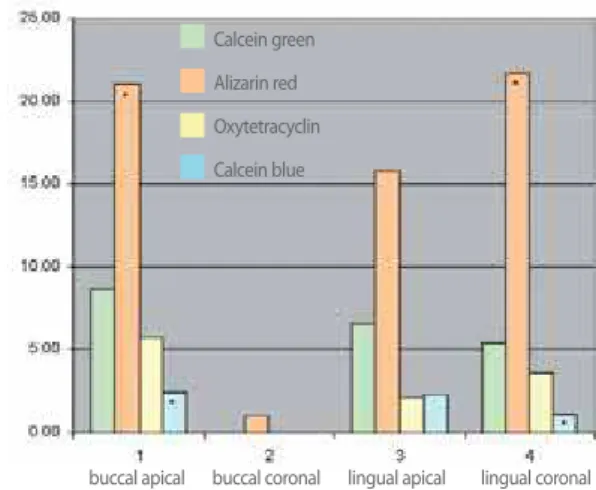
A pat t ern of bone remodeling bet w een t he experiment al groups (f lap and f lapless) and also bet ween t he dif f erent evaluat ed areas (buccal and lingual; apical and coronal) was det ect ed (f ig. 7, 8; t ables 3, 4). No st at ist ically signif icant dif f erences were f ound bet ween t he f lap and f lapless groups (t able 2), however numerically dif f erent values of bone f ormat ion were observed at t he buccal coronal area of t he groups, especially at t he red alizarin period of applicat ion. Generally, t he init ial phases of bone remodeling t hat w ere represent ed by t he calcein green and red alizarin, one week and t wo weeks af t er implant placement respect ively, showed higher values of bone f ormat ion when compared t o t he ot her periods evaluat ed, af t er 4 and 12 weeks of implant placement . The alizarin red bone marker comprised t he peak of bone f ormat ion f or all groups. Administ ered af t er 2 weeks of implant placement , it exhibit ed t he highest levels of marked bone (f ig. 7, 8).
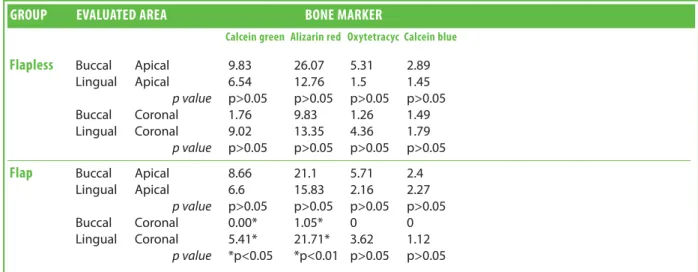
Table 3
Fluorescent analysis. Intra-group evaluation of the percentage of each different bone marker found in the apical and coronal areas of the
experimental groups.
GROUP
EVALUATED AREA
BONE MARKER
P VALUE
Calcein green Alizarin red Oxytetracyc Calcein blue
Flapless
Buccal Apical 9.83 26.07* 5.31 2.89* *p<0.05Coronal 1.76 9.83 1.26 1.49 p>0.05
Lingual Apical 6.54 12.76* / * 1.50* 1.45* *p<0.01 *p<0.01
Coronal 9.02 13.35* 4.36 1.79* *p<0.01
Flap
Buccal Apical 8.66 21.1* 5.71 2.40* *p<0.01Coronal 0 1.05 0 0 p>0.05
Lingual Apical 6.6 15.83 2.16 2.27 p>0.05
Coronal 5.41 21.71* 3.62 1.12* *p<0.01
Table 4
Fluorescent analysis. Intra-group evaluation of the percentage of each different bone marker found in the buccal and lingual areas of the
experimental groups.
