w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Effect
of
combined
treatment
with
zoledronic
acid
and
propranolol
on
mechanical
strength
in
an
rat
model
of
disuse
osteoporosis
Deepak
Kumar
Khajuria
a,b,∗,
Rema
Razdan
a,
Debiprosad
Roy
Mahapatra
baDepartmentofPharmacology,Al-AmeenCollegeofPharmacy,Bangalore,India
bLaboratoryforIntegrativeMultiscaleEngineeringMaterialsandSystems,DepartmentofAerospaceEngineering,IndianInstituteof
Science,Bangalore,India
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13May2014 Accepted28July2014
Availableonline27November2014
Keywords:
Disuseosteoporosis Ratmodel
Zoledronicacid Propranolol
a
b
s
t
r
a
c
t
Objectives: Amodelthatusesrighthind-limbunloadingofratsisusedtostudythe conse-quencesofskeletalunloadingduringvariousconditionslikespaceflightsandprolonged bedrestinelderly.Thisstudywasaimedtoinvestigatetheadditiveeffectsofantiresorptive agentzoledronicacid(ZOL),aloneandincombinationwithpropranolol(PRO)inaratmodel ofdisuseosteoporosis.
Methods:Inthepresentstudy,3-month-oldmaleWistarratshadtheirrighthind-limb immo-bilized(RHLI)for10weekstoinduceosteopenia,thenwererandomizedintofourgroups: (1) RHLIpositivecontrol,(2)RHLIplusZOL(50g/kg, i.v.singledose),(3)RHLIplusPRO (0.1mg/kg,s.c.5daysperweek),(4)RHLIplusPRO(0.1mg/kg,s.c.5daysperweek)plusZOL (50g/kg,i.v.singledose)foranother10weeks.Onegroupofnon-immobilizedratswasused asnegativecontrol.Attheendoftreatment,thefemurswereremovedandtestedforbone porosity,bonemechanicalproperties,andbonedryandashweight.
Results:With respect to improvementin the mechanicalstrength ofthe femoral mid-shaft,thecombinationtreatmentwithZOLplusPROwasmoreeffectivethanZOLorPRO monotherapy.Moreover,combinationtherapyusingZOLplusPROwasmoreeffectivein improvingdryboneweightandpreservedthecorticalboneporositybetterthan monother-apyusingZOLorPROinRHLIrats.
Conclusions: ThesedatasuggestthatthiscombinedtreatmentwithZOLplusPROshouldbe recommendedforthetreatmentofdisuseosteoporosis.
©2014ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](D.K.Khajuria).
http://dx.doi.org/10.1016/j.rbre.2014.07.007
Efeitos
da
terapia
combinada
com
ácido
zoledrônico
e
propranolol
na
resistência
mecânica
em
um
modelo
de
rato
com
osteoporose
por
desuso
Palavras-chave:
Osteoporosepordesuso Estudocomratos Ácidozoledrônico Propranolol
r
e
s
u
m
o
Objetivos: Investigarosefeitosaditivosdoagenteantirreabsorc¸ãoácidozoledrônico(ZOL), isoladoeemcombinac¸ãoaopropranolol(PRO),emummodeloderatocomosteoporosepor desuso.
Métodos: Usou-seummodelodepatatraseiradireitaderatoprivadadedescargadepeso paraestudarasconsequênciasdafaltadedescargadepesosobreoesqueletodurantevárias condic¸ões,comomissõesespaciaiserepousoprolongadonoleitoemidosos.RatosWistar machosdetrêsmesesdeidadeforamsubmetidosàimobilizac¸ãodapatatraseiradireita (IPTD)por10semanasparainduziràosteopenia;emseguida,foramdivididos aleatoria-menteemquatrogrupos:1–IPTDparacontrolepositivo;2–IPTDmaisZOL(50g/kg,dose únicaintravenosa);3–IPTDmaisPRO(0,1mg/kg,viasubcutnea,cincodiasnasemana);4 –IPTDmaisPRO(0,1mg/kg,viasubcutnea,cincodiasnasemana)maisZOL(50g/kg,dose únicaintravenosa)poroutras10semanas.Umgrupoderatosnãoimobilizadosfoiusado comocontrolenegativo.Nofimdotratamento,osfêmuresforamremovidosetestaram-se aporosidadedoossoesuaspropriedadesmecnicas,alémdopesosecoedascinzasdoosso.
Resultados: Noquedizrespeitoàmelhoriadaresistênciamecnicadadiáfisefemoralmédia, aterapiacombinadacomZOLmaisPROfoimaiseficazdoqueamonoterapiacomZOLou PRO.Alémdisso,aterapiacombinadacomZOLmaisPROfoimaiseficaznamelhoriado pesosecodoossoepreservoumelhoraporosidadedoossocorticaldoqueamonoterapia comZOLouPROemratossubmetidosàimobilizac¸ãodapatatraseiradireita.
Conclusões: EssesdadossugeremqueaterapiacombinadacomZOLmaisPROdeveser recomendadaparaotratamentodaosteoporosepordesuso.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Osteoporosisisabonedebilitatingdiseasethatcausesnearly 9millionbonefractureseachyear.1Disuse(unloading)isone
oftheimportantcauses ofosteoporosis.2 Mechanical
load-ing is essential forthe normalfunctioning of bone tissue. Immobilizationresultsinimbalanceofbonemetabolism fol-lowedbyrapidbonelossandimpairmentofbonemechanical function.3 Thisimmobilization-inducedbonelossiscaused
byanincreasedboneresorptionandadecreasedbone forma-tion.Disuse(unloading)osteoporosisoccursinpatientswith spinalcordinjuries,patientsconfinedtoprolongedbedrest, andastronautsexposedtomicrogravityduringspaceflight.2
Microgravity induced osteoporosis poses a major threat to theastronaut’shealth.Microgravityleadstotheunloadingof theskeletonespeciallyweightbearingbones.3Disuse
osteo-porosis notonlyincreases thesusceptibility tofractures in patientswithspinalcordinjuriesandelderlyrequiringbed rest,butalsothreatenssafetyandhealthofastronauts dur-ingspaceflights.Therefore,itisveryessentialtofindrelevant countermeasuresfordisuseosteoporosistoreduceorprevent suchboneloss.
