rev bras reumatol.2016;56(1):86–89
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
Skeletal
abnormalities
of
tricho-rhino-phalangeal
syndrome
type
I
Guilherme
Monteiro
de
Barros,
Adriana
Maria
Kakehasi
∗UniversidadeFederaldeMinasGerais,BeloHorizonte,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24April2014 Accepted26August2014 Availableonline9March2015
Keywords:
Tricho-rhino-phalangealsyndrome typeI
Jointmalformations Geneticsyndrome
a
b
s
t
r
a
c
t
Thetricho-rhino-phalangealsyndrome(TRPS)typeIisararegeneticdisorderrelatedto theTRPS1genemutationinchromosome8,characterizedbycraniofacialabnormalities and disturbances in formation and maturation of bone matrix. The hallmarks are sparseandbrittlehair,tendencytoprematurebaldness,bulbousnosecalledpear-shaped, longandflatfilterandlowearimplantation.The mostnoticeableskeletalchangesare clinodactyly,phalangealepiphysesofthehandsappearingascone-shaped,shortstature andhipjointmalformations.WereportacaseofateenagerboydiagnosedwithTRPSand referredforrheumatologicevaluationduetojointcomplaints.
©2014ElsevierEditoraLtda.Allrightsreserved.
Anormalidades
esqueléticas
da
síndrome
tricorrinofalangiana
tipo
I
Palavras-chave:
SíndrometricorrinofalangianatipoI Malformac¸õesarticulares
Síndromegenética
r
e
s
u
m
o
Asíndrometricorrinofalangiana(STRF)tipoIéumadoenc¸agenéticarara,relacionadacom amutac¸ãonogeneTRPS1docromossomo8.Écaracterizadaporanomaliascraniofaciaise distúrbiosnaformac¸ãoematurac¸ãodamatrizóssea.Ascaracterísticassãocabelosralose quebradic¸os,tendênciaàcalvícieprematura,narizbulbosoemformatodepera,filtronasal longoeplanoebaixaimplantac¸ãodasorelhas.Asalterac¸õesesqueléticasmaisnotáveis sãoaclinodactilia,asepífisesdasfalangesdasmãosemformadecone,abaixaestatura easmalformac¸õesnaarticulac¸ãodoquadril.Relata-seocasodeumadolescente diagnos-ticadocomSTRFeencaminhadoparaavaliac¸ãoreumatológicaemdecorrênciadequeixas articulares.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
∗ Correspondingauthor.
E-mail:[email protected](A.M.Kakehasi).
http://dx.doi.org/10.1016/j.rbre.2014.08.017
rev bras reumatol.2016;56(1):86–89
87
Introduction
FirstdescribedbyGiedion,thetricho-rhino-phalangeal syn-drome(TRPS)typeIisararediseasecausedbyTRPS1gene haploinsufficiency,whichislocatedinchromosome8.1This geneisrelatedtodecodingoftranscriptionfactorsinvolvedin regulationofboneperichondriummineralizationand prolif-erationandapoptosisofchondrocytes.TheTRPSisclassified intothreesubtypes:typesIandIIIhavedistinctclinical pre-sentationsaccordingtoTRPS1mutation,differingclinicallyby degreeofmalformations,2whiletypeIIhasassociatedmental retardationandboneexostosesasalandmark.3Inmostcases thesyndromeisautosomaldominantandmarkedbyshort stature,finehairandalopecia,pear-shapednose,craniofacial andskeletalmalformations,andphalangealjointdeformity. Althoughrare, individualsmay present tothe rheumatolo-gistatdifferentages,bringingdifferentialdiagnosesincluding juvenileidiopathicarthritisandLegg–Calvé–Perthesdisease. Besideschangesofthehandsandfeet,degenerationofthe hipjointmaybeaseriousconsequenceduetothepotential forearlyfunctionalimpairment.Thisgeneticdiseasepresents broadclinicalspectrumandimportantimpactonpatientand family,requiringmultidisciplinaryapproach.
Case
report
A17-year-oldboywasevaluatedwithcomplaintsofchronic paininthehipsandinterphalangealjointsofthehands.In thelast 7months,hip jointpain wasalsoobservedduring sports activities,which ledthe patient formusculoskeletal systemevaluation.Nomorningstiffnessand nosignificant inflammatorysignswerenoted.Therewasnoreportoffever orweightloss.Fiveyearsago,hismotherobservedsymmetric deformityinproximalinterphalangealjointsofhands char-acterizedbylocalswellingandinsidiousmechanicalpain.In 2009,during the investigation ofshort stature,the patient wasdiagnosedwithtricho-rhino-phalangealsyndrometype Ithroughgeneticstudy.Cognitivedevelopmentwasnormal.
