w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Additive
effect
of
zoledronic
acid
and
alfacalcidol
in
the
treatment
of
disuse
osteoporosis
in
rats
Deepak
Kumar
Khajuria
a,b,∗,
Choudhary
Disha
a,
Rema
Razdan
a,
D.
Roy
Mahapatra
b aDepartmentofPharmacology,Al-AmeenCollegeofPharmacy,Bangalore,IndiabLaboratoryforIntegrativeMultiscaleEngineeringMaterialsandSystems,DepartmentofAerospaceEngineering,IndianInstituteof Science,Bangalore,India
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received1May2014 Accepted17August2014
Availableonline27November2014
Keywords:
Disuseosteoporosis Ratmodel
Zoledronicacid Alfacalcidol
a
b
s
t
r
a
c
t
Objectives:Disusebybedrest,limbimmobilizationorspaceflightcausesrapidboneloss.We conductedthepresentstudytoinvestigatethetherapeuticeffectsofzoledronicacid(ZOL), aloneandincombinationwithalfacalcidol(ALF)inaratmodelofdisuseosteoporosis. Methods:Inthepresentstudy,3-month-oldmaleWistarratshadtheirrighthind-limb immo-bilized(RHLI)for10weekstoinduceosteopenia,thenweredividedintofourgroups:1–RHLI positivecontrol;2–RHLIplusZOL(50g/kg,i.v.singledose);3–RHLIplusALF(0.5g/kg,
oralgaugedaily);4–RHLIplusALF(0.5g/kg,oralgaugedaily)plusZOL(50g/kg,i.v.single
dose)foranother10weeks.Onegroupofnon-immobilizedratswasusedasnegative con-trol.Attheendofthetreatment,thefemurswereremovedandtestedforboneporosity, bonemechanicalproperties,andbonedryandashweight.
Results:CombinationtherapywithZOLplusALFwasmoreeffectiveindecreasingbone porositythaneachdrugadministeredasmonotherapyinRHLIrats.Withrespectto improve-mentinthemechanicalstrengthofthefemoralmid-shaft,thecombinationtreatmentof ZOLplusALFwasmoreeffectivethaneachdrugadministeredasamonotherapy.Moreover, combinationtherapyusingZOLplusALFwasmoreeffectiveinimprovingdryboneandash weight,thansingle-drugtherapyusingZOLorALFinRHLIrats.
Conclusions:ThesedatasuggestthatcombinationtherapywithZOLplusALFrepresentsa potentiallyusefultherapeuticoptionforthetreatmentofdisuseosteoporosis.
©2014ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](D.K.Khajuria).
http://dx.doi.org/10.1016/j.rbre.2014.08.006
Efeito
combinado
do
ácido
zoledrônico
e
do
alfacalcidol
no
tratamento
da
osteoporose
por
desuso
em
ratos
Palavras-chave:
Osteoporosepordesuso Estudocomratos Ácidozoledrônico Alfacalcidol
r
e
s
u
m
o
Objetivos: Odesusopelorepousonoleito,pelaimobilizac¸ãodemembrosoupormissões espaciaisprovocaaperdaóssearápida.Fez-seesteestudoparainvestigarosefeitos ter-apêuticosdoácidozoledrônico(ZOL),isoladamenteeemcombinac¸ãoaoalfacalcidol(ALF), emummodeloderatocomosteoporosepordesuso.
Métodos: RatosWistarmachosdetrêsmesesforamsubmetidosàimobilizac¸ãoda pata traseiradireita(IPTD)por10semanasparainduziraosteopenia;emseguida,foram divi-didosemquatrogrupos:1–IPTDparacontrolepositivo;2–IPTDmaisZOL(50g/kg,dose
únicaintravenosa);3–IPTDmaisALF(0,5g/kg,viaoraldiariamente);4–IPTDmaisALF
(0,5g/kg,viaoraldiariamente)maisZOL(50g/kg,doseúnicaintravenosa)poroutras10
semanas.Umgrupoderatosnãoimobilizadosfoiusadocomocontrolenegativo.Nofim dotratamento,osfêmuresforamremovidosetestaram-seaporosidadedoossoesuas propriedadesmecânicas,alémdopesosecoedascinzasdoosso.