Severalanimalmodelshavebeensuggestedforstudying immobilizationinducedbonelossincludingneurectomy,tail suspension, plaster casting, and elastic bandaging. In this study,righthind-limbimmobilization(RHLI)wasachievedby anewprocedurewhichwasdevelopedtoavoidtheproblems caused by mostwidely used methods for the immobiliza-tion(e.g.,plastercast,bandagingortailsuspension)ofrats.
Thesmallerweightoftheframeworkcomparedwitha plas-ter castkeptthe difficultyinmovementand locomotionto a minimum, with aconsequent minimalbody weightloss throughouttheperiodofimmobilization.Moreover,noskin ulcerationorfootswellingwasfoundintheanimalswhenthe immobilizationwasremoved.Theimmobilizationprocedure proposedwaseffectiveinproducinglong-termdisuseinthe hind-limbsofratsandisagoodalternativetothetraditional methodsofimmobilization.2
Zoledronicacid(ZOL)isathirdgenerationnitrogen con-taining bisphosphonate that binds to hydroxyapatite with the highestaffinity and inhibitsosteoclasts withthe high-estpotencyofalllicensedbisphosphonates.4,5Therefore,ZOL
needsonlytobeinjectedonceannuallyinpatients,whilestill efficientlyinhibitingosteoclasticactivityandthereby reduc-ingtheriskoffracture.6Althoughanti-resorptiveagentssuch
asbisphosphonatesareeffectiveinreducingboneloss,they arenotabletoinduceformationofanewone.5
Propranolol(PRO),anon-selective-adrenergicantagonist, is now considered to bea potential drug under investiga-tionforfracturehealingandmorespecificallyforosteoporosis therapy.Inratmodelofpostmenopausalosteoporosis treat-mentwithPROimprovesbonepropertiesbyincreasingbone formationanddecreasingboneresorption.7–10Moreover,
var-ious preclinical studies have demonstrated that treatment byPROmitigatedthebonelossinducedbyunloading.2,11,12
Furthermore, resultsofsome priorepidemiological studies confirmthehypothesisthat-blockersuseisassociatedwitha decreaseinfracturerisk.13–15Combinationtherapyisnowthe
canincreasetheeffectivenessoftreatment.Teriparatideisan analogofhumanparathyroidhormone(PTH).Itisananabolic agentthatreducestheriskoffractureinosteoporoticpatients. Combined PTH and bisphosphonate treatment resulted in more pronounced improvements of the bone architecture than either PTH or bisphosphonate treatment alone.16–18
Rodriguesetal.demonstratedthatlowdosesofPROsuppress bone resorptionby inhibiting receptor activator ofnuclear factorkappa-B ligand(RANKL)-mediated osteoclastogenesis aswellasinflammatorymarkerswithoutaffecting hemody-namicparameters.19 Thisresultissupportedbyaprevious
finding,whichshowedthatpropranololstimulates osteopro-tegerin(OPG)onitsowninosteoblastcells.20 Theabilityto
stimulateosteoblast,whilealsodampingosteoclastsmakes PROan attractiveand unique alternative to antiresorptive therapyforosteoporosis.PRO, whichcoulddirectly prevent bonelossand biomechanical alterationbyincreasing bone formationanddecreasingboneresorption,maybethenext anabolicagentforosteoporosistreatmentafterPTH.7,8,10,19,20
As immobilization induced bone loss involves both increasedboneresorptionanddecreasedboneformation,it seems to beobvious totarget the immobilization induced bonelosswithacombinedantiresorptiveandboneanabolic treatmentregimen,suchasZOLandPRO.Theeffectsofa com-binedPROandZOLtreatmenthavepreviouslybeenstudied inovariectomizedrats,7whereasthistreatmentregimenhas
notpreviouslybeeninvestigatedinimmobilization-induced osteopenia.Consequently,theaimofthepresentstudywas toinvestigate the efficacy ofa boneanabolic agent PRO, a boneantiresorptiveagentZOL,andthecombinationofthese two in the treatment of immobilization-induced osteope-niainrats.Owingtothedifferentmechanismsofactionof ZOL and PRO, ourhypothesis wasthat the combination of ZOLandPROwouldfacilitategreaterimprovementsinbone propertiesthan eitherintervention alone. Weassessedthe parametersasfollows:(1)themechanicalpropertiesin immo-bilized(right)andnon-immobilized(left)femoralmid-shaft; (2)theboneporositymeasurementoftheimmobilized(right) andnon-immobilized(left)femur;(3)measurementof immo-bilized(right)andnon-immobilized(left)dry boneand ash weight.
Materials
and
methods
Drugs,chemicalsandothermaterials
ZOLwasobtainedfromNaprod LifeSciences,Maharashtra, India.PRO,ketamine,xylazineandxylenewasobtainedfrom AurobindoPharma(Hyderabad,India),NeonPharma (Mum-bai,India),IndianImmunologicals(Hyderabad,India),andS.D. Finechemicals(Mumbai,India),respectively.
Experimentalanimals
In-house laboratorybred healthy male Wistar rats with12 weeks of age were included in the study. Animals were maintained under controlledtemperature at 25±2◦C with
12h light/darkcycle with foodand water and providedad libitum.TheexperimentswereconductedaspertheCPCSEA
(Committee forthe Purpose of Control and Supervisionof Experiments onAnimals) guidelines afterobtainingethical clearancefromtheInstitutionalAnimalEthicalCommittee.
