Abst ract
Submitted: May 28, 2016 0RGL¿FDWLRQ6HSW Accepted: October 27, 2016
Microbiological, lipid and im m unological
SUR¿OHVLQFKLOGUHQZLWKJLQJLYLWLVDQG
t ype 1 diabet es m ellit us
Obj ect iv e: The aim of t his st udy w as t o com par e t he pr evalence of SHULRGRQWDOSDWKRJHQVV\VWHPLFLQÀDPPDWRU\PHGLDWRUVDQGOLSLGSUR¿OHVLQ t ype 1 diabet es children ( DM) wit h t hose observed in children wit hout diabet es ( NDM) , bot h w it h gingivit is. Mat er ial and m et hods: Tw ent y- four DM childr en and t w ent y- seven NDM cont r ols w er e evaluat ed. The per iodont al st at us, JO\FHPLFDQGOLSLGSUR¿OHVZHUHGHWHUPLQHGIRUERWKJURXSV6XEJLQJLYDO sam ples of per iodont al sit es w er e collect ed t o det er m ine t he pr evalence of SHULRGRQWDOPLFURRUJDQLVPVE\3&5%ORRGVDPSOHVZHUHFROOHFWHGIRU,/ǃ TNF-D and I L- 6 analysis using ELI SA kit s. Result s: Periodont al condit ions of DM and NDM pat ient s w er e sim ilar, w it hout st at ist ical differ ences in per iodont al in dices. Wh en con sider in g pat ien t s w it h gin giv it is, all lipid par am et er s evaluat ed w er e highest in t he DM gr oup; Capnocytophaga sputigena and
Capnocytophaga ochracea were m ore prevalent in t he periodont al sit es of DM
childr en. “ Red com plex” bact er ia w er e det ect ed in few sit es of DM and NDM groups. Fusobacterium nucleatum and Campylobacter rectus were frequent ly IRXQGLQERWKJURXSV6LPLODUOHYHOVRI,/ǃ71)D and I L- 6 w er e det ect ed LQ'0DQG1'0FKLOGUHQ&RQFOXVLRQ&OLQLFDODQGLPPXQRORJLFDOSUR¿OHVDUH sim ilar bet w een DM and NDM childr en. The pr esence of Capnocytophaga sputigena and Capnocytophaga ochracea w er e associat ed w it h gingivit is in
DM childr en.
Ke y w or d s: Gingiv it is. Childr en. Diabet es m ellit us. Poly m erase chain
r eact ion. Cyt okines. Cristiane DUQUE1
Mariana Ferreira Dib JOÃO2
Gabriela Alessandra da Cruz
Galhardo CAMARGO3
Gláucia Schuindt TEIXEIRA3
Thamiris Santana MACHADO3
Rebeca de Souza AZEVEDO3
Flávia Sammartino MARIANO2
Natália Helena COLOMBO1
Natália Leal VIZOTO2
Renata de Oliveira
MATTOS-GRANER2
1Universidade Estadual Paulista, Faculdade de Odontologia de Araçatuba, Departamento de Odontologia Infantil e Social, Araçatuba, São Paulo, Brasil
2Universidade de Campinas, Faculdade de odontologia de Piracicaba, Departamento de Diagnóstico Oral, Piracicaba, São Paulo, Brasil.
3Universidade Federal Fluminense, Faculdade de Odontologia de Nova Friburgo, Nova Friburgo, Rio de Janeiro, Brasil.
Corresponding address: Cristiane Duque Universidade Estadual Paulista Faculdade de Odontologia de Araçatuba Departmento de Odontologia Infantil e Social Rua José Bonifácio, 1193 - 16015-050 Araçatuba - São Paulo - Brazil Phone: +55.18.36363315- Fax: +55.18.36363236
I nt r oduct ion
Periodont al disease com prises a group of condit ions
t h a t a f f e ct s t h e g i n g i v a , p e r i o d o n t a l l i g a m e n t ,
cem en t u m , alv eolar b on e, an d t issu e st r u ct u r es
t h at su ppor t t h e t eet h . Th e pr edom in an t f or m of
per iodont al disease in childr en and adolescent s is
gingiv it is13. Ther e is no clear- cut age at w hich t he
gingival react ion t o bact erial insult in children convert s
t o t hat found in adult s. How ever, t her e is a gradual
incr ease in gingival act iv it y fr om ear ly childhood t o
adult age11.
The et iology of per iodont al disease is com plex .
Som e bact er ial species ar e r ecognized as put at ive
p er iod on t al p at h og en s2 6. I n p ar t icu lar, Tannerella
forsythia (Tannerella forsythensis) , Porphyromonas
gingivalis a n d Treponema denticola, k n o w n a s
“ r e d co m p l e x ” p a t h o g e n s, h a v e b e e n i n d i ca t e d
f o r p l ay i n g i m p o r t a n t r o l es i n v a r i o u s f o r m s o f
periodont al diseases7,26. Campylobacter sp., Prevotella
intermedia/Prevotella nigrescens, Fusobacterium
sp., m em b er s of t h e “ or an g e com p lex ”, ar e also
r elat ed t o per iodont al br eak dow n as t he secondar y
g r o u p o f p er i o d o n t al p at h o g en s an d t h e “ g r een
c o m p l e x ,” r e p r e s e n t e d b y t h e c o m b i n a t i o n o f
Eikenella corrodens, Capnocytophaga sputigena, C.
ochracea, C. gingivalis, C. concisus was consider ed
pr im ar y colonizer s and com pat ible w it h per iodont al
healt h26. Cor t elli, et al.6 ( 2009) det ect ed high levels
of Campylobacter rectus associat ed w it h per iodont al
healt h and Prevotella intermedia w it h t he pr esence
RILQÀDPPDWLRQ5RWLPLHWDO18 ( 2010) show ed t hat ,
except for P. gingivalis, per iodont opat hogens such as
A. actinomycetemcomitans, T. forsythia, P. intermedia
an d P. nigrescens DUH UHODWLYHO\ FRPPRQ ¿QGLQJV
in t he oral cav it y of childr en. Thus, t he r elat ionship
bet w een clinical param et er s and t he pr evalence of
several per iodont al pat hogens in childr en need t o be
st udied in gr eat er det ail.
The pat hogenesis of per iodont al disease has been
w idely r ev ised1 6 , 1 7 an d t h er e is a con sen su s t h at , DOWKRXJKEDFWHULDDUHHVVHQWLDOWKH\DUHLQVXI¿FLHQW
for t he disease t o occur16. Micr obial challenge in t he
su b g in g iv al p laq u e m od u lat es t h e h ost im m u n
e-LQÀDPPDWRU\ UHVSRQVH LQ WKH SHULRGRQWDO WLVVXHV17.
Macr ophages and poly m or phonuclear leukocy t es, in
r esponse t o t he chem o- at t ract ant effect of bact er ial
t oxins, such as lipopolysaccharide ( LPS) , are act ivat ed
WRSURGXFHLPSRUWDQWLQÀDPPDWRU\PHGLDWRUV71)D,
,/ǃ,/DQGRWKHUF\WRNLQHV29. These m ediat or s
ar e r esponsible for per iodont al br eak dow n, leading
t o t he clinical signs and sy m pt om s of disease17. A
few st udies evaluat ed t he pr oduct ion of cy t ok ines in
childr en w it h gingiv it is. Ulker, et al.29 ( 2008) found a FRUUHODWLRQEHWZHHQKLJKOHYHOVRI,/ǃDQG71)ĮLQ JLQJLYDOFUHYLFXODUÀXLGRIFKLOGUHQDQGFOLQLFDOVLJQV
of gingiv it is.