Resultados: AterapiacombinadacomZOLmaisALFfoimaiseficazemreduzira porosi-dadedoossodoqueamonoterapiacomumdosfármacosadministradoisoladamenteem ratossubmetidosàIPTD.Noquedizrespeitoàmelhoriadaresistênciamecânicada diá-fisefemoralmédia,otratamentocombinadocomZOLmaisALFfoimaiseficazdoquea monoterapiacomumdosfármacosadministradoisoladamente.Alémdisso,aterapia com-binadacomZOLmaisALFfoimaiseficaznamelhoriadopesosecoedascinzasdoossodo queamonoterapiacomZOLouALFemratossubmetidosàIPTD.
Conclusões: EssesdadossugeremqueaterapiacombinadacomZOLmaisALFrepresenta umaopc¸ãoterapêuticapotencialmenteútilparaotratamentodaosteoporosepordesuso.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Mechanicalloading isessential forthe normalfunctioning ofbonetissue.1Maintenanceofskeletalintegrity,bonemass andboneformationinweight-bearinglimbsaredependent on gravity.2 Skeletal unloading induced by prolonged cast or splint fixation, stress protectionsecondary to plate fix-ation of fractures, incapacitation due to chronic illness or spinalcordinjury,orweightlessnessassociatedwithorbital spaceflightcausesadecreaseinbonemassinbothhuman andanimal models.2,3 Immobilization(disuse)osteoporosis causes net bone lossas aresult ofan imbalance between bone resorption and bone formation.3 Hence, we have to keepinmindthat bonelossduetoprolonged immobiliza-tionincreasesthesusceptibilitytofracturesinpatientswith spinalcordinjuries,elderlyrequiringbedrestandastronauts duringlongspacemissions.Therefore,itisveryessentialto selectoptimaltreatmentforeffectivemanagementofdisuse osteoporosis.
Bisphosphonatesinhibitboneresorptionastheyare selec-tively incorporated into osteoclasts and interfere with the resorptiveactionofosteoclasts.4 Zoledronicacid (ZOL)is a thirdgenerationnitrogencontainingbisphosphonate,andis widelyusedforpostmenopausalandglucocorticoid-induced osteoporosisinhumans.5–8Theeffectofasingletreatmentof ZOLforimmobilization-inducedosteoporosishasbeenshown inanimalstudies.9,10Althoughanti-resorptiveagentssuchas bisphosphonatesareeffectiveinreducingboneloss,theyare notabletoinduceformationofanewbone.7,10
Alfacalcidol(1alpha-hydroxyVitaminD3–ALF)isa syn-theticVitaminDanalog,acalciumregulatinghormone,andis frequentlyusedinseveralcountriestotreatosteoporosis.9,11 ALFreducesparathyroidhormonelevels,asaresultofboth increasedcalciumabsorptionandaninhibitionofthe prolifer-ationoftheparathyroidgland,andalsodecreasestherelease ofpro-inflammatorycytokines,whichcontributetoosteoclast activation.Moreover,ALFstimulatestheformationandaction ofosteoblasts,leadingtoincreasedboneformation.12–15Ithas beendemonstratedpreviouslythattheadministrationofALF diminishedtheeffectofimmobilizationinthedevelopment ofosteoporosis.9,16
agentZOL,and the combinationofthese twointhe treat-ment ofimmobilization-induced osteopenia inrats. Owing tothedifferent mechanismsofactionofZOL andALF, our hypothesiswasthatthecombinationofZOLandALFwould facilitategreaterimprovementsinbonepropertiesthaneither interventionalone.Weassessedtheparametersasfollows; (1)themechanicalpropertiesinimmobilized(right)and non-immobilized(left) femoral mid-shaft; (2) the bone porosity measurementoftheimmobilized(right)andnon-immobilized (left)femur;(3)measurementofimmobilized(right)and non-immobilized(left)dryboneandashweight.