Pre-clinicalstudydesign
At three months of age, right hind-limb of the rats were immobilizedagainsttheabdomenunderketamine(80mg/kg) andxylazine(10mg/kg)anesthesia,intraperitoneally accord-ingtoanewmethodofrighthind-limbimmobilization(RHLI) describedpreviously.2
Rats were divided into 5 groups (6 rats per group): (1) non-immobilized(negativecontrol)group; (2)RHLI(positive control)for20weeks;(3)RHLIfor10weeks,andthenRHLIplus ZOL(50g/kg,singleintravenousdose)foranother10weeks; (4) RHLI for10 weeks,and then RHLIplus PRO(0.1mg/kg, injected subcutaneously 5 days per week) for another 10 weeks;(5)RHLIfor10weeks,thenRHLIplusPRO(0.1mg/kg, injectedsubcutaneously5daysperweek)plusZOL(50g/kg, singleintravenousdose)foranother10weeks.Subcutaneous injectionsfivedaysperweekincaseofimmobilizedgroups treated with PRO and ZOL plus PRO require some animal handling andcreatesomestresstotheanimals.Therefore, non-immobilized(negativecontrol)andRHLI(positivecontrol) and RHLI plus ZOL groups were subcutaneously adminis-teredvehicle(normalsaline,5days/week)for10weeks.The medication dosages usedinthis experiment were selected frompreviousstudiesonratonratmodelofpostmenopausal osteoporosis.7Attheendoftreatmentstudy,allgroupswere
euthanizedbyanoverdoseofanesthesia.Inallrats, immo-bilized (right)and non-immobilized(left)were excised and clearedoffatandconnectivetissues.Femursweresoakedin salinesolutiongauzeandfrozenat−20◦Ctillfurtheranalysis.
Bothimmobilized(right)andnon-immobilized(left)femurs wereusedformeasurementofboneporosity,biomechanical properties,femorallength,femoraldryweightandashweight.
Finalbodyweightandfemorallength
Bodyweight(expressedingrams)wasmonitoredatthestart andtheendoftheexperiments.Femorallengthwasmeasured withaprecisioncaliper.
MeasurementofboneporositybyX-rayimaging
TherightfemursofallanimalswerescannedwithfoX-Rayzor, whichisaportable X-rayinspectionsystemequippedwith “Calculatehistogram”toolsoftware,accordingtothemethod described bypreviously.8,21 Briefly,forX-rayanalysis ofrat
femur,wholefemurwasdividedintofourequalfields,which includesdistalfemoralepiphysis(R1),femoralshaft(R2and R3)andproximalfemur(R4).
Biomechanicalbonestrengthtesting
Table1–Effectsofthedifferenttreatmentsonbodyweight.
Bodyweight
Group Pre-treatment(g) Post-treatment(g)
Normalcontrol 253.2±10.65a 320.1±13.39a
RHLIpositivecontrol 230.1±18.22 216.6±9.01
RHLI+ZOL 229.4±11.22 218.0±10.19
RHLI+PRO 222.4±11.07 217.0±10.21
RHLI+ZOL+PRO 227.4±19.88 219.6±14.14
Pre-treatmentshowsthedataonthedaypriortothestartoftreatment.Post-treatmentshowsdataonthefinaldayofthetreatment.Dataare
expressedasthemean±S.D.(n=6),evaluatedbyone-wayANOVAfollowedbyTukey’smultiplecomparisontest.
a p<0.001,comparedtoRHLI(positivecontrol)group.Allgroupsexceptnormalgroupunderwentrighthind-limbimmobilization(RHLI).
Briefly, femurswere removed from the −20◦C freezer and
rehydratedinasalinesolutionfor4hatroomtemperature. Hydratedweightoftheboneswasdeterminedusingafour decimalplacedigitalscale.Lengthoftheboneswasmeasured withcalipers. Specimenswere placedontwosupportsthat wereseparatedbyadistanceof12mmandbent until frac-turebyloweringthecrossheadpositionedatthemid-shaftat aconstantspeedof0.033mm/s.Fromtheload-displacement curve,thepeakload(N),theultimatestiffness(N/mm),andthe toughness(mJ)wereobtained.Ultimatestress(strength)and Young’smoduluswerederivedfromload-deformationcurves obtainedbyusingequationsdescribedbyKhajuriaetal.8
Measurementoffemoraldryweightandashweight
Afterconductingthree-pointbendingtest,thefemursofall animalsweredehydratedwithethanol,andfatwasremoved withdiethylether.Afterthe boneswereallowedtoair-dry, thedry boneweightwas measuredwithadigitalweighing balance.Next,thedriedfemurswereburnedtoashat900◦C
for5h,andtheirashweightwasmeasured.
Statisticalanalysis
All data were expressed as the mean±standard deviation (SD).For allthe data,comparisonsbetweendifferent treat-mentswereanalyzedbyone-wayANOVAfollowedbyTukey’s multiple comparison tests, and differences between the immobilizedsideandthenon-immobilizedsidewere com-pared with the Wilcoxon signed-rank test. In all cases, a probabilityerroroflessthan0.05wasselectedasthecriterion
forstatistical significance.Graphs weredrawn usingGraph PadPrism(version5.0forWindows).
Results
Effectofdifferenttreatmentsonbodyweightandfemoral
length
Ten weeks afterRHLI, the body weights were significantly lower for animals in the RHLI (positive control) and RHLI treatmentgroupscomparedwiththenon-immobilized nor-malgroup.Thisdifferencebecamegreaterattheendofthe experiment(RHLIforanother10weeks).However,therewere no statistically significant differences in weights observed betweenanyoftheactivetreatmentgroupsandthatofthe RHLI(positivecontrol)group(Table1).
Thelengthoftheimmobilizedfemurswasnotsignificantly differentfromthatofthenon-immobilizedfemursofthesame ratsintheRHLI(positivecontrol)groupandRHLItreatment groups(Table2).