GROUP
EVALUATED AREA
BONE MARKER
Calcein green Alizarin red Oxytetracyc Calcein blue
Flapless
Buccal Apical 9.83 26.07 5.31 2.89Lingual Apical 6.54 12.76 1.5 1.45
p value p>0.05 p>0.05 p>0.05 p>0.05
Buccal Coronal 1.76 9.83 1.26 1.49
Lingual Coronal 9.02 13.35 4.36 1.79
p value p>0.05 p>0.05 p>0.05 p>0.05
Flap
Buccal Apical 8.66 21.1 5.71 2.4Lingual Apical 6.6 15.83 2.16 2.27
p value p>0.05 p>0.05 p>0.05 p>0.05
Buccal Coronal 0.00* 1.05* 0 0
Lingual Coronal 5.41* 21.71* 3.62 1.12
St at ist ically signif icant dif f erences were observed bet ween red alizarin and calcein blue f or bone remodeling evaluat ions at t he f lapless buccal apical areas and also at t he f lapless lingual apical and coronal areas (t able 3). St ill considering t he int ra-group analysis, t he f lap buccal apical and t he f lap lingual coronal areas also show ed st at ist ically signif icant dif f erences bet ween t he alizarin red and calcein blue marked bone (t able 3).
When comparing t he buccal and t he lingual areas of t he f lap and f lapless groups, st at ist ically signif icant dif f erences were f ound only bet ween buccal coronal and lingual coronal areas of t he f lap group at t he calcein green and red alizarin periods of applicat ion (t able 4).
DISCUSSION
The f lapless surgical approach signif icant ly f avored t he preservat ion of t he alveolar buccal plat e height af t er immediat e implant placement and a reasonable explanat ion could be t he non- det achment of t he periost eum and it s vascular net work. In t his st udy t he only dif f erence bet ween t he groups was t he f lap elevat ion in t he cont rol group, which exhibit ed at least t wice as more buccal bone loss when compared t o t he f lapless group. Even bet t er result s were demonst rat ed by anot her st udy w it h a similar met hodology, where t he buccal bone loss of 2.11 mm f or t he f lap sit es was conf ront ed by t he 0.6 mm f ound at t he t est immediat e implant s t reat ed wit h f lapless surgery (23).
M any years ago, Wilderman et al. (24) have primarily demonst rat ed t hat “alt hough t he exposure of bone by surgery allow s it s observat ion, some bone resorpt ion is t he penalt y f or t his t ype of examinat ion”. M ore recent ly, t he evaluat ion of t he microvascular responses af t er mucoperiost eal f lap
surgery in dogs conf irmed t hat t he elevat ion of t he periost eum may cause circulat ory insuf f iciency and t hen bone resorpt ion (25). In general, t he bone surf ace t hat is t emporarily exposed usually undergoes a necrot ic process t hat f inishes in bone resorpt ion, wit h except ion of t he broad bone plat e t hat cont ains a signif icant number of marrow spaces and could have less bone height loss at t he end of t he healing period. Considering t hat one of t he main f unct ions of t he periodont al ligament (PDL) blood vessels is t o supply nut rient s t o t he ost eoblast s in t he alveolar bone (13), it is easy t o underst and t hat af t er t oot h ext ract ions, only t he vascularizat ion provided by t he periost eum remains. However, t he elevat ion of mucoperiost eal f laps also compromises t he blood supply f rom t he periost eum. Fickl et al. (26) evaluat ed t he hypot hesis t hat t oot h ext ract ion wit hout t he elevat ion of a mucoperiost eal f lap may decrease t he post - surgery resorpt ion level, and demonst rat ed t hat t he act of leaving t he periost eum in place decreased t he resorpt ion index of t he ext ract ion socket . They highlight ed t hat t he great impact of t his f inding might be w hen dealing w it h t hin periodont al biot ypes, where t he ost eoclast ic act ivit ies of t he int ernal and ext ernal sides could merge t oget her and cause a more pronounced buccal bone plat e loss. The result s of t he present st udy were consist ent wit h t hese st at ement s, especially f or t he f lap approach group in which t he loss of t he buccal bone was more t han 100% great er t han t he lingual bone as shown by t he absolut e measurement s of bone loss around t he implant s. The st at ist ically signif icant dif f erence bet ween f lapless and f lap groups when considering t he buccal bone loss conf irmed t he import ance of periost eum preservat ion in t his t ype of implant t herapy. On t he ot her hand, t here were no signif icant dif f erences bet ween t he f lap and f lapless on t he lingual bone plat e resorpt ion, indicat ing t hat t he
Fig. 8
Dynamic of bone formation at the different evaluated areas in
the flap group.