6\VWHPLFLQÀDPPDWRU\GLVHDVHVVXFKDVGLDEHWHV
alt er t h e h ost env ir on m en t , an d ar e pr edict ed t o
incr ease t he pat ient ’s v ulnerabilit y t o gingiv it is due
WRFKDQJHVLQWKHLQÀDPPDWRU\UHVSRQVHWRPLFURELDO
challenges12. Clinical st udies have dem onst rat ed t hat
t he presence of diabet es can be considered a risk fact or
for per iodont al disease in childhood19,31.I ndiv iduals
w it h diabet es m ellit us have im pair ed neut r ophil and
m acr ophage funct ioning, alt er ed collagen pr oduct ion,
an d ex ag g er at ed collag en ase act iv it y1 2, p er h ap s OHDGLQJWRWKHSDWLHQW¶VKHLJKWHQHGLQÀDPPDWRU\VWDWH
as int eract ions w it h advanced glycat ion endpr oduct s
( AGEs) hav e been show n t o incr ease m acr ophage
VHFUHWLRQRISURLQÀDPPDWRU\PHGLDWRUV12. Salvi, et al.19
( 2010)IRXQGDKLJKFRQFHQWUDWLRQRI,/ǃLQSDWLHQWV
w it h t y p e 1 d iab et es w h en com p ar ed t o h ealt h y
indiv iduals. Snell- Ber geon, et al.24 ( 2010) evaluat ed
553 pat ient s w it h t y pe 1 diabet es m ellit us and 215
healt hy pat ient s aged bet w een 10 and 22 year s and
observed t hat high levels of I L- 6 and ot her biom arkers
w er e a sso ci a t ed w i t h t h e l i p i d p r o f i l e a n d m ay
collaborat e w it h sy st em ic com plicat ions in indiv iduals
w it h diabet es. These com plicat ions could incr ease t he
pat ient ’s r isk t o develop sever e per iodont al disease31.
Ther e ar e few st udies t hat have ex am ined m icr obial
colon izat ion , im m u n olog ical f act or s an d g in g iv al
healt h dur ing childhood. The aim of t his st udy was
t o com par e t he pr evalence of per iodont al pat hogens,
V\VWHPLFLQÀDPPDWRU\PHGLDWRUVDQGOLSLGSUR¿OHVLQ
t y pe 1 diabet es childr en ( DM) w it h t hose obser ved in
childr en w it hout diabet es ( NDM) , bot h w it h gingiv it is.
Mat er ial and m et hods
St udy populat ion
The st udy pr ot ocol was appr oved by t he Et hics
Com m it t ee of An t on io Ped r o Un iv er sit y Hosp it al
( pr ot ocol 057/ 2010) . Childr en w it h t y pe 1 diabet es
m ellit us ( DM) and childr en w it hout diabet es ( NDM) ,
aged bet w een 7 and 13 year s, w it h m ixed dent it ion,
w er e select ed f or t h is st u d y. I n d iv id u als w it h ou t
diabet es w er e r ecr uit ed fr om t he Pediat r ic Dent ist r y
Clinic and childr en w it h diabet es fr om t he dat abase
k indly pr ov ided by a local Diabet es Associat ion. The
diagnosis of diabet es was given by an endocrinologist .
The exclusion cr it er ia used for subj ect r ecr uit m ent2
w er e: an t ibiot ic pr ophy lax is for den t al t r eat m en t ,
u n co n t r o l l e d sy st e m i c d i se a se s, i m m u n o l o g i ca l
com pr om ise, subj ect s w ho w er e w ear ing or t hodont ic
devices, subj ect s who had been undergoing periodont al
t r eat m ent 1 2 m ont hs befor e t he beginning of t he
st udy, t hose w ho had been t ak ing ant ibiot ics w it hin 6
m ont hs pr ior t o t he clinical ex am inat ion, t hose w it h
ex t ensive car ies lesions, indiv iduals w ho w er e using
an ant isept ic solut ion dur ing 3 m ont hs per iod and
sm oker s. Par ent s or legal guar dians w er e infor m ed of
t he st udy and signed an infor m ed consent for m and
com plet ed an int er v iew r egar ding t he m edical and
dent al hist or ies of t he childr en.
Clinical m easur em ent s
The follow ing clinical param et er s w er e m easur ed:
car ies index [ ( dm f/ DMF – decay ( d) , m issing ( m )
DQG¿OOLQJIGHFLGXRXVGPIDQGSHUPDQHQW'0)
t eet h)6, pr obing dept h ( PD) , plaque index ( PI )23 and
gingival index ( GI ) ]10, by t w o pr ev iously calibrat ed
ex am in er s ( CD an d GACGC) , u sin g a per iodon t al
pr obe ( PCPUNC 15) ( Hu- Fr iedy, Chicago, I L, USA)
at four sit es ( m esiobuccal, m id- buccal, dist o- lingual,
m id - lin g u al) p er t oot h . Th e f ollow in g t eet h w er e
H[DPLQHG DOO ¿UVW SHUPDQHQW PRODUV DOO VHFRQG
d ecid u ou s m olar s, t w o u p p er p er m an en t in cisor s
and low er per m anent incisor s. Per m anent t eet h w er e
fully er upt ed. The int ra- ex am iner and int er- ex am iner
agr eem ent of t he cat egor ical var iables ( PI , GI ) using
t he Kappa calculat ion, at t oot h level, was 0.72 and
0 . 6 8 , r esp ect iv ely. Rep r od u cib ilit y of con t in u ou s
var iables ( PD) was 0.71 and 0.69, r espect ively, as
H[DPLQHG E\ WKH LQWUDFODVV FRUUHODWLRQ FRHI¿FLHQW
( I CC) .
I nt raoral sam ples collect ion
Befor e t he int raoral collect ion pr ocedur es, cot t on
r olls w er e applied t o pr event cont am inat ion of t he
VDPSOLQJDUHDZLWKRWKHURUDOÀXLGV7KHVXSUDJLQJLYDO ELR¿OPZDVJHQWO\UHPRYHGXVLQJVWHULOHFRWWRQSHOOHWV DQGVXEJLQJLYDOELR¿OPVDPSOHVZHUHFROOHFWHGXVLQJ
st er ile paper point s ( Tanar i # 30, Tanar im an I ndust r ial
Lt da., Manacapur u, AM, Brazil) , w hich w er e inser t ed
t o t he dept h of t he gingival sulci for 6 0 seconds.
This pr ocedur e was per for m ed for each of t he four
sit es pr ev iously select ed ( m esiobuccal sulci of t hr ee
perm anent m olars and one perm anent incisor, select ed
r an d om ly or m esiob u ccal su lci of f ou r d ecid u ou s
m olar s) and t he paper point s of each subj ect w er e
inser t ed in a m icr ot ube cont aining 1 m L of Tr is- EDTA
solut ion ( 10 m M Tr is–HCl, 0. 1 m M EDTA, pH 8. 0)
RQLFH3RROHGELR¿OPVZHUHVHSDUDWHGDFFRUGLQJWR
dent it ion ( per m anent or deciduous) for each pat ient .