Effectofdifferenttreatmentsonboneporosity
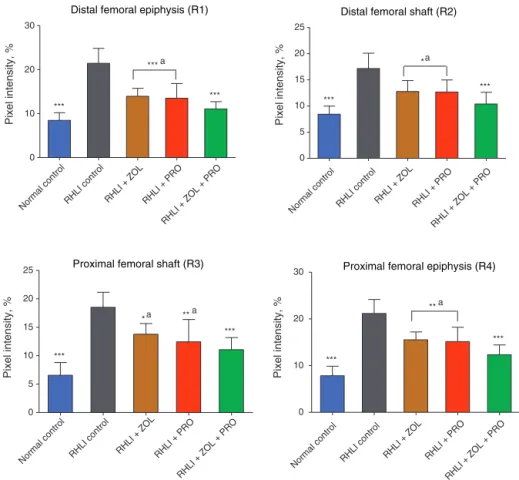
X-raytransmission intensity forthe RHLI(positive control) groupatR1,R2,R3andR4regionsofratfemoralbonewas significantlyhigherthanthoseforthenon-immobilized nor-malcontrolgroup,whichindicatesanimmobilizationelicited increaseinporosityintheseareas.
After10weeksoftherapy,allactivetreatments(singleand combined)succeededindecreasingboneporosityinRHLIrats.
Table2–Averagefemorallengthincontrolandexperimentalgroupsofrats.
Femurlength(mm)
Group Left(non-immobilized) Right(immobilized)
Normalcontrol 40.80±2.1 41.09±2.2
RHLIpositivecontrol 39.99±3.4 39.89±1.3
RHLI+ZOL 40.31±4.7 40.23±4.7
RHLI+PRO 40.23±3.3 40.14±8.7
RHLI+ZOL+PRO 40.51±7.6 40.48±2.9
Distal femoral epiphysis (R1)
Normal controlRHLI control RHLI + ZOL RHLI + PRO
RHLI + ZOL + PRO
0 10 20 30
***a
***
***
Pixel intensity, %
Proximal femoral shaft (R3)
Normal control RHLI control R HLI + ZOL
RHLI + PRO
RHLI + ZOL + PRO
0 5 10 15 20 25
***
*** **a *a
Pixel intensity, %
Proximal femoral epiphysis (R4)
Normal co
ntrol
RHLI co
ntrol
RHLI
+ ZOL
RHLI + P
RO
RHLI
+ ZOL
+ PR
O
0 10 20 30
***
***
**a
Pixel intensity, %
Distal femoral shaft (R2)
Nor mal
control
RHLI control RHLI + ZOL RHLI + PRO
RHLI + ZOL + PRO
0 5 10 15 20 25
***
*** *a
Pixel intensity, %
Fig.1–Effectofzoledronicacidandpropranolol,aloneorincombinationonfemoralporosity.Dataareshownasthe mean±SD(n=6),evaluatedbyTukey’smultiplecomparisontest.BoneporosityofR1:distalfemoralepiphysis,R2:distal
femoralshaft,R3:proximalfemoralshaft,R4:proximalfemoralepiphysis*p<0.05;**p<0.01;***p<0.001,comparedtoRHLI
(positivecontrol)group;ap<0.05,comparedtoZOLplusPROgroup.Allgroupsexceptnormalgroupunderwentright hind-limbimmobilization(RHLI).
TheX-raytransmissionintensityofZOL,PROandZOLplus PROgroups wassignificantlylower ascomparedwithRHLI (positivecontrol) groupatR1, R2,R3 and R4regions ofrat femoralbone.TheX-raytransmissionintensityofZOLplus PROgroupswassignificantlylowerthanthatoftheZOLand PROgroupatR1,R2,R3andR4 regions.Theseresults indi-catethatascomparedtomonotherapywithZOLorPRO,the combination therapywithZOL plus PROismorebeneficial forthemassofbothtrabecularandcorticalbonesthatwere decreasedbyimmobilization(Fig.1).
Effectofdifferenttreatmentsonmechanicalpropertiesin
thefemoralmid-shaft
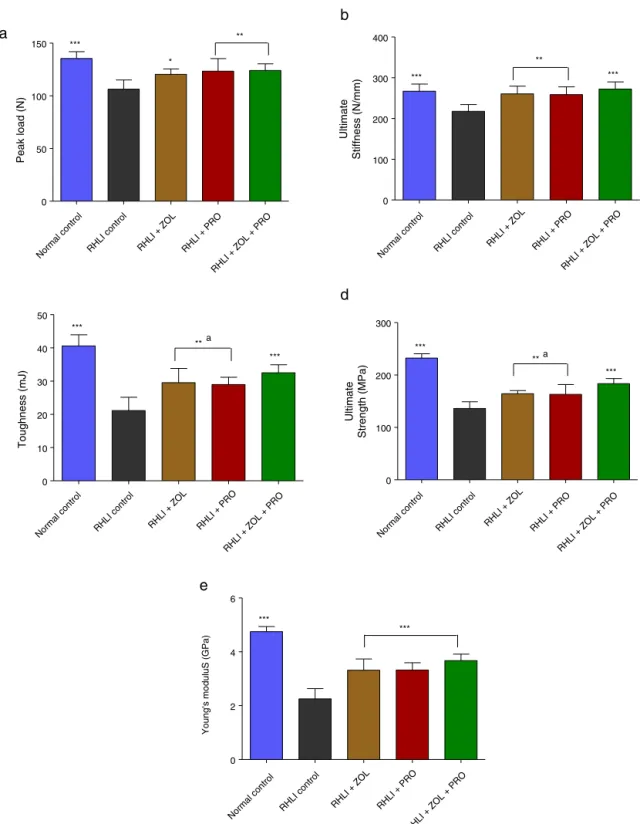
Fig.2showsthepeakload,ultimatestiffness,toughness, ulti-matestrengthandYoung’smodulusinthefemoralmid-shaft, respectively.Three-pointbendingtestsoftherightfemur indi-cated that RHLI (positive control) group caused significant reductionsin the peak load,ultimate stiffness, toughness, ultimatestrengthandYoung’smoduluscomparedwiththose innon-immobilizednormalgroup.IntheZOL,PROandZOL plus PROgroups, the peak load, ultimate stiffness, tough-ness,ultimatestrengthandYoung’smodulusofthefemurwas
significantlyhigherthanintheRHLI(positivecontrol)group.In ZOLandPROgroups,theultimatestrengthandYoung’s mod-ulus wassignificantlylowerthan thatinthe ZOLplusPRO group.