buccal apical buccal coronal lingual apical lingual coronal Calcein green
Alizarin red
Oxytetracyclin
Calcein blue
Fig. 7
Dynamic of bone formation at the different evaluated areas in
the flapless group.
buccal apical buccal coronal lingual apical lingual coronal Calcein green
Alizarin red
Oxytetracyclin
morphology of t he buccal and lingual plat es might represent anot her crucial f act or in det ermining t he f inal bone resorpt ion.
Based on t hese f act s it could be speculat ed t hat t he immediat e implant t herapy was not t he only f act or t hat inf luenced t he high level of buccal bone height loss of 2,5 mm in relat ion t o t he lingual bone plat e described by Araujo et al. (9) af t er f lap surgery. In our hist ological specimens t he buccal bone crest appeared signif icant ly t hinner when compared t o t he lingual component . This pat t ern was also observed in dif f erent st udies (10,12,17,19,27). Furt hermore, t he bone densit ies of buccal and lingual plat es were very dif f erent in bot h groups. In general, while t he buccal plat es were const it ut ed by a cort ical bone t ype wit h sparse and decreased number of marrow areas, t he lingual bone plat es exhibit ed numerous and large marrow areas. This dif f erence bet ween t he buccal and lingual bone densit ies was st at ist ically signif icant in t he apical port ion of t est and cont rol groups, and w as also st at ist ically signif icant in t he coronal port ion of t he f lap group. This last f inding could mean t hat t his port ion exhibit ed insuf f icient bone marrow spaces and source of blood vessels, and consequent ially compromised angiogenesis t hat is usually relat ed t o bone loss (11, 25). There were no st at ist ically signif icant dif f erences bet ween t he bone densit ies adjacent and dist ant t o t he implant s in bot h groups, but t here was f or t he buccal bone densit ies of t he apical port ion of t he f lapless group. The signif icant lower densit y adjacent t o t he implant of t he buccal bone observed in t he int ra- group evaluat ion (85.80% adjacent and 95.52% dist ant ), and also t he numerical dif f erence bet w een t he groups considering t his paramet er (85.80% f or f lapless and 94.39% f or f lap) could be underst ood as anot her advant age of t he non- det achment of t he periost eum, providing vessels and consequent ly nut rient s t o t he cort ical bone plat es.
All t he implant s present ed good BIC levels and t he result s were very similar bet ween f lapless and f lap groups. The buccal BIC is numerically higher in bot h groups when compared t o t he lingual BIC and t his could be relat ed t o t he higher number of marrow areas f ound in t he lingual bone plat e.
To sum up, t he current st udy support s t he exist ence of a close relat ionship bet ween angiogenesis and bone resorpt ion/ f ormat ion (25), in w hich t he remodeling process is st rongly dependent on t he int eract ion bet ween new blood vessels and bone. Qahash et al. (28) demonst rat ed a signif icant associat ion bet ween t he widt h of t he buccal alveolar ridge and ext ent of bone resorpt ion evaluat ed by incandescent and f luorescent light microscopy. They suggest ed t hat t he widt h of t he buccal alveolar ridge should be at least 2 mm t o maint ain t he alveolar bone level. These observat ions have general
implicat ions f or implant placement w it h most surgical prot ocols, and even more f or immediat e implant at ion. St udies about t he alveolar bone healing pot ent ial in peri- implant crit ical- size def ect s, showed t hat t he t hicker lingual bone plat e provided a large w ound space t hat w as correlat ed w it h enhanced bone regenerat ion, while t he implant s placed closer t o t he buccal plat e were associat ed wit h increased crest al bone loss (29,30).