7KHVDPSOHVZHUHVWRUHGDWí&XQWLOWKHDQDO\VHV
Blood sam ples collect ion
Pat ient s w er e asked t o r educe t he int ake of fat t y
foods t he night befor e collect ing t he blood sam ples.
Bl o o d sa m p l e s w e r e co l l e ct e d b y a sp e ci a l i ze d
pr ofessional fr om t he per ipher ical vein ( cubit al fossa)
of indiv iduals w ho had an over night fast . Sam ples
w er e collect ed in vacuum collect ion t ubes and sent
t o Raul Ser t ã Hospit al Laborat or y at Nova Fr ibur go/
RJ for clinical analy sis [ fast ing glucose levels ( GL) ,
g ly cosy lat ed h em og lob in – ( Hb A1 c) , t r ig ly cer id es
( TRG) , t ot al cholest erol ( TC) , high–densit y lipoprot ein
( HDL) , low- densit y lipoprot ein ( LDL) , very low- densit y
OLSRSURWHLQ9/'/DQGWRWDOOLSLGV7/@XVLQJVSHFL¿F
k it s ( Gold Analisa, Belo Hor izont e/ MG) . One t ube was
cent r ifuged ( 3000 r pm / 10 m in) and t he blood ser um
ZDVFDUHIXOO\FROOHFWHGDOLTXRWHGDQGIUR]HQDWí&
for im m unological analy sis.
%DFWHULXPVSHFL¿F3&5
The subgingival sam ples w er e t haw ed, vor t exed
and cent r ifuged ( 10,000 r pm / 10 m in) . Aft er r em oval
o f t h e p a p e r p o i n t s a n d su p e r n a t a n t , sa m p l e s
w er e subm it t ed t o DNA ex t ract ion using a pr ot ocol
described by Sardi, et al.21 ( 2011) ; bact erial m olecular LGHQWL¿FDWLRQ ZDV FDUULHG RXW E\ 3RO\PHUDVH &KDLQ
React ion m et hod using a t her m al cycler ( TPer sonal,
%LRPHWUD*HUPDQ\7KHEDFWHULXPVSHFL¿FSULPHU
seq u en ces u sed ar e list ed in t h e cor r esp on d en t
r efer ences: Aggregatibacter actinomycetemcomitans
( Aa)5; Campylobacter rectus ( Cr )2; Capnocytophaga
ochracea ( Co)5; Capnocytophaga sputigena ( Cs)5;
Eikenella corrodens ( Ec)2; Fusobacterium nucleatum
( Fn)28; Tannerella forsythia ( Tf )2; Treponema denticola
( Td)30; Porphyromonas gingivalis ( Pg)18; Prevotella
intermedia ( Pi)2; Prevotella nigrescens ( Pn )2. PCR
r eact ions w er e st andar dized for each pr im er using
a posit ive cont r ol and dist illed wat er as a negat ive
FRQWURO 3&5 DPSOL¿FDWLRQV ZHUH SHUIRUPHG XVLQJ 0RIG173VP0RI0J&O20RIHDFK
pr im er, 1.25 U of Taq DNA poly m erase ( I nv it r ogen,
Brazil) and appr ox im at ely 10 ng of genom ic DNA, t o
REWDLQDYROXPHRIO7KHUPDOFRQGLWLRQVRIHDFK
pr im er was t est ed, follow ing t he init ial pat t er n: DNA
denat urat ion at 95oC for 5 m inut es, 35 cycles at 95oC
for 30 seconds, pr im er hy br idizat ion at 55oC- 62oC
( depending on t he pr im er ) for 30 seconds, ex t ension
at 72o&IRUPLQXWHDQG¿QDOL]LQJWKHUHDFWLRQDWoC
for 7 m inut es2. The PCR pr oduct s w er e separat ed by
elect r ophor esis in 2% agar ose gels and Tr is- borat
e-EDTA r unning buffer. The DNA was st ained w it h 0.5
ug/ m L et hidium br om ide and v isualized under UV
illum inat ion ( Phar m acia LKB- Macr oVue, San Gabr iel,
CA, USA) . Each gel r eceived a 100 pb or 1 Kb DNA
Ladder ( I nv it r ogen, Brazil) .
ELI SA assays
,/ǃ 71)D a n d I L- 6 s e r u m l e v e l s w e r e det erm ined by ELI SA kit s ( R&D Syst em s, Minneapolis,
USA) , accor ding t o t he m anufact ur er ’s inst r uct ions.
Ser um sam ples w er e assayed at 1: 10 dilut ions and
HYDOXDWHGLQGXSOLFDWH%LRPDUNHUTXDQWL¿FDWLRQZDV
p er f or m ed u sin g a m icr op lat e r ead er ( Molecu lar
Devices, Pr ogram a Ver sa Max) . Result s w er e r epor t ed
as pg/ m L.
St at ist ical analysis
The st at ist ical analy sis was per for m ed using SPSS
St at ist ics 1 7 . 0 ( I BM I n c., Ch icago, I L, USA) . Th e
subj ect charact er ist ics ( gender, age, fast ing glucose
lev el, HBA1 c lev el an d dm f / DMF) w er e com par ed
bet w een DM an d NDM u sin g t h e St u den t ’s t - t est
for quant it at ive var iables and Mann- Whit ney U t est
for qu alit at iv e var iables. Clin ical param et er s w er e
com par ed bet w een DM and NDM using Mann- Whit ney
t est , except for PD, w hich was subm it t ed t o St udent ’s
t - t est . The percent age of sit es w it h t he t est ed bact eria
an d d at a f r om t h e q u est ion n air e w er e com p ar ed
bet w een DM and NDM apply ing t he Chi- squar e t est .
I m m u n o l o g i cal an d l i p i d p r o f i l es w er e assessed
using St udent ’s t - t est . The Pear son cor r elat ion t est
ZDV DSSOLHG WR ¿QG SRVLWLYH DVVRFLDWLRQV EHWZHHQ
periodont al st at us and ot her clinical param et ers ( lipid,
m icr ob iolog ical an d im m u n olog ical p r of iles) . Th e
GLIIHUHQFHVZHUHFRQVLGHUHGVLJQL¿FDQWZKHQS
Result s
Clinical charact er ist ics of t he st udy populat ion
Tw ent y- four childr en w it h t y pe 1 diabet es m ellit us
and 27 childr en w it hout diabet es par t icipat ed in t his
VWXG\1RVLJQL¿FDQWGLIIHUHQFHZDVREVHUYHGEHWZHHQ
DM and NDM gr oups, consider ing gender, age and
caries level evaluat ion ( dm ft / DMFT) . Table 1 describes
t he charact er ist ics of t he st udy populat ion ( DM and
NDM gr oups) . Fast ing glucose and HBA1c levels w er e
st at ist ically differ ent bet w een t he gr oups, always w it h
t he highest values for t he DM pat ient s. Ther e w er e
QR VLJQL¿FDQW GLIIHUHQFHV IRU 3, DQG *, VFRUHV DQG
all PD m easur em ent s w hen com par ing DM and NDM
for bot h dent it ions, indicat ing t hat bot h gr oups had
sim ilar periodont al condit ions. Quest ionnaires given t o
childr en and t heir par ent s pr ov ided infor m at ion about
t he gingiv it is hist or y and dent al car e of pat ient s, such
as pr esence of gingival bleeding, halit osis, m out h
br eat hing and t oot h br ushing habit s. Ther e w er e no
differences bet ween DM and NDM for t hese param et ers
evaluat ed. Table 1 also present s lipid and im m unologic
SUR¿OHVRI'0DQG1'0JURXSVFRQVLGHULQJFKLOGUHQ ZLWKJLQJLYLWLVS$OOOLSLGSDUDPHWHUVHYDOXDWHG
w er e t he highest in t he DM gr oup; how ever, st at ist ical
differ ence was obser ved only for HDL, TRG and TL.