Comparisonbetweennon-immobilized(left)legand
immobilized(right)legwithinasamegroup
RHLIinducedasignificantdecreaseindryandashweights in RHLI (positive control) rat femurs compared to non-immobilizednormalcontrol rats(Table3). IntheRHLI rats treatedwithallactivetreatments(singleandcombined),dry andashweightsweresignificantlyheavierthanthoseinthe RHLI (positive control) group. The RHLI femur of the rats treatedwithZOLplusPRO,thedryandashweightwas sig-nificantly heavierthanthoseinZOLorPROtreatedgroups. Intheleftnon-immobilizedfemurs,nosignificantdifference was observed between RHLI (positive control) group, non-immobilizednormalgroupandallactivetreatments(single andcombined)groups.
Normal control RHLI control RHLI + ZOL RHLI + PRO RHLI + ZOL + PRO 0
50 100 150 ***
*
**
Peak load (N)
a
Normal control
RHLI control RHLI + ZOL RHLI + PRO
RHLI + ZOL + PRO
0 100 200 300 400
*** ***
**
Ultimate
Stiffness (N/mm)
b
e
d
Norma l control
RHLI control RHLI + ZOL RHLI + PRO
RHLI + ZOL + P RO 0
10 20 30 40 50
***
*** **a
Toughness (mJ)
c
Norm al control
RHLI contr ol
RHLI + Z OL
RHLI + PRO
RHLI + ZOL + PRO 0
100 200 300
***
**a
***
Ultimate
Strength (MPa)
Normal control RHLI control
RHLI + ZOL RHLI + PRO
RHLI + ZOL + PR O
0 2 4 6
*** ***
Young's moduluS (GPa)
Fig.2–Effectsofzoledronicacid,propranolol,orzoledronicacidpluspropranololonthemechanicalstrengthofthefemoral diaphysis.Thediaphysiswassubjectedtothree-pointbendingtofailure,whichprovideddataonpeakload(a),ultimate stiffness(b),toughness(c),ultimatestrength(d),andYoung’smodulus(e).Dataareshownasthemean±SD(n=6),
evaluatedbyTukey’smultiplecomparisontest.*p<0.05;**p<0.01;***p<0.001,comparedtoRHLI(positivecontrol)group;
Distal femoral epiphysis (R1)
0 10 20 30
Normal control RHLI control RHLI + ZOL RHLI + PRO RHLI + ZOL + PRO ***
* *
Pixel intensity (%)
Proximal femoral shaft (R3)
0 5 10 15 20 25
Normal co ntrol
RHLI co ntrol
RHLI + ZOLRHLI + PRO
RHLI + ZOL + PRO ***
* *
Pixel intensity (%)
Proximal femoral epiphysis (R4) Distal femoral shaft (R2)
0 5 10 15 20 25
Normal controlRHLI control RHLI + ZOLRHLI + PR O
RHLI + ZOL + PRO ***
* *
Pixel intensity (%)
0 10 20 30
Norma l control
RHL I contr
ol
RHLI + ZOLRHLI + PRO
RHLI + ZOL + PRO
***
* *
Pixel intensity (%)
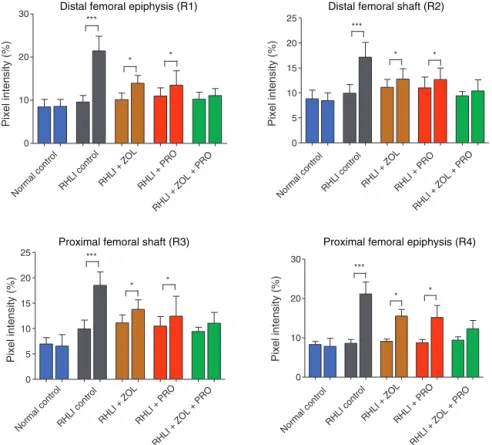
Fig.3–Femoralporosityforthenon-immobilized(leftbar)andtheimmobilized(rightbar)sidewithinthesamegroup. Asteriskdenotessignificantdifferencebetweenthenon-immobilizedsideandtheimmobilizedside(mean±SD).Allgroups exceptnormalcontrolgroupunderwentrighthind-limbimmobilization(RHLI).
significant differencebetweenthe left and right legwithin thesamegroup.AtR1,R2,R3andR4regionsofratfemoral bone,the X-raytransmission intensityforthe immobilized side(right)seemedsignificantlyhigherthanthosefromthe non-immobilized side (left) in the RHLI (positive control) group.
Similarly, atR1,R2,R3 and R4 regions, the X-ray trans-mission intensity for the immobilized side (right) seemed significantlyhigherthanthosefromthenon-immobilizedside (left)intheimmobilizedgroupstreatedwithZOLorPRO.In contrast,theRHLIgrouptreatedwithZOLplusPROshowed fullprotectionagainstdisuseosteoporosisatR1,R2,R3and
Table3–Effectofimmobilizationanddifferenttreatmentsondryboneandashweight.