Anot her comparat ive st udy bet ween f lapless and f lap surgeries f or immediat e post - ext ract ion implant s, also f ound a minor reduct ion of t he buccal bone plat e wit h t he f lapless approach, but emphasized t he import ance of t he locat ion of t he implant s in t he conf ines of t he alveolus (31). Based on t his, it could be discussed t hat one reason f or t he higher buccal bone plat e resorpt ion of Araujo et al. (19) st udy could be due t o t he use of a 4.1 mm diamet er implant s in alveoli t hat are smaller (3.5 mm is t he diamet er of t hird premolars and of 3.9 mm of f ourt h premolars in dogs); in ot her words, t he diamet er of t he implant was great er t han t he alveoli t hemselves.
In t he present st udy t he implant s were placed 1 mm away f rom t he buccal marginal bone wall wit hout invading t he lingual bone plat e wit h t he drill or t he implant . No residual def ect was observed on t he hist ological specimens af t er 12 weeks of healing and t he f ormat ion of new bone could be a possible explanat ion as well as bone loss t o some ext ent . This jumping gap dist ance has already been st udied and it was shown t hat t his def ect may heal wit h new bone and a high degree of osseoint egrat ion wit hout t he use of barrier membranes (32). It was described t hat t his kind of def ect “allowed t he f ormat ion of a coagulum t hat , even in t he absence of a barrier membrane, it w as properly prot ect ed by t he periost eum of t he sof t t issue f lap. In ot her words, during t he healing of a ‘self - cont ained’ bone def ect and in t he presence of a proper periost eum, t he use of a barrier membrane may not be required”, but t his is dependent on t he implant surf ace and t ime of healing allowed af t er implant inst allat ion and gap dist ance.
From t he f luorescence analysis of t he present st udy no st at ist ically signif icant dif f erences were obt ained bet w een t he f lap and f lapless groups, but t he evaluat ion of t he buccal coronal areas show ed numerically higher new bone f ormat ion f or t he f lapless group and t he lack of st at ist ical signif icance could be explained by t he size of t he sample. It was also observed t hat bone remodeling f ollowed a pat t ern not only in t he t wo experiment al groups, but also in t he dif f erent evaluat ed sect ions of t he implant s in an int ra- group analysis – coronal and apical, buccal and lingual.
In t he present st udy t he peak of bone mineralizat ion f or t he groups and subgroups st udied comprised t he period of 2 weeks af t er implant placement as marked by t he red alizarin dye. This is in accordance t o Abrahamsson et al. (33) t hat had already charact erized t his t ime period as a very act ive phase in t he process of mineralizat ion.
The st at ist ically signif icant dif f erences f ound wit hin t he groups, f or example bet ween t he red alizarin and calcein blue marked bone in t he buccal apical area conf irmed t hat bone remodeling is an ongoing process t hat also involves a decrease in t he mineralizat ion levels along t ime. This could explain t he replacement of woven bone by lamellar bone as a physiological process.
Finally, t he evaluat ion w it hin t he experiment al groups comparing buccal and lingual halves showed st at ist ically signif icant dif f erences f or t he f lap coronal area at t he f irst t wo periods of evaluat ion. This result could be explained by t he very low values of bone t hickness f ound f or t he buccal plat e in t his area, reinf orcing t he hist omorphomet ric f indings t hat described t he lingual plat es as t hicker.
CONCLUSION
In summary no major dif f erences in t he dynamics of bone healing, evidenced by t he f luorescence analysis, has been det ect ed bet ween t he f lap and f lapless groups t hat support s t he hypot hesis t hat t he higher loss of buccal bone height is linked t o t he anat omic charact erist ics of t he buccal bone, t he negat ive inf luence of t he det achment of t he periost eum during t he f lap procedure in immediat e implant t herapy and t he presence of a gap bet ween t he implant and t he buccal bone plat e.