Materials
and
methods
Drugs,chemicalsandothermaterials
ZOL and ALF were obtained from Naprod Life Sciences (Maharashtra, India)and GlaxoSmithKline Pharmaceuticals (Mumbai,India),respectively.Ketamine,xylazineandxylene were obtained from Neon Pharma(Mumbai, India), Indian Immunologicals(Hyderabad,India),andS.D.Finechemicals (Mumbai,India),respectively.
Experimentalanimals
Twelve-week-oldmale Wistarrats weighing170–180gwere includedinthestudy.Animalsweremaintainedunder con-trolledtemperatureat25±2◦Cwith12hlight/darkcyclewith
food and waterand providedad libitum.The experiments wereconductedaspertheCPCSEA(CommitteeforthePurpose ofControlandSupervisionofExperimentsonAnimals) guide-linesafterobtainingethicalclearancefromtheInstitutional AnimalEthicalCommittee.
Pre-clinicalstudydesign
Atthreemonthsofage,righthind-limboftheratswere immo-bilizedagainsttheabdomenunderketamine(80mg/kg)and xylazine(10mg/kg)anesthesia,intraperitoneallyaccordingto anewmethodofhind-limbimmobilizationdescribedby Kha-juriaetal.9
Rats were divided into 5 groups (6 rats per group). 1– non-immobilized(negativecontrol)group;2–RHLI(positive control)for20weeks;3–RHLIfor10weeks,andthenRHLIplus ZOL(50g/kg,singleintravenousdose)foranother10weeks;
4–RHLIfor10weeks,andthenRHLIplusALF(0.5g/kg,oral
gaugedaily)foranother10weeks;5–RHLIfor10weeks,then RHLIplusALF(0.5g/kg,oralgaugedaily)plusZOL(50g/kg,
singleintravenousdose)foranother10weeks.Oralgaugedaily incaseofRHLIgroupstreatedwithALF andZOL plusALF requiredsomeanimalhandling andcreated somestressto the animals. Therefore, non-immobilized(negative control) andRHLI(positivecontrol) andRHLIplusZOL groupswere orallyadministeredvehicle(normalsaline)for10weeks.All RHLIrats were singlehoused inpolypropylene cages (size: 421mm×290mm×190mmwithgapof7mmbetweenwires) duringtheexperimentalperiod.Themedicationdosagesused in this experiment were selected from our previous study conductedonrat modelofpostmenopausalosteoporosis.17
Atthe end oftreatmentstudy, allgroups were euthanized byanoverdoseofanesthesia.Inallrats,immobilized(right) and non-immobilized(left)were excisedand clearedoffat andconnectivetissues.Femursweresoakedinsalinesolution gauzeandfrozenat−20◦Ctillfurtheranalysis.Both
immo-bilized(right)andnon-immobilized(left)femurswereused formeasurementofboneporosity,biomechanicalproperties, femorallength,femoraldryandashweight.
Finalbodyweightandfemorallength
Bodyweight(expressedingrams)wasmonitoredatthestart andtheendoftheexperiments.Femorallengthwasmeasured withaprecisioncaliper.
MeasurementofboneporositybyX-rayimaging
TherightfemursofallanimalswerescannedwithfoX-Rayzor, which isaportable X-rayinspectionsystemequippedwith “Calculatehistogram”toolsoftware,accordingtothemethod describedpreviously.22Briefly,forX-rayanalysisofratfemur, wholefemurwasdividedintofourequalfields,whichincluded distalfemoralepiphysis(R1),femoralshaft(R2andR3)and proximalfemur(R4).