Leftnon-immobilizedfemur Rightimmobilizedfemur
Group Dryboneweight
(mg/bone)
Boneashweight
(mg/bone)
Dryboneweight
(mg/bone)a
Boneashweight
(mg/bone)b
Normalcontrol 630.7±8.1 381.4±7.7 639.8±12.2c 385.7±9.4c
RHLIpositivecontrol 620.5±10.9 368.9±4.3 543.9±15.5 321.5±11.5
RHLI+ZOL 622.1±18.1 379.1±7.2 593.7±13.7c,d 351.7±9.8b,d
RHLI+PRO 619.3±12.5 372.9±8.5 592.4±12.3c,d 346.1±12.3b,d
RHLI+ZOL+PRO 638.2±9.2 388.9±15.6 617.9±15.5c 365.6±6.2e
Dataareexpressedasthemean±S.D.(n=6),evaluatedbyone-wayANOVAfollowedbyTukey’smultiplecomparisontest.
a Indicates,fortheparameter,asignificantdifferenceoftheactivetreatmentsbetweenthetwolegs.
b p<0.05.
c p<0.001,comparedtoRHLI(positivecontrol)group;
d p<0.05comparedtoZOLplusPROgroup.Allgroupsexceptnormalgroupunderwentrighthind-limbimmobilization(RHLI).
0 50 100 150 200
Normal control RHLI control RHLI + ZOL RHLI + PRO
RHLI + ZOL + PRO
*** * *
Peak load (N)
a
0 100 200 300 400
Nor
mal control RHLI control RHLI + ZOL RHLI + PRO
RHLI + ZOL 50 + PRO
*** * *
Ultimate
Stiffness (N/mm)
b
0 10 20 30 40 50
Normal control RHLI control
RHLI + ZOL RHLI + PRO
RHLI + ZOL 50 + PRO ***
** **
Toughness (mJ)
c
0 100 200 300
Normal cont
rol
RHLI co ntrol
RHL I + ZOL
RHLI + PRO
RHL I + ZO
L 50 + PRO
*** ** **
Ultimate
Strength (MPa)
d
0 2 4 6
Normal control RHLI control RHLI + ZOL RHL I + PRO
RHL I + ZOL
+ PR O
*** ** **
Young's moduluS
(GPa)
e
R4regions,asindicatedbyX-raytransmissionintensityvalues (Fig.3).
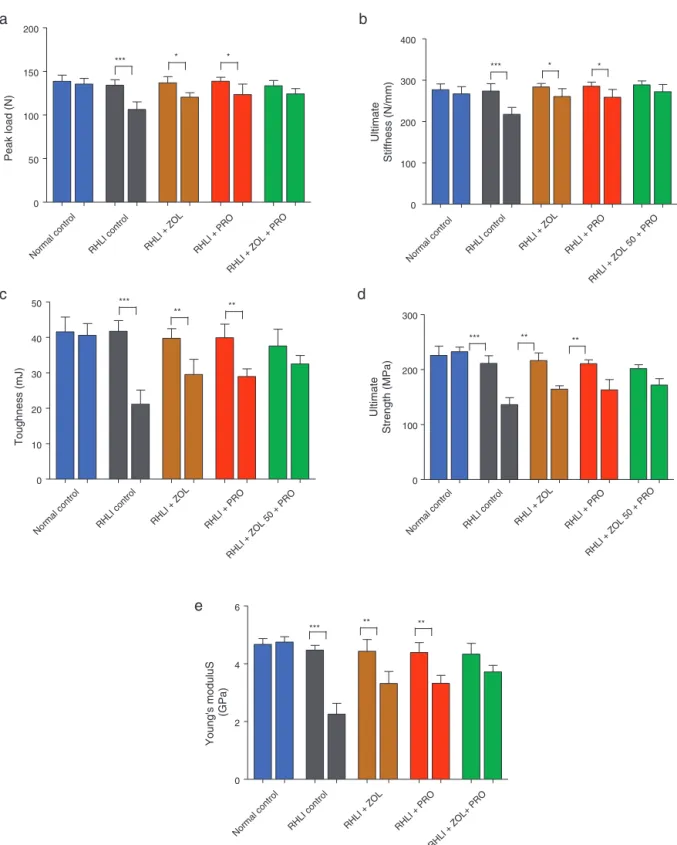
Atthe femoralmid-diaphysis(three-point bendingtest), the effect ofimmobilization was very pronouncedin RHLI (positive control) group; that is, the immobilized side (right)hadsignificantlylowervaluesofstrengthparameters including peakload,ultimate stiffness,fracture toughness, ultimate strength and Young’s modulus than the non-immobilizedside(left).Similarly,intheRHLIgroupstreated with ZOL or PRO, the immobilized side (right) had sig-nificantly lower values of strength parameters, including peak load, ultimate stiffness, fracture toughness, ultimate strength and Young’s modulus than the non-immobilized side (left). In contrast, the RHLI group treated with ZOL plus PRO showed full protection against immobilization (Fig.4).
Discussion
Thisstudy wasaimed atclinicalapplication ofthe combi-nation therapywith ZOL plusPRO asacurative treatment ofestablisheddisuseosteoporosis.Duetothedifficultyand highcostofconductingexperimentsduringaspaceflighton astronauts,anumberofinvivoground-basedexperimental modelshavebeenestablishedbyresearcherstosimulatethe conditionsexperiencedduringaspacemission.Thepresent study showedthat PROand ZOL monotherapywas able to counteract the bone loss in a rat model of disuse osteo-porosis. Furthermore,this study showed that combination therapywithZOLplusPROhadatherapeuticadvantageover ZOLorPROmonotherapyfortreatmentofdisuse osteoporo-sis.