Ther e w er e no st at ist ical differ ences bet w een DM and
1'0IRU,/ǃ71)D and I L- 6 det ect ed in t he ser um of childr en.
Associat ion bet w een per iodont al st at us and
OLSLGDQGLPPXQRORJLFDOSUR¿OHV
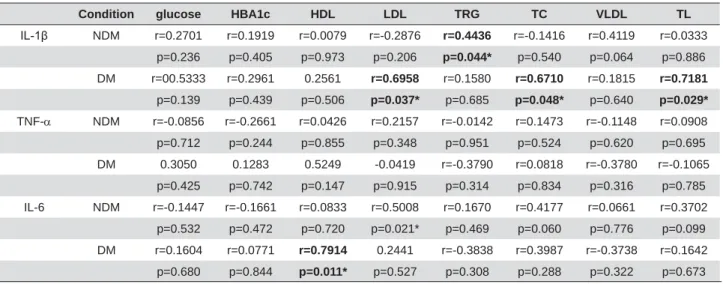
Tables 2 and 3 show t he associat ions bet w een
SHULRGRQWDOVWDWXVDQGOLSLGDQGLPPXQRORJLFDOSUR¿OHV
When com par ing t he per iodont al st at us and cy t ok ine
levels, TNF-D was cor r elat ed w it h PI for deciduous t eet h ( Pear son cor r elat ion, r = 0.935, p= 0.002) and
w it h GI f or decidu ou s t eet h ( Pear son cor r elat ion ,
r = 0. 772, p= 0. 042) in pat ient s w it h diabet es. I L- 6
was cor r elat ed w it h PI for deciduous t eet h ( Pear son
cor r el at i on , r = 0 . 9 2 2 , p = 0 . 0 0 3 ) i n p at i en t s w i t h
diabet es. When consider ing t he im m unological and
OLSLG SUR¿OHV ,/ǃ ZDV SRVLWLYHO\ FRUUHODWHG ZLWK
LDL ( Pear son cor r elat ion , r = 0 . 6 9 6 , p = 0 . 0 3 7 ) TC
( Pear son cor r elat ion , r = 0 . 6 7 1 , p = 0 . 0 4 8 ) an d TL
( Pear son cor r elat ion , r = 0 . 7 1 8 1 , p= 0 . 0 2 9 ) f or DM
childr en and w it h TRG ( r = 0.444, p= 0.044) for NDM
ch ildr en . I L- 6 w as posit iv ely cor r elat ed w it h HDL
LDL ( Pear son cor r elat ion, r = 0.501 p= 0.021) for NDM.
0LFURELRORJLFDOSUR¿OH
Figur e 1 and Table 4 show r elat ive and absolut e
fr equencies of per iodont al bact er ia, as w ell as each
species com binat ion, det ect ed in t he crevicular gingival
ÀXLGRI'0DQG1'0FKLOGUHQFRQVLGHULQJGHFLGXRXV DQG SHUPDQHQW WHHWK DQG *, 7KH '0 JURXS
present ed st at ist ically higher levels of Capnocytophaga
sputigena for bot h dent it ions and Capnocytophaga
ochracea for per m anent dent it ion w hen com par ed t o
t he NDM gr oup. Prevotella intermedia was det ect ed
i n o n l y t w o D M p a t i e n t s a n d Aggregatibacter
actinomycetemcomitans w as n ot d et ect ed in an y
ch ild r en in t h is st u d y. Fusobacterium nucleatum
and Campylobacter rectus w er e t he m ost pr evalent
bact er ia, follow ed by Eikenella corrodens, in bot h
populat ions. Bact er ia fr om t he “ r ed com plex ” w er e
det ect ed in few sit es of bot h t he DM and NDM gr oups.
The best com binat ion of “ orange com plex ” pat hogens
w as Fusobacterium nucleatum and Campylobacter
rectus. Ho w e v e r, b o t h o f t h e m co m b i n e d w i t h
Prevotella nigrescens h ar b or ed ar ou n d 4 2 % an d
50% of NDM and DM gr oups sit es, r espect ively. The
“ gr een com plex ” – r epr esent ed by t he com binat ion of
Eikenella corrodens, Capnocytophaga sputigena and
NDM DM
General Characteristics
Gender n (%)
Male Female
13 (48.1) 14 (1.9)
12 (50) 12 (50)
Age (in years) Mean±SD
9.62 ±1.86 9.45 ±1.69
Fasting glucose level (mg/dL) Mean±SD
78.7± 8.10* 101.74 ±40.64
HbA1c % (mmol/mol) Mean [SD]
4.42 ±0.61* 6.94±1.58
Children using insulin for more than 1 year n (%) dmft/DMFT
-0.93/0.11
13 (54.16) 0.94/0.13
Periodontal status
Deciduous teeth
PI** 24.2 (63) 6.2 12.6 (4.1) 3.5
GI** 15.3 (0) 5.04 16.3 (6.25) 6.0
PS 1.41±0.49 1.34±0.29
Permanent teeth
PI** 32 (19.4) 6.0 24.7 (25) 4.62
GI** 19.1 (12.5) 3.9 17.6 (8.33) 4.5
PS 1.41±0.50 1.48±0.48
/LSLG3UR¿OH
HDL 45.9 (8.4)* 54.4(15.5)
LDL 82.7(21.5) 106.4 (37.5)
TRG 66.9(27.0)* 78.9(53.3)
TC 142.5(27.7) 167.5(46.5)
VLDL 13.5 (5.6) 16.12 (10.4)
TL 389.0(78.1)* 490(143.5)
,PPXQRORJLFDOSUR¿OH
,/ȕ 1.98 (0.29) 1.57 (0.31)
TNF-D 15.01 (2.91) 11.48 (5.73)
IL-6 2.18 (0.29) 1.26 (0.30)
NDM – children without diabetes / DM – children with type 1 diabetes mellitus
PI = Plaque index, GI = Gingival Index, PD = depth probing, HDL = high density lipoprotein, LDL = low density lipoprotein, TRG = triglycerides, TC = total cholesterol, VLDL = very low density lipoprotein, TL = total lipids (values in mg/dL).
* Statistical difference when compared NDM vs. DM, according to the Student’s t-test for quantitative data and Mann-Whitney test for
TXDOLWDWLYHGDWDS
0HDQ0HGLDQVWDQGDUGHUURURISHUFHQWDJHRIVFRUHV
Capnocytophaga ochracea LQWKLVVWXG\±ZDVGH¿QLWHO\
m ore prevalent in t he periodont al sit es of DM children.