Biomechanicalbonestrengthtesting
The mechanical properties of the femoral mid-shaft were measuredusingthree-pointbending,usingauniversal test-ingmachine(BISSMakron,Bangalore,India).Femurstrength wasassessedbythreepointbendingaspreviouslydescribed.22 Briefly, femurswere removed from the −20◦ C freezer and
rehydratedinasalinesolutionfor4hatroomtemperature. Hydrated weightoftheboneswasdeterminedusingafour decimalplacedigitalscale.Lengthoftheboneswasmeasured withcalipers.Specimenswereplacedontwosupportsthat were separatedbyadistanceof12mmandbentuntil frac-turebyloweringthecrossheadpositionedatthemid-shaftat aconstantspeedof0.033mm/s.Fromtheload–displacement curve,thepeakload(N),theultimatestiffness(N/mm),andthe toughness(mJ)wereobtained.Ultimatestress(strength)and Young’smoduluswerederivedfromload–deformationcurves obtainedbyusingequationsdescribedpreviously.22
Measurementoffemoraldryweightandashweight
Afterconductingthreepointbendingtest,thefemursofall animalsweredehydratedwithethanol,andfatwasremoved withdiethylether.Aftertheboneswere allowedtoair-dry, the dryboneweightwasmeasuredwithadigitalweighing balance.Next,thedriedfemurswereburnedtoashat900◦C
for5h,andtheirashweightwasmeasured.
Statisticalanalysis
comparedwiththeWilcoxonsigned-ranktest.Inallcases,a probabilityerroroflessthan0.05wasselectedasthecriterion forstatisticalsignificance.Graphswere drawnusingGraph PadPrism(version5.0forWindows).
Results
Effectofdifferenttreatmentsonbodyweightandfemoral length
Tenweeks after RHLI, the body weights were significantly lowerforanimalsintheRHLI(positivecontrol)andRHLI treat-ment groups compared with the non-immobilized normal group.Thisdifferencehadbecomegreaterattheendofthe experiment(RHLIforanother10weeks).However,therewere no statistically significant differences in weights observed betweenanyoftheactivetreatmentgroupsandthatofthe RHLI(positivecontrol)group(Table1).
There were no significant differences in immobilized (right) femoral length between positive control group (39.89±1.3mm), ZOL group (40.23±4.7mm), ALF group (39.78±8.4mm), ZOL+ALF group (40.69±10.4) and normal controlgroup(41.09±2.2mm).Moreover,therewereno sig-nificantdifferencesbetweentheimmobilized(right)sideand non-immobilized(left)side(datanotshown).
Effectofdifferenttreatmentsonboneporosity
TheX-rayimageshowsthedifferenceintheX-ray transmis-sionintensitydependingontheporosityofthesample.The X-raytransmissionintensity is directly proportional tothe porosity.TheeffectsofRHLIandsubsequenttreatmentwith alltherapeuticinterventionsontheporosityoftherightfemur weremeasured byX-rayimaging,asshowninFig.1. X-ray intensityfortheRHLI(positivecontrol)groupatR1(distal epi-physis),R2(mid-shaft:distal)R3(mid-shaft:proximal)andR4 (proximalepiphysis)wassignificantlyhigherthan thosefor thenon-immobilizednormalgroup,whichindicatesan immo-bilizationelicitedincreaseinboneporosityintheseareas.
Table1–Effectsofthedifferenttreatmentsonbody weight.
Group Bodyweight
Pre-treatment(g) Post-treatment(g)
Normalcontrol 253.2±10.65a 320.1±13.39a
RHLIpositivecontrol 230.1±18.22 216.6±9.01 RHLI+ZOL 229.4±11.22 218.0±10.19 RHLI+ALF 232.8±17.15 223.4±12.18 RHLI+ZOL+ALF 225.8±13.34 212.6±11.13
Pre-treatmentshowsthedataonthedaypriortothestartof treat-ment.Post-treatmentshowsdataonthefinaldayofthetreatment. Dataareexpressedasthemean±S.D(n=6),evaluatedbyone-way ANOVAfollowedbyTukey’smultiplecomparisontest.
a p<0.001,comparedtoRHLI(positivecontrol)group.Allgroups
exceptnormalgroupunderwentrighthind-limbimmobilization (RHLI).