Fig.1–Seventeen-year-oldboywithtricho-rhino-phalangealsyndromeshowingfinehair,longphiltrumandbulboustipof thenose(a)andhandshowingincreasedproximalinterphalangealjoints(b).
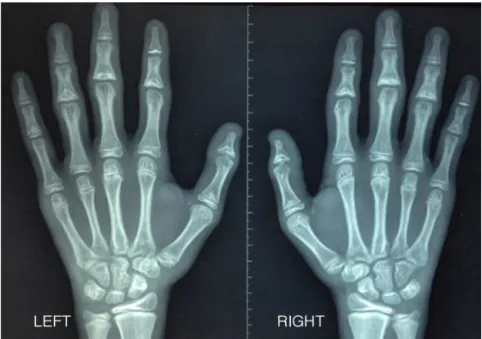
Physicalexaminationshowedtriangularfacewiththenose elongated(pear-shaped),thepresenceofmediannasolabial grooveandtaperingofthelips,thinhairandprominentjaw, prominenceoftheinterphalangealjointsofthehands,no red-nessorlocalheat(Fig.1).Therewasnopainonmanipulation and no movementlimitation inupperlimbs. Discreetgenu varus,andpainwithlimitationofmovementwereobserved inbothhipjoints.Laboratorytestswereessentiallynormal: erythrocytesedimentationratewas2mm/h,C-reactive pro-tein<6mg/L(referencevalue<8mg/L),antinuclearantibodies andrheumatoidfactornegative,creatinineandbloodcount cellswerealsonormal.Radiographyofthehandsshowedbone dimorphisminthedistalphalanxofthethumbandthemiddle phalanxoftheotherfingers,characterizedbyshorteningand wideningoftheproximalmetaphysisandproximalepiphysis triangularshape(Fig.2).Radiographyofthehipjointsshowed
coxaplanaandmildsubchondralsclerosisintherightfemoral acetabulumwithpreservedjointspace.Magneticresonance imaging(MRI)ruledoutasepticnecrosisofthehipshowing flatteningofthefemoralnecksandlabralhypertrophy. Assess-mentofbonemineraldensity(BMD)and bodycomposition bydual-energyX-rayabsorptiometry(equipmentHologic Dis-covery W)showedlowBMDinlumbarspine(Z-score−2.3)
andlimitrophebonemineralcontendvalue(Z-scoreof−2.0).
Patientandhisfamily receivedsupportaboutthediagnosis andrecommendationsforarticularstructurespreservation.
Discussion
88
rev bras reumatol.2016;56(1):86–89Fig.2–Handradiographyshowingshorteningandwideningoftheproximalmetaphysisandproximalepiphysistriangular
shape.
TypesIand IIIarethoughttoexistonacommonspectrum resultingfrommutationsoftheTRPS1gene,andare differenti-atedbythedegreeofphenotypicskeletaldeformity.Deletions spanningTRPS1andthedistaladjacentgeneEXTarefoundin TRPStypeII,andalterationsinEXTarethoughttobe respon-sibleforthe mentaldeficienciesandexostosesseeninthis form.Clinodactylydescribesabendorcurvatureofthefifth fingertowardtheadjacentfourthfingerandcanbeanisolated anomalyoritcanoccurinassociationwithgeneticsyndromes likeTRPS.Deformitieslikeirregularlyshortandstubbyhands are frequent. Similar feet involvementcan occur, but in a lesser extent. As inthis case, deformitiesof the hips and pelvissuchascoxaplana,coxamagna,orfindingsresembling Legg–Calvè–Perthesdisease,canbefound.
Historyandphysicalexaminationcansuggestthe diagno-sisespeciallybecauseofcraniofacialandhandsappearancein typicalcases.Imagingroentgenogramsofhands,pelvis,and hipcanbeusefuland,althoughconedepiphysisatthebase ofphalangesistypical,itcanbefoundinotherskeletal dys-plasiasandinalmost5%ofnormalchildrenandteenagers. AnalysisoftheTRPSand EXT genesatthe 8q24locuscan beundertakentoidentifytheresponsiblemutation.6Inthis indexpatient,therearenoreportsofrelativeswithsimilar condition,andprobablyasporadicmutationwasresponsible, asreportedbyBoothin1981.7Therearereportsofcardiacand neurologicabnormalities8butnoneofthemwerefoundinour patient.Noassociationwithautoimmunediseaseisdescribed andimmunologicallaboratorytestsareessentiallynormal.