Even w it h t he inclusion of Campylobacter rectus in t he
“ gr een com plex ”, t his r esult did not change.
Discussion
Most st udies on t he t opic have concluded t hat DM
FKLOGUHQKDYHKLJKHUOHYHOVRIJLQJLYDOLQÀDPPDWLRQ
w hen com par ed t o NDM pat ient s, suggest ing t hat
d iab et es is an ag g r av at in g f act or f or p er iod on t al
disease1,15,19,31. However, in t his st udy, children showed
good gingival healt h, w hich is dem onst rat ed by t he
low per cent age of scor es above 2 in Plaque I ndex and
Gingival I ndex and reduced probing dept hs ( average of
approxim at ely 1.5 m m ) , in bot h dent it ions, regardless
of t he pr esence of diabet es m ellit us. These r esult s ar e
in agr eem ent w it h t he dat a obt ained by Sbor done,
et al.2 5 ( 1 9 9 8 ) w h o ob ser v ed t h at , ev en af t er 3
y ear s of m onit or ing, no differ ences w er e det ect ed
in t he per iodont al evaluat ion of pat ient s w it h t y pe 1
diabet es m ellit us w hen com par ed t o pat ient s w it hout
diabet es25. A lim it at ion of t his st udy is t he sam ple
size t hat could have r educed t he pr obabilit y t o det ect
difference bet ween groups. Moreover, when com paring
per iodont al st udies, differ ences m ay be det ect ed in
t he clinical ex am inat ions r elat ed t o r ecor ding design,
t y pe/ num ber of sit es assessed and t he per iodont al
Condition glucose HBA1c HDL LDL TRG TC VLDL TL
,/ȕ NDM r=0.2701 r=0.1919 r=0.0079 r=-0.2876 r=0.4436 r=-0.1416 r=0.4119 r=0.0333
p=0.236 p=0.405 p=0.973 p=0.206 p=0.044* p=0.540 p=0.064 p=0.886
DM r=00.5333 r=0.2961 0.2561 r=0.6958 r=0.1580 r=0.6710 r=0.1815 r=0.7181
p=0.139 p=0.439 p=0.506 p=0.037* p=0.685 p=0.048* p=0.640 p=0.029*
TNF-D NDM r=-0.0856 r=-0.2661 r=0.0426 r=0.2157 r=-0.0142 r=0.1473 r=-0.1148 r=0.0908
p=0.712 p=0.244 p=0.855 p=0.348 p=0.951 p=0.524 p=0.620 p=0.695
DM 0.3050 0.1283 0.5249 -0.0419 r=-0.3790 r=0.0818 r=-0.3780 r=-0.1065
p=0.425 p=0.742 p=0.147 p=0.915 p=0.314 p=0.834 p=0.316 p=0.785
IL-6 NDM r=-0.1447 r=-0.1661 r=0.0833 r=0.5008 r=0.1670 r=0.4177 r=0.0661 r=0.3702
p=0.532 p=0.472 p=0.720 p=0.021* p=0.469 p=0.060 p=0.776 p=0.099
DM r=0.1604 r=0.0771 r=0.7914 0.2441 r=-0.3838 r=0.3987 r=-0.3738 r=0.1642
p=0.680 p=0.844 p=0.011* p=0.527 p=0.308 p=0.288 p=0.322 p=0.673
3RVLWLYHFRUUHODWLRQVREWDLQHGE\3HDUVRQFRUUHODWLRQDQDO\VLVVLJWDLOHGS
Table 2- Associations between lipid and immunological results for children with gingival bleeding, considering NDM and DM groups
Condition PID PIP PIT GID GIP GIT PDD PDP PDT
/ȕ NDM r=-0.2368 r=-0.1314 r=-0.0873 r=0.3629 r=0.2810 r=0.3969 r=0.1170 r=0.5629 r=0.3910 p=0.459 p=0.684 p=0.787 p=0.246 p=0.376 p=0.201 p=0.717 p=0.057 p=0.209
DM r=0.4102 r=0.5387 r=0.5664 r=0.2995 r=0.2363 r=0.2847 r=-0.1141 r=0.2819 r=0.0619
p=0.361 p=0.212 p=0.185 p=0.514 p=0.610 p=0.536 p=0.807 p=0.540 p=0.895
TNF-D NDM r=0.3277 r=0.0482 r=0.3740 r=0.0010 r=-0.5255 r=-0.3758 r=-0.2531 r=-0.7000 r=-0.5589 p=0.298 p=0.882 p=0.231 p=0.998 p=0.079 p=0.229 p=0.427 p=0.011* p=0.059 DM r=0.9346 r=0.6450 r=0.8011 r=0.7719 r=0.3044 r=0.5176 r=0.0570 r=0.0382 r=0.0523
p=0.002* p=0.118 p=0.030* p=0.042* p=0.507 p=0.234 p=0.903 p=0.935 p=0.911 IL-6 NDM r=-0.2206 r=-0.2787 r=-0.3017 r=-0.1404 r=-0.1070 r=-0.1654 r=-0.2270 r=-0.3676 r=-0.3570
p=0.491 p=0.380 p=0.341 p=0.663 p=0.741 p=0.607 p=0.478 p=0.240 p=0.255
DM r=0.9227 r=0.6076 r=0.7789 r=0.5371 r=0.0501 r=0.2591 r=0.0313 r=-0.0642 r=-0.0109 p=0.003* p=0.148 p=0.039* p=0.214 p=0.915 p=0.575 p=0.947 p=0.891 p=0.982
Table 3- Associations between clinical (PI, GI and PD) and immunological results for children with gingival bleeding, considering NDM
and DM groups
PID = Plaque index for deciduous teeth, PIP = Plaque index for permanent teeth, PIT = Plaque index for all teeth, GID = Gingival index for deciduous teeth, GIP = Gingival index for permanent teeth, GIT=Gingival index for all teeth. PDD = probing depth for deciduous teeth, PDP= probing depth for permanent teeth, PDT=probing depth for all teeth.