After10weeksoftherapy,allactivetreatments(singleand combined)succeededindecreasingboneporosityinRHLIrats. X-raytransmissionintensityvaluesatR1(distalfemoral epi-physis) forZOL, ALFand ZOL+ALFgroups waslower than thoseofRHLI(positivecontrol)group(p<0.001).Similarly,the X-raytransmissionintensityvaluesatR2(distalfemoralshaft) forZOL,ALFandZOL+ALFgroupswaslowerthanthoseof RHLI (positive control) group (p<0.01; p<0.05 and p<0.001 respectively).Likewise,theX-raytransmissionintensity val-uesatR3(proximalfemoralshaft)forZOL,ALFandZOL+ALF groupswaslowerthanthoseofRHLI(positivecontrol)group (p<0.01;p<0.001andp<0.001respectively).Furthermore,the X-raytransmissionintensityvaluesatR4(proximalfemoral epiphysis)forZOL,ALFandZOL+ALFgroupswaslowerthan those of RHLI(positive control) group (p<0.01; p<0.01 and p<0.001 respectively). In contrast, the X-ray transmission intensityoftheZOL+ALFgroupwassignificantlylowerthan thatoftheZOLandALFgroupsatR1,R2,R3andR4regions (p<0.05).
Effectofdifferenttreatmentsonmechanicalpropertiesin thefemoralmid-shaft
Fig.2showsthepeakload,ultimatestiffness,toughness, ulti-matestrengthandYoung’smodulusinthefemoralmid-shaft, respectively.Three-pointbendingtestsoftherightfemur indi-catedthatRHLIcausedsignificantreductionsinthepeakload, ultimatestiffness,toughness,ultimatestrengthandYoung’s modulus comparedwiththose innon-immobilizednormal group(p<0.001).
In ZOL,ALFand ZOL+ALFgroups, the peakload ofthe femur was significantly higher than in the RHLI (positive control) group (p<0.05; p<0.01 and p<0.001, respectively). Similarly,ZOL,ALFandZOL+ALFgroups,theultimate stiff-ness of the femur was significantly higher than in the RHLI (positive control) group (p<0.01; p<0.01 and p<0.001 respectively). The toughnessofthe femur inthe ZOL, ALF and ZOL+ALF groups was significantlyhigher than in the RHLI (positive control) group (p<0.01; p<0.05 and p<0.001 respectively).Inallsingletreatments,thetoughnesswas sig-nificantly lower than that inthe ZOL+ALFgroup (p<0.05). Moreover, ZOL, ALF and ZOL+ALF groups, the ultimate strength of the femurwas significantlyhigher than in the RHLI(positivecontrol)group(p<0.001).InZOLandALFgroups, the ultimate strength was significantly lower than that in theZOL+ALFgroup(p<0.01;p<0.001,respectively). Further-more, theYoung’s modulusofthe ZOL, ALFand ZOL+ALF groupswassignificantlyincreasedwhencomparedwiththe RHLI (positive control) group (p<0.05; p<0.01; p<0.01 and p<0.001, respectively).Inall singletreatments,the Young’s moduluswassignificantlylower thanthatintheZOL+ALF group(p<0.05).