Delayed skeletal maturation and early degeneration of the hips are alsodescribed. This case reportconfirms the mainfeaturesofthesyndromeandaddsinformationabout MR imagingand body composition byDXA. Both diagnos-tic methods are helpful tools in evaluation of phenotype characteristics, bringing more information about articular consequencesandgrowthdisturbances.Thecontributionof
MRIresidesinthepossibilityofearlyevaluationofthejoints cartilage status,allowingtheexclusionofother diseasesor complications,suchashipasepticnecrosis.
Low bone mineral density can be another pitfall in youngindividualswithtricho-rhino-phalangealsyndrome.An appropriateevaluationofbonestatusintheyouthcomprises the composite of lumbar spine mineral density and bone mineralcontendbyDXAand,giventheresultsinthiscase, strategiestominimizeunfavorable evolutioncan be imple-mented.Delayedskeletalmaturationcanalsobefollowedby DXAanditisimportanttorememberthattotalbodyand lum-barspinearethesitestobeevaluatedinindividualslessthan 20years.
One ofthe hallmarks ofthe syndrome is its wide vari-etyofclinicalpresentation,whichincludesasimplechange inthephalangestolowbonemineraldensitywithhighrisk offragilityfractures.Besidesmusculoskeletalcare,patients with tricho-rhino-phalangeal syndrome must be followed upforthedevelopmentofendocrineabnormalitiessuchas hypothyroidism,growthhormonedeficiency,andidiopathic hypoglycemia.5
ExperimentalstudieshavepermittedevaluationofTRPS1 specificroleinkidneydevelopment.NewbornmiceTRPS1−/−
have shortened long bones and incompletely formed pha-langealjoints.ItcouldrevealthatTRPS1actsintheBmp7/p38 MAPK/TRPS1 signaling pathway, responsible for mediating theinductionofmesenchymaltoepithelialtransition,which leadstoformationoftubulesandglomeruliandisessential fornormalrenaldevelopment.9
rev bras reumatol.2016;56(1):86–89
89
and,second,thissyndromecanresembleidiopathicjuvenile arthritis,Legg–Calvè–Perthes,orskeletaldysplasia.Thevalue ofearlyevaluationalsoliesinprovidingthepatientandfamily withappropriatesupportandcounselingforfamilyplanning.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. GiedionA.Dastricho-rhino-phalangealsyndrom.Helv PaediatrActa.1966;21:475–82.
2. LudeckeHJ,SchaperJ,MeineckeP,MomeniP,GroS,Von HultumD,etal.Genotypicandphenotypicspectrumin tricho-rhino-phalangealsyndrometypesIandIII.AmJHum Genet.2001;68:81–91.
3. LangerLOJr,KrassikoffN,LaxovaR,Scheer-WilliamsM, LutterLD,GorlinRJ,etal.Thetricho-rhinophalangeal
syndromewithexostoses(orLanger–Giedionsyndrome):four additionalpatientswithoutmentalretardationandreviewof theliterature.AmJMedGenet.1984;19:81–111.
4.BurgessRC.Trichorhinophalangealsyndrome.SouthMedJ. 1991;84:1268–70.
5.VaccaroM,GuarneriC,BlandinoA.Trichorhinophalangeal syndrome.JAmAcadDermatol.2005;53:858–60.
6.SayedCJ,MatheisP,MorrellDS.Hypotrichosis,bulbousnose, andcone-shapedepiphysesinan8-year-oldgirl.Pediatr Dermatol.2008;25:557–8.
7.BoothCW,MaurerWF,KayeC.Denovo9:11translocationina sporadiccaseoftrichorhinophalangeal(I)syndrome.Pediatr Res.1981;15:559.
8.RuéM,LudeckeHJ,SibonI,RichezC,TaineL,Fouber-Samier A,etal.Rheumatologicandneurologicaleventsinanelderly patientwithtricho-rhino-phalangealsyndrometypeI.EurJ MedGenet.2011;54:e405–8.
9.SunY,GuiT,ShimokadoA,MuragakiY.Theroleof tricho-rhino-phalangealsyndrome(TRPS)1inapoptosis duringembryonicdevelopmentandtumorprogression.Cells. 2013;2:496–505.