Deciduous teeth Permanent teeth Total NDM
(13 sites)
DM (17 sites)
NDM (22 sites)
DM (20 sites)
NDM (35 sites)
DM (37 sites)
Red complex Pg+Tf 1(7.7) 2 (11.8) 5 (22.7) 5 (25) 6 (17.2) 7 (18.9)
Pg+Td 0 0 0 1 (5) 0 1 (2.7)
Tf+Td 0 2 (11.8) 1(4.5) 2 (10) 1 (2.8) 4 (10.8)
Pg+Tf+Td 0 0 0 1 (5) 0 1 (2.7)
Orange complex Pi+Fn 0 0 0 2 (10) 0 2 (5.8)
Pi+Pn 0 0 0 0 0 0
Pi+Cr 0 0 0 2 0 2 (5.8)
Fn+Pn 5 (38.4) 9 (52.9) 10 (45.5) 10 (50) 15(42.8) 19 (51.4)
Fn +Cr 11 (84.6) 15 (88.2) 21 (95.5) 19(95 32 (91.4) 34 (91.9)
Cr+Pn 5 (38.4) 8 (47.1) 10(45.5) 10 (50) 15 (42.9) 18 (48.6)
Pi+Fn+Pn 0 0 0 0 0 0
Pi+Fn+Pn+Cr 0 0 0 0 0 0
Green complex Ec+Cs 0* 11 (64.7) 2 (9)* 10 (50) 2 (5.7)* 21 (56.8)
Ec+Co 4 (30.7) 9 (52.9) 4 (18.1)* 10 (50) 8 (22.9)* 19 (51.4)
Cs+Co 0* 9 (52.9) 1 (4.5)* 9 (45) 1 (2.8)* 18 (48.6)
Ec+Cs+Co 0* 9 (52.9) 1 (4.5)* 7 (35) 1 (2.8)* 16 (43.2)
Green complex (+Cr) Ec+Cr 11 (84.6) 15 (88.2) 21 (95.5) 17 (85) 32 (91.4) 32 (86.5)
Co+Cr 4 (30.7) 7 (41.1) 4 (18.1)* 12 (60) 8 (22.9)* 19 (51.4)
Cs+Cr 0* 9 (52.9) 2 (9)* 13 (65) 2 (5.4)* 22 (59.5)
Ec+Cs+Cr 0* 9 (52.9) 2 (9)* 11 (55) 2 (5.4)* 20 (54.0)
Ec+Co+Cr 4 (30.7) 7 (41.1) 2 (9)* 10 (50) 6 (17.1)* 17 (45.9)
Cs+Co+Cr 0* 7 (41.1) 1 (4.5)* 9 (45) 1 (2.8)* 16 (43.2)
(Ec+Cs+Co)+ Cr
0* 7(41.1) 1 (4.5)* 7 (35) 1 (2.8)* 14 (37.8)
Table 4-$EVROXWHDQGUHODWLYHIUHTXHQF\YDOXHVQRIEDFWHULDFRPELQDWLRQVGHWHFWHGRQFUHYLFXODUJLQJLYDOÀXLGRIFKLOGUHQZLWK
gingival bleeding, considering deciduous and permanent teeth
6LJQL¿FDQWGLIIHUHQFHEHWZHHQ'0DQG1'0DFFRUGLQJWRWKH&KLVTXDUHȤWHVWS
6LJQL¿FDQWGLIIHUHQFHEHWZHHQ'0DQG1'0LQGHFLGXRXVWHHWKDFFRUGLQJWRWKH&KLVTXDUHȤWHVWS 6LJQL¿FDQWGLIIHUHQFHEHWZHHQ'0DQG1'0LQSHUPDQHQWWHHWKDFFRUGLQJWRWKH&KLVTXDUHȤWHVWS
Figure 1-)UHTXHQF\RIEDFWHULDGHWHFWHGRQFUHYLFXODUJLQJLYDOÀXLGRIFKLOGUHQZLWKJLQJLYDOEOHHGLQJ*,FRQVLGHULQJGHFLGXRXVDQG
pr obe used t o m easur e per iodont al disease15. The
pr ot ocol used in t his st udy ( four per iodont al sit es)
show ed t he sm allest bias and highest sensit iv it y of
pr evalence est im at es am ongst ot her t est ed pr ot ocols,
accor ding t o Susin, et al.27 ( 2005) . Addit ionally, good
oral hygiene habit s, as pr esent ed in t his st udy, helped
t o m aint ain t he per iodont al healt h of bot h gr oups.
2WKHULPSRUWDQWIDFWRUVWKDWFRXOGDOVRKDYHLQÀXHQFHG
t he clinical r esult s of differ ent st udy ar e t he durat ion
of diabet es and t he glucose levels1. Al- Khabbaz, et
al.1 ( 2 0 1 3 ) obser v ed t h at , in ch ildr en w it h t y pe 1 GLDEHWHV SHULRGRQWLWLV ZDV VLJQL¿FDQWO\ DVVRFLDWHG
w it h longer durat ion of diabet es and older age at
diagnosis of diabet es. St udies hav e dem onst rat ed
t h at poor m et abolic con t r ol, in clu din g h igh lev els
of fast ing glucose and glycosy lat ed hem oglobin ar e
im port ant fact ors t hat could increase t he suscept ibilit y
t o per iodon t al disease, as w ell as ot h er sy st em ic
com plicat ions of diabet es m ellit us3,22.
Ch i l d r e n a n d a d o l e sce n t s w i t h u n co n t r o l l e d
g l y cem i c co n t r o l , r ep r esen t ed b y h i g h er Hb A1 c
concent rat ions or higher fast ing glucose, had higher
fr equency of car ies and gingivit is22. I n t his st udy, t he
levels of HbA1c found in DM childr en w er e st at ist ically
higher t han t hose observed in t he cont rol children, but
according t o accept able glycem ic param et ers, denot ing
low in f lu en ce of g ly cem ic con t r ol on p er iod on t al
param et er s. Lim , et al.9 ( 2007)evaluat ed 181 adult
pat ient s w it h diabet es and st udied t he r elat ionship
EHWZHHQPHWDEROLFFRQWUROPDUNHUVDQGLQÀDPPDWLRQ
and t he sever it y of per iodont al disease in pat ient s
w it h diabet es m ellit us. These aut hor s found posit ive
cor r elat ions bet w een HbA1c and t he per cent age of
VLWHVZLWKSURELQJGHSWKVPPWRWDOFKROHVWHURO
LDL and t r iglycer ides. Posit ive associat ions bet w een
SHULRGRQWDOVWDWXVDQGOLSLGDQGLPPXQRORJLFDOSUR¿OHV
were found in t his st udy. Snell- Bergeon, et al.24 ( 2010)
evaluat ed 553 pat ient s w it h t y pe 1 diabet es m ellit us
and 215 healt hy pat ient s, aged bet w een 10 and 22
y ear s, an d obser v ed t h at h igh lev els of I L- 6 an d
¿EULQRJHQZHUHDVVRFLDWHGZLWKOLSLGSUR¿OHDQGPD\
collaborat e w it h sy st em ic com plicat ions in indiv iduals
w it h diabet es. The sam e was obser ved in our st udy.
I L- 6 was posit ively cor r elat ed w it h LDL, TC and TL for
bot h gr oups. Alt hough m ost of t he lipid param et er s
w er e higher in DM childr en w hen com par ed t o NDM
childr en, st at ist ical differ ences w er e obser ved only
for HDL, TRG and TL. Lar ger sam ples could increase WKHFKDQFHRI¿QGLQJDsigni¿cant difference for t hese
param et er s. St udies evaluat ing lipid param et er s and
per iodont al disease in childr en or adolescent s w it h
diabet es w er e not found.
I n t his st udy, t he pr evalence of bact er ia fr om t he
“ r ed com plex ” (Porphyromonas gingivalis, Tannerella
forsythia an d Treponema denticola) w as low an d
t here was no difference bet w een DM and NDM groups.
These bact er ia have been r elat ed t o t he pat hogenesis
of per iodont al disease and ar e fr equent ly found in
pat ient s w it h chr onic per iodont it is7. When consider ing
t he “ orange com plex”, P. intermedia was det ect ed only
in t he perm anent t eet h of t wo pat ient s. Fusobacterium
nucleatum and Prevotella nigrescens w er e det ect ed in
about half of t he evaluat ed sit es on bot h dent it ions for
bot h DM and NDM subj ect s. One int erest ing result was
t he m ar ked com binat ion of Fusobacterium nucleatum
and Prevotella nigrescens in t he per m anent dent it ion.