Body weight in the normal group was greater than in the RHLI(positivecontrol) group. Thismay havebeen due tothe anesthesiaadministered duringthe RHLIprocedure. Reducedeatingandoverallreduced mobilityare other pos-siblefactors that may havecontributed in aminorway to the developmentoflower body weightand bone loss. Ear-lier studies haveshown asimilar decrease in body weight afterRHLI.2,22,23Thelengthofthefemuroftheimmobilized
limbwas not significantlydifferent from that of the non-immobilizedintact femur ofthe same rat, suggestingthat thelongitudinalgrowthoftheboneisnotretardedinthese animals.Itisthereforemorelikelythatweareheredealing withimmobilizationosteoporosisratherthansimplegrowth retardation.
TheincreaseintheboneporosityatR1,R2,R3,R4regions of rat femoral bone, due to unloading of right hind-limb was suppressed by all active treatments (single and com-bined). Moreover, the bone porosity of the ZOL plus PRO groupatR1,R2,R3andR4 regionsofratfemoralbonewas significantlylower than that ofthe ZOL or PRO monother-apy.ThisindicatesthatcombinationtherapywithZOLplus PROthickensandstrengthenscorticalbone.Itisinteresting that,inanimalstreatedwithsingleand combinedtherapy, dry and ash weights inthe right immobilizedfemur were significantly greater than those of the RHLI (positive con-trol)group.Moreover,intheanimalstreatedwithcombined therapyofZOL plus PRO,dry and ashweightsin theright
immobilizedfemurwere significantlygreaterthan thoseof theZOLorPROgroups.Theseresultsshowedthatthe com-binedtreatmentwithZOLplusPROisbeneficialforincreasing the massof rat femoral bones that was decreased due to RHLI.
Mechanical load iscrucial forthe maintenanceofbone strength.Thebonestrengthisdeterminedbythebonemass and the intrinsic properties ofthe bone material. Physical inactivity duetospinalcordinjuries,prolonged bedrestin elderlyandastronautsexposedtomicrogravityduringspace flightwouldacceleratethebonemicroarchitecture deteriora-tionanddemineralization.2,7CombinationtherapywithZOL
plusPROwasstatisticallysuperiortomonotherapywithZOL andPROatincreasingfemoralmid-shafttoughnessand ulti-matestrength.Thecurrentdatacorrelatewithfindingsfrom ourpreviousstudies,demonstratingeffectsofZOLplusPROon themechanicalpropertiesofovariectomizedratbone.7
There-fore,itisofhighpossibilitythatcombinationtherapywithZOL plus PRO is capable oftreating/preventing weightlessness-inducedboneloss.
Thisstudyhasseverallimitations.Itshouldbenotedthat extrapolationtohumansofthedatafromratstudiesshould beundertakenwithcautionbecause(1)ratsarequadrupeds, andthereforeexperienceadifferentloadingpatternfromthat ofhumans;and(2)theremodelingpatterninratsisdifferent from thatofhumans.However,theadvantageofusingthis preclinicalratmodelisthatitallowsassessmentnotonlyof boneturnoverandbonemass,butalsoofbonemechanical properties.
Comparisonmadebetweennon-immobilized(left)legand immobilized (right) leg within a same group showed that bonepropertieswere improvedbyall therapeutic interven-tions,butthemarkedosteopeniainducedbyRHLIwerenot completelycorrectedwithsingletreatmentslikeZOLorPRO alone. In contrast,combinedtreatment withZOL plusPRO showedfullprotectionagainstdisuseosteoporosis, suggest-ingthatthecombinationtherapyhasatherapeuticadvantage overeachmonotherapyforthetreatmentofdisuse osteoporo-sis.
With regardtothe clinical situation and theknowledge gainedfromtheaforementionedstudiesconcerning immobi-lizationandfromthepresentstudy,itwouldseemadvisable toshorten immobilization periodsasmuchaspossible24,25
and perhapstoconsidertheuse ofcombinationtherapyof ZOLplusPROasprotectionagainstlossofbonedensityand strength even duringshort-termimmobilization. Moreover, the combined therapy with ZOL plus PROmay prevent or reducetheriskofatrialfibrillation,oneoftheseriousadverse drugreactionsofZOL.7Inotherclinicalsituationswithvery
long-termimmobilization(paraplegiaortetraplegia,bothafter spinalcordlesions,orhemiplegiaaftercerebrovascular acci-dent,longtermspacetravel)preventivetreatmentwithZOL plusPROmayalsoberecommendedbasedonfindingsofthe presentpreclinicalstudy.
Conclusions
inhibitoryeffectofimmobilizationonboneformation.This study firstly demonstrates that combination therapy with ZOL plus PRO therapy is highlyeffective in improving the bonepropertiesinananimalmodelofdisuseosteoporosis, suggestingthat thecombination therapyhas atherapeutic advantageoverZOLorPROmonotherapyfortheprevention and treatmentofdisuseosteoporosisinduced by mechani-calinactivity.Thefindingsareconsistentwiththeeffectsof ZOLplusPROonestrogendeficiency-inducedbonelossand extendour knowledgeregardingthe effectsofthistherapy inimmobilization-inducedboneloss.Assuch,thiscombined regimenmaybeofinterestforfurtherevaluationinclinical studies.Moreover,PROmightbeanewpotentialboneanabolic agent forprevention/treatment of osteoporosis, and it can beusedeitheraloneorinconjunctionwithbisphosphonate drugs.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
AuthorswouldwholeheartedlythankProf.B.G.Shivananda, Principal,Al-AmeenCollegeofPharmacyforhiskindsupport andencouragementtocarryoutthisproject.Theauthorsare thankful toMr. B.K Jain,Naprod Life Sciences, Maharash-tra,India forprovidinggiftsampleofZoledronic acid.The authorsalsogratefullyacknowledgethecontributionofMr. VijayKumarandMr.ManishKumarPriydarshifrom Depart-mentofAerospaceEngineering,IndianInstituteofScience, incarrying out the X-rayimagingand threepoint-bending tests.
r
e
f
e
r
e
n
c
e
s
1. JohnellO,KanisJA.Anestimateoftheworldwideprevalence anddisabilityassociatedwithosteoporoticfractures. OsteoporosInt.2006;17:1726–33.