Wit hin t he limit at ions of t his st udy, it can be concluded t hat t he f lapless approach f or immediat e post - ext ract ion implant s reduces t he buccal bone plat e resorpt ion
REFERENCES
1. Chen ST, Darby IB, Reynolds EC, Clement JG. Immediat e implant placement post ext ract ion w it hout f lap elevat ion. J Periodont ol 2009;80:163- 172.
2. Knox R, Caudill R, M ef f ert R. Hist ologic evaluat ion of dent al endosseous implant s placed in surgically creat ed ext ract ion def ect s. Int J Periodont ics Rest orat ive Dent 1991;11:364- 375.
3. Lazarra RJ. Immediat e implant placement int o ext ract ion sit es: surgical and rest orant e advant ages. . Int J Periodont ics Rest orat ive Dent 1989;9:333- 343
4. Lundgren D, Rylander H, Andersson M , Johansson C, Albrekt sson T. Healing- in of root analogue t it anium
implant s placed in ext ract ion socket s. An experiment al st udy in t he beagle dog. Clin Oral Im plant s Res 1992;3:136- 143.
5. Nemcovsky CE, Art zi Z, M oses O, Gelernt er I. Healing of marginal def ect s at implant s placed in f resh ext ract ion socket s or af t er 4- 6 w eeks of healing. A comparat ive st udy. Clin Oral Implant s Res 2002;13:410- 419.
6. Paolant onio M , Dolci M , Scarano A, d'Archivio D, di Placido G, Tumini V et al. Immediat e implant at ion in f resh ext ract ion socket s. A cont rolled clinical and hist ological st udy in man. J Periodont ol 2001;72:1560- 1571. 7. Rosenquist B, Ahmed M . The immediat e replacement of
t eet h by dent al im plant s using hom ologous bone membranes t o seal t he socket s: clinical and radiographic f indings. Clin Oral Implant s Res 2000;11:572- 582. 8. Wilson TG, Jr., Schenk R, Buser D, Cochran D. Implant s
placed in im m ediat e ext ract ion sit es: a report of hist ologic and hist omet ric analyses of human biopsies. Int J Oral M axillof ac Implant s 1998;13:333- 341.
9. Araujo M G, Sukekava F, Wennst rom JL, Lindhe J. Tissue m odeling f ollow ing im plant placem ent in f resh ext ract ion socket s. Clin Oral Implant s Res 2006;17:615-624.
10. Araujo M G, Wennst rom JL, Lindhe J. M odeling of t he buccal and lingual bone w alls of f resh ext ract ion sit es f ollow ing implant inst allat ion. Clin Oral Implant s Res 2006;17:606- 614.
11. Novaes AB, Jr., M acedo GO, Suaid FA, Barros RR, Souza SL, Silveira ESAM . Hist ologic evaluat ion of t he buccal and lingual bone plat es in ant erior dog t eet h: possible inf luence on im plant dent ist ry. J Periodont ol 2011;82:872- 877.
12. Spray JR, Black CG, M orris HF, Ochi S. The inf luence of bone t hickness on f acial marginal bone response: st age 1 placement t hrough st age 2 uncovering. Ann Periodont ol 2000;5:119- 128.
13. M at suo M SC, Sait o M , Kishi Y,Takahashi K. Vascularizat ion an unsuccessf ul case f ollow ing guided bone regenerat ion. . Jpn J Oral Biol 2000;42:573- 579. 14. Bragger U, Pasquali L, Kornman KS. Remodelling of
int erdent al alveolar bone af t er periodont al f lap procedures assessed by means of comput er- assist ed densit omet ric image analysis (CADIA). J Clin Periodont ol 1988;15:558- 564.
15. St af f ileno H, Levy S, Gargiulo A. Hist ologic st udy of cellular mobilizat ion and repair f ollow ing a periost eal ret ent ion operat ion via split t hickness mucogingival f lap surgery. J Periodont ol 1966;37:117- 131.
16. Wood DL, Hoag PM , Donnenf eld OW, Rosenberg DL. Alveolar crest reduct ion f ollow ing f ull and part ial t hickness f laps. J of Periodont ology 1972;43:141- 144. 17. Araujo M G, Lindhe J. Dim ensional ridge alt erat ions
f ollow ing t oot h ext ract ion. An experiment al st udy in t he dog. J Clin Periodont ol 2005;32:212- 218.