Ok uda, et al.14 ( 2012) obser ved sy ner gism bet w een
Prevotella species, including Prevotella nigrescens,
and Fusobacterium nucleatumLQELR¿OPIRUPDWLRQ
suggest ing t hat t hese Gram - negat ive bact er ia in t he
subgingival cr evice could play an im por t ant r ole in t he
developm ent of chr onic per iodont it is.
Campylobacter rectus has been included in t he
“ orange com plex ”, w hich is consider ed a secondar y
group of pat hogens in periodont al infect ions26. However,
one st udy has det ect ed high levels of Campylobacter
rectus associat ed wit h periodont al healt h6, as observed
in t his st udy. The “ green com plex” – represent ed by t he
com binat ion of Eikenella corrodens, Capnocytophaga
sputigena an d Capnocytophaga ochracea – w as
GH¿QLWHO\PRUHSUHYDOHQWLQWKHSHULRGRQWDOVLWHVRI
ch ildr en w it h DM. Kim u ra, et al.8 ( 2 0 0 2 )obser v ed
t hat som e put at ive per iodont al bact er ia, such as E.
corrodens, A. actinomycetemcomitans, C. sputigena,
C. ochracea and C. rectus, colonize ear lier in t he oral
cav it y t han ot her species also r elat ed t o per iodont al
disease. Ciant ar, et al.4 ( 2005) showed higher num bers
of Capnocytophaga spp. in per iodont it is sit es of DM
pat ient s in com par ison w it h healt hy sit es in DM and
NDM adult pat ient s. C. ochracea and C. granulosa
w er e t he m ost pr evalent species. Sak alausk iene, et
al.20 ( 2014) obser ved a st r ong r elat ionship bet w een
t he pr esence of F. nucleatum and Capnocytophaga
spp. and poor er m et abolic cont r ol in t y pe 1 diabet es
pat ien t s ( HbA1 c) an d in all clin ical par am et er s of
periodont al pat hology. Few st udies have evaluat ed t he
m icrobiot a from subgingival sit es of children w it h t ype
t he r elat ionship bet w een per iodont al pat hogens and
diabet es w er e found19,25.
7KHLQÀDPPDWRU\KRVWUHVSRQVHWRDQRUDOEDFWHULDO
challenge is a cr it ical det er m inant in t he out com e of
SDWLHQW KHDOWK RU GLVHDVH 6\VWHPLF LQÀDPPDWRU\
diseases, such as diabet es, alt er t he host environm ent
an d cou ld in cr ease t h e p at ien t ’s v u ln er ab ilit y t o
JLQJLYLWLVGXHWRFKDQJHVLQWKHLQÀDPPDWRU\UHVSRQVH
t o m icr obial challenges12,19,31*LQJLYDOFUHYLFXODUÀXLG
is considered a good source of locally and syst em ically
der ived biom ar ker s of per iodont al disease. How ever,
WKH FROOHFWLRQ RI JLQJLYDO FUHYLFXODU ÀXLG LQ FKLOGUHQ LVGLI¿FXOWEHFDXVHWKHJLQJLYDOVXOFLLQWKHSULPDU\
t eet h ar e shallow er t han in per m anent t eet h, and t his
ELRORJLFDOÀXLGLVSURGXFHGDWORZUDWH,QWKLVVWXG\
t he im m unological analy ses did not show differ ences
EHWZHHQ,/ǃ71)D and I L- 6 levels am ong DM and NDM children. However, a posit ive correlat ion bet ween
t hese serum biom arkers ( I L- 1b for NDM and TNF-D and I L- 6 for DM) and gingival st at us was observed. Ulker, et
al.29REVHUYHGKLJKHUOHYHOVRI,/ǃDQG71)D LQWKHJLQJLYDOÀXLGRISDWLHQWVZKRKDGJLQJLYLWLVZKHQ
com pared t o t hose wit h a healt hy periodont ium . Those
¿QGLQJVZHUHSRVLWLYHO\FRUUHODWHGZLWKSURELQJGHSWKV
and clinical at t achm ent loss. Salvi, et al.19 ( 2010)found DKLJKFRQFHQWUDWLRQRI,/ǃDQG,/LQSDWLHQWVZLWK
t y pe 1 diabet es w hen com par ed t o healt hy indiv iduals
in an ex per im ent al gingiv it is m et hod. Those aut hor s
DOVRYHUL¿HGDFRUUHODWLRQEHWZHHQWKLVLQÀDPPDWRU\
biom arker and som e bact erial species belonging t o t he
“ orange com plex ” in childr en w it h diabet es.
,QFRQFOXVLRQFOLQLFDODQGLPPXQRORJLFDOSUR¿OHV
w e r e s i m i l a r b e t w e e n D M a n d N D M c h i l d r e n .
Th e p r esen ce of Cap n ocy t op h ag a sp u t ig en a an d
Ca p n o cy t o p h a g a o ch r a ce a w a s a sso ci a t e d w i t h
gingivit is in DM children. Glycem ic and lipid param et ers
w er e higher in pat ient s w it h diabet es, but r em ained
w it h in n or m al valu es. Lon git u din al clin ical st u dies
XVLQJODUJHUSDWLHQWJURXSVDUHQHFHVVDU\WRFRQ¿UP WKHLQÀXHQFHRIGLDEHWHVRQWKHPLFURELRORJLFDODQG
im m unological param et er s and t heir r elat ionship w it h
gingiv it is in childr en.
Refer ences
1 - Al- Kh ab b az AK, Al- Sh am m ar i KF, Hasan A, Ab d u l- Rasou l M.
Per iodont al healt h of childr en w it h t y pe 1 diabet es m ellit us in Kuwait :
a case- cont r ol st udy. Med Pr inc Pract . 2013; 22( 2) : 144- 9.
2- Ashim ot o A, Chen C, Bak ker I , Slot s J. Poly m erase chain r eact ion
det ect ion of 8 put at ive per iodont al pat hogens in subgingival plaque of
gingiv it is and advanced per iodont it is lesions. Oral Micr obiol I m m unol.
1996; 11( 4) : 266- 73.
3 - Car n eir o VL, Fr aiz FC, Fer r eir a FM, Pin t ar elli TP, Oliv eir a AC,
%RJXV]HZVNL0&7KHLQÀXHQFHRIJO\FHPLFFRQWURORQWKHRUDOKHDOWKRI
children and adolescent s wit h diabet es m ellit us t ype 1. Arch Endocrinol
Met ab. 2015; 59( 6) : 535- 40.
4- Ciant ar M, Gilt hor pe MS, Hur el SJ, New m an HN, Wilson M, Sprat t
DA. Capnocytophaga spp. in periodont it is pat ient s m anifest ing diabet es
m ellit us. J Per iodont ol. 2005; 76( 2) : 194- 203.
&RQUDGV*0XWWHUV5)LVFKHU-%UDXQHU$/WWLFNHQ5/DPSHUW
F. PCR r eact ion and dot - blot hy br idizat ion t o m onit or t he dist r ibut ion
of oral pat hogens w it hin plaque sam ples of per iodont ally healt hy
indiv iduals. J Per iodont ol. 1996; 67( 10) : 994- 1003.