Comparisonoftheeffectofdifferenttreatmentsondryand ashweightsofimmobilizedandnon-immobilizedfemursin rats
Distal femoral epiphysis (R1)
Normal control RHLI control
RHLI + ZOL RHLI + ALF
RHLI + ZOL + ALF
Normal control RHLI control
RHLI + ZOL RHLI + ALF
RHLI + ZOL + ALF
Normal control RHLI control
RHLI + ZOL RHLI + ALF
RHLI + ZOL + ALF Normal control RHLI control
RHLI + ZOL RHLI + ALF
RHLI + ZOL + ALF 0
10 20 30
***
b***
a***
***
***
aPixel intensity, %
Distal femoral shaft (R2)
0 5 10 15 20 25
***
***
**
a*
b*
aPixel intensity, %
Proximal femoral shaft (R3)
0 5 10 15 20 25
***
*** ***a
*b **a
Pixel intensity, %
Proximal femoral epiphysis (R4)
0 10 20 30
***
***
**a **
a
Pixel intensity, %
Fig.1–Effectofzoledronicacidandalfacalcidol,aloneorincombinationonfemoralporosity.BoneporosityofR1:distal femoralepiphysis,R2:distalfemoralshaft,R3:proximalfemoralshaft,R4:proximalfemoralepiphysis.Dataareshownas themean±SD(n=6),evaluatedbyTukey’smultiplecomparisontest.*p<0.05;**p<0.01;***p<0.001,comparedtoRHLI (positivecontrol)group;ap<0.05,comparedtoZOL+ALFgroup.Allgroupsexceptnormalgroupunderwentrighthind-limb
immobilization(RHLI).
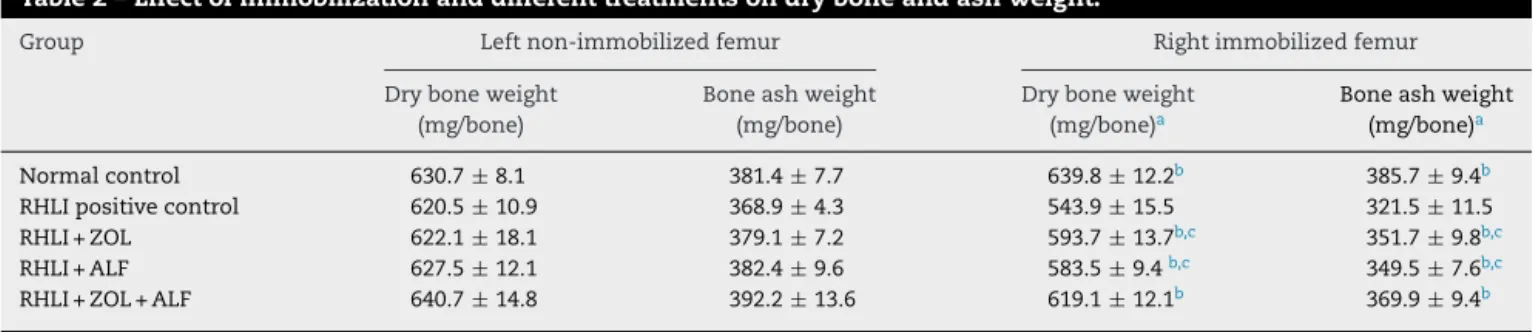
Table2–Effectofimmobilizationanddifferenttreatmentsondryboneandashweight.
Group Leftnon-immobilizedfemur Rightimmobilizedfemur
Dryboneweight
(mg/bone)
Boneashweight
(mg/bone)
Dryboneweight
(mg/bone)a
Boneashweight (mg/bone)a
Normalcontrol 630.7±8.1 381.4±7.7 639.8±12.2b 385.7±9.4b RHLIpositivecontrol 620.5±10.9 368.9±4.3 543.9±15.5 321.5±11.5 RHLI+ZOL 622.1±18.1 379.1±7.2 593.7±13.7b,c 351.7±9.8b,c RHLI+ALF 627.5±12.1 382.4±9.6 583.5±9.4b,c 349.5±7.6b,c RHLI+ZOL+ALF 640.7±14.8 392.2±13.6 619.1±12.1b 369.9±9.4b
Dataareexpressedasthemean±S.D(n=6),evaluatedbyone-wayANOVAfollowedbyTukey’smultiplecomparisontest. a Indicates,fortheparameter,