2. KhajuriaDK,DishaC,RazdanR,MahapatraDR,VasireddiR. Prophylacticeffectsofpropranololversusstandardtherapy onanewmodelofdisuseosteoporosisinrats.SciPharm. 2014;82:357–74.
3. LiCR,ZhangGW,NiuYB,PanYL,ZhaiYK,MeiQB.
AntiosteoporosiseffectofRadixScutellariaeextractondensity andmicrostructureoflongbonesintail-suspended
Sprague-Dawleyrats.Evid-BasedComplementAlternMed. 2013;2013:753703.
4. RussellRGG,WattsNB,EbetinoFH,RogersMJ.Mechanismsof actionofbisphosphonates:similaritiesanddifferencesand theirpotentialinfluenceonclinicalefficacy.OsteoporosInt. 2008;19:733–59.
5. KhajuriaDK,RazdanR,MahapatraDR.Drugsforthe managementofosteoporosis:areview.RevBrasReumatol. 2011;51:365–82.
6. BlackDM,DelmasPD,EastellR,ReidIR,BoonenS,CauleyJA, etal.Once-yearlyzoledronicacidfortreatmentof
postmenopausalosteoporosis.NEnglJMed. 2007;356:1809–22.
7.KhajuriaDK,RazdanR,MahapatraDR.Thecombination therapywithzoledronicacidandpropranololimprovesthe trabecularmicroarchitectureandmechanicalpropertyinan ratmodelofpostmenopausalosteoporosis.JOsteoporos. 2014;2014:586431.
8.KhajuriaDK,RazdanR,MahapatraDR,BhatMR.
Osteoprotectiveeffectofpropranololinovariectomizedrats: acomparisonwithzoledronicacidandalfacalcidol.JOrthop Sci.2013;18:832–42.
9.KhajuriaDK,DishaC,RazdanR,MahapatraDR.Comparative evaluationofzoledronicacid,alfacalcidol,andpropranololin pharmacologicalcorrectionofexperimentalosteoporosis.Lat AmJPharm.2013;32:968–76.
10.BonnetN,BenhamouCL,MalavalL,GoncalvesC,VicoL,Eder V,etal.Lowdosebeta-blockerpreventsovariectomy-induced bonelossinratswithoutaffectingheartfunctions.JCell Physiol.2008;217:819–27.
11.LevasseurR,SabatierJP,Potrel-BurgotC,LecoqB,CreveuilC, MarcelliC.Sympatheticnervoussystemastransmitterof mechanicalloadinginbone.JointBoneSpine.2003;70: 515–9.
12.KondoH,NifujiA,TakedaS,EzuraY,RittlingSR,DenhardtDT, etal.Unloadinginducesosteoblasticcellsuppressionand osteoclasticcellactivationtoleadtobonelossvia sympatheticnervoussystem.JBiolChem. 2005;280:30192–200.
13.BonnetN,GadoisC,McCloskeyE,LemineurG,LespessaillesE, CourteixD,etal.Protectiveeffectofb-blockersin
postmenopausalwomen:influenceonfractures,bone density,microandmacroarchitecture.Bone.2007;40: 1209–16.
14.deVriesF,SouvereinPC,CooperC,LeufkensHG,vanStaaTP. Useofb-blockersandtheriskofhip/femurfractureinthe UnitedKingdomandTheNetherlands.CalcifTissueInt. 2007;80:69–75.
15.MeisingerC,HeierM,LangO,DöringA.Beta-blockeruseand riskoffracturesinmenandwomenfromthegeneral population:theMONICA/KORAAugsburgcohortstudy. OsteoporosInt.2007;18:1189–95.
16.JohnstonS,AndrewsS,ShenV,CosmanF,LindsayR, DempsterDW,etal.Theeffectsofcombinationof
alendronateandhumanparathyroidhormone(1-34)onbone strengtharesynergisticinthelumbarvertebraandadditive inthefemurofC57BL/6Jmice.Endocrinology.2007;148: 4466–74.
17.YangX,ChanYH,MuthukumaranP,DasdeS,TeohSH,LeeT. IbandronatedoesnotreducetheanaboliceffectsofPTHin ovariectomizedrattibiae:amicroarchitecturaland mechanicalstudy.Bone.2011;48:1154–63.
18.CampbellGM,BernhardtR,ScharnweberD,BoydSK.The bonearchitectureisenhancedwithcombinedPTHand alendronatetreatmentcomparedtomonotherapywhile maintainingthestateofsurfacemineralizationintheOVX rat.Bone.2011;49:225–32.
19.RodriguesWF,MadeiraMF,daSilvaTA,Clemente-Napimoga JT,MiguelCB,Dias-da-SilvaVJ,etal.Lowdoseofpropranolol down-modulatesboneresorptionbyinhibitinginflammation andosteoclastdifferentiation.BrJPharmacol.
2012;165:2140–51.
20.HuangHH,BrennanTC,MuirMM,MasonRS.Functional alpha1-andbeta2-adrenergicreceptorsinhuman osteoblasts.JCellPhysiol.2009;220:267–75.
22.MosekildeL,ThomsenJS,MackeyMS,PhippsRJ.Treatment withrisedronateoralendronatepreventshind-limb immobilization-inducedlossofbonedensityandstrengthin adultfemalerats.Bone.2000;27:639–45.
23.TrebaczH.Disuse-induceddeteriorationofbonestrengthis notstoppedafterfreeremobilizationinyoungadultrats.J Biomech.2001;34:1631–6.
24.KannusP,JarvinenM,SievanenH,JarvinenTAH,OjaP,VuoriI. Reducedbonemineraldensityinmenwithapreviousfemur fracture.JBoneMinerRes.1994;9:1729–36.