18. Yaf f e A, Fine N, Binderm an I. Regional accelerat ed phenomenon in t he mandible f ollow ing mucoperiost eal f lap surgery. J Periodont ol 1994;65:79- 83.
19. Araujo M G, Sukekava F, Wennst rom JL, Lindhe J. Ridge alt erat ions f ollow ing im plant placem ent in f resh ext ract ion socket s: an experiment al st udy in t he dog. J Clin Periodont ol 2005;32:645- 652.
t he peri- implant mucosa: a comparison bet w een f lap and f lapless procedures. Oral Surg Oral M ed Oral Pat hol Oral Radiol Endod 2009;107:508- 512.
21. Cho KS, Choi SH, Han KH, Chai JK, Wikesjo UM , Kim CK. Alveolar bone f ormat ion at dent al implant dehiscence def ect s f ollow ing guided bone regenerat ion and xenogeneic f reeze- dried demineralized bone mat rix. Clin Oral Implant s Res 1998;9:419- 428.
22. Donat h K, Breuner G. A m et hod f or t he st udy of undecalcif ied bones and t eet h w it h at t ached sof t t issues. The Sage- Schlif f (saw ing and grinding) t echnique. J Oral Pat hol 1982;11:318- 326.
23. Cardaropoli G M F, Osorio R, Toledano M , Pisani Proenca T, Thomsen P, Tarnow D. Healing f ollow ing t oot h ext ract ion and immediat e implant inst allat ion w it h f lapless surgery. Clin Oral Impl Res 2007;18.
24. Wilderman M N, Went z F, Orban BJ. Hist ogenesis of repair af t er mucogingival surgery. J Periodont ol 1960;31: 283-299.
25. Nobut o T, Suw a F, Kono T, Taguchi Y, Takahashi T, Kanem ura N et al. M icrovascular response in t he periost eum f ollow ing mucoperiost eal f lap surgery in dogs: angiogenesis and bone resorpt ion and f ormat ion. J Periodont ol 2005;76:1346- 1353.
26. Fickl S, Zuhr O, Wacht el H, Bolz W, Huerzeler M . Tissue alt erat ions af t er t oot h ext ract ion w it h and w it hout surgical t rauma: a volumet ric st udy in t he beagle dog. J Clin Periodont ol 2008;35:356- 363.
27. Adell R, Lekholm U, Rockler B, Branemark PI, Lindhe J, Eriksson B et al. M arginal t issue react ions at osseoint egrat ed t it anium f ixt ures (I). A 3- year longit udinal prospect ive st udy. Int J Oral M axillof ac Surg 1986;15:39- 52.
28. Qahash M , Susin C, Polimeni G, Hall J, Wikesjo UM . Bone healing dynamics at buccal peri- implant sit es. Clin Oral Implant s Res 2008;19:166- 172.
29. Polimeni G, Koo KT, Qahash M , Xiropaidis AV, Albandar JM , Wikesjo UM . Prognost ic f act ors f or alveolar regenerat ion: bone f ormat ion at t eet h and t it anium implant s. J Clin Periodont ol 2004;31:927- 932.
30. Wikesjo UM , Susin C, Qahash M , Polimeni G, Leknes KN, Shanaman RH et al. The crit ical- size supraalveolar peri-implant def ect model: charact erist ics and use. J Clin Periodont ol 2006;33:846- 854.
31. Blanco J NV, Aracil L, M unoz F, Ramos I. Ridge alt erat ions f ollow ing immediat e implant placement in t he dog: f lap versus f lapless surgery. . J Clin Periodont ol 2008;35:640-648.
32. Bot t icelli D, Berglundh T, Buser D, Lindhe J. The jumping dist ance revisit ed: An experiment al st udy in t he dog. Clin Oral Implant s Res 2003;14:35- 42.