6- Cor t elli SC, Cor t elli JR, Aquino DR, Holzhausen M, Franco GC, Cost a
FO, et al. Clinical st at us and det ect ion of per iodont opat hogens and
Streptococcus mutans in childr en w it h high levels of supragingival
ELR¿OP%UD]2UDO5HV
7- Haffaj ee AD, Socransky SS. Microbial et iological agent s of dest ruct ive
per iodont al diseases. Per iodont ol 2000. 1994; 5: 78- 111.
8- Kim ura S, Ooshim a T, Tak iguchi M, Sasak i Y, Am ano A, Mor isak i I ,
et al. Per iodont opat hic bact er ial infect ion in childhood. J Per iodont ol.
2002; 73( 1) : 20- 6.
9- Lim LP, Tay FB, Sum CF, Thai AC. Relat ionship bet w een m ar ker s of
PHWDEROLFFRQWURODQGLQÀDPPDWLRQRQVHYHULW\RISHULRGRQWDOGLVHDVHLQ
pat ient s wit h diabet es m ellit us. J Clin Periodont ol. 2007; 34( 2) : 118- 23.
10- Loe H, Silness J. Per iodont al disease in pr egnancy: pr evalence and
sever it y. Act a Odont ol Scand. 1963; 21: 533- 1.
0DWVVRQ/*ROGEHUJ3*LQJLYDOLQÀDPPDWRU\UHDFWLRQLQFKLOGUHQ
at differ ent ages. J Clin Per iodont ol. 1985; 12( 2) : 98- 103.
0HDOH\%/5RVH/)'LDEHWHVPHOOLWXVDQGLQÀDPPDWRU\SHULRGRQWDO
diseases. Com pend Cont in Educ Dent . 2008; 29( 7) : 402- 8,410,412- 3.
1 3 - Modéer T, Won dim u B. Per iodon t al diseases in ch ildr en an d
adolescent s. Dent Clin Nor t h Am . 2000; 44( 3) : 633- 8.
14- Ok uda T, Kok ubu E, Kawana T, Sait o A, Ok uda K, I shihara K.
6\QHUJ\LQELR¿OPIRUPDWLRQEHWZHHQFusobacterium nucleatum and
Prevotella species. Anaer obe. 2012; 18( 1) : 110- 6.
2UEDN56LPVHN62UEDN=.DYUXW)&RODN07KHLQÀXHQFHRI
t y pe- 1 diabet es m ellit us on dent it ion and oral healt h in childr en and
adolescent s. Yonsei Medical J. 2008; 49( 3) : 357- 65.
16- Page RC, Kor nm an KS. The pat hogenesis of hum an per iodont it is:
an int r oduct ion. Per iodont ol 2000. 1997; 14: 9- 11.
17- Preshaw PM. Host response m odulat ion in periodont ics. Periodont ol
2000. 2008; 48: 92- 110.
18- Rot im i VO, Salako NO, Div ia M, Asfour L, Kononen E. Pr evalence
of per iodont al bact er ia in saliva of Kuwait i childr en at differ ent age
gr oups. J I nfect Public Healt h. 2010; 3( 2) : 76- 82.
19- Salv i GE, Franco LM, Braun TM, Lee A, Rut ger Per sson G, Lang
13HWDO3URLQÀDPPDWRU\ELRPDUNHUVGXULQJH[SHULPHQWDOJLQJLYLWLV
in pat ient s w it h t y pe 1 diabet es m ellit us: a pr oof- of- concept st udy. J
Clin Per iodont ol. 2010; 37( 1) : 9- 16.
2 0 - Sa k a l a u sk i e n e J, Ku b i l i u s R, Gl e i zn y s A, Vi t k a u sk i e n e A,
I vanausk iene E, Šafer is V. Relat ionship of clinical and m icr obiological
var iables in pat ient s w it h t y pe 1 diabet es m ellit us and per iodont it is.
6DUGL -& 'XTXH & &DPDUJR *$ +RÀLQJ -) *RQoDOYHV 5%
Periodont al condit ions and prevalence of put at ive periodont opat hogens
and Candida spp. in insulin- dependent t ype 2 diabet ic and non- diabet ic
pat ien t s w it h ch r on ic per iodon t it is: a pilot st u dy. Ar ch Or al Biol.
2011; 56( 10) : 1098- 105.
22- Seck in D, I lhan N, Er t ugr ul S. Gly caem ic cont r ol, m ar ker s of
endot helial cell act ivat ion and ox idat ive st r ess in childr en w it h t y pe 1
diabet es m ellit us. Diabet es Res Clin Pract . 2006; 73( 2) : 191- 7.
23- Silness J, Loe H. Per iodont al disease in pr egnancy. I I . Cor r elat ion
bet w een oral hygiene and per iodont al condit ion. Act a Odont ol Scand.
1964; 22: 121- 35.
24- Snell- Ber geon JK, West NA, Mayer- Dav is EJ, Liese AD, Mar cov ina
60'$JRVWLQR5%-UHWDO,QÀDPPDWRU\PDUNHUVDUHLQFUHDVHGLQ
yout h w it h t y pe 1 diabet es: t he SEARCH Case- Cont r ol st udy. J Clin
Endocr inol Met ab. 2010; 95( 6) : 2868- 76.
2 5 - Sb or d on e L, Ram ag lia L, Bar on e A, Ciag lia RN, I acon o VJ.
Per iodont al st at us and subgingival m icr obiot a of insulin- dependent
j u v en i l e d i a b et i cs: a 3 - y ea r l o n g i t u d i n a l st u d y. J Per i o d o n t o l .
1998; 69( 2) : 120- 8.
26- Socransky SS, Haffaj ee AD, Cugini MA, Sm it h C, Kent RL. Micr obial
com plexes in subgingival plaque. J Clin Per iodont ol. 1998; 25( 2) :
134-44.
27- Susin C, Kingm an A, Albandar JM. Effect of par t ial r ecor ding
p r ot ocols on est im at es of p r ev alen ce of p er iod on t al d isease. J
Per iodont ol. 2005; 76( 2) : 262- 7.
28- Suzuk i N, Yoshida A, Sait o T, Kawada M, Nak ano Y. Quant it at ive
m icr obiological st udy of subgingival plaque by r eal- t im e PCR show s
correlat ion bet ween levels of Tannerella forsyt hensis and Fusobacterium
spp. J Clin Micr obiol. 2004; 42( 5) : 2255- 7.
2 9 - Ulk er AE, Tu lu n oglu O, Ozm er ic N, Can M, Dem ir t as S. Th e
ev alu at ion of cy st at in C, I L- 1 bet a, an d TNF- alph a lev els in t ot al
VDOLYDDQGJLQJLYDOFUHYLFXODUÀXLGIURPWR\HDUROGFKLOGUHQ-Per iodont ol. 2008; 79( 5) : 854- 60.
30- Wat anabe K, From m el TO. Porphyromonas gingivalis, Actinobacillus
actinomycetemcomitans and Treponema denticola det ect ion in oral
plaque sam ples using t he polym erase chain react ion. J Clin Periodont ol.
1996; 23( 3 Pt 1) : 212- 9.
31- Xav ier AC, Silva I N, Cost a FO, Cor r êa DS. Per iodont al st at us
in childr en and adolescent s w it h t y pe 1 diabet es m ellit us. Ar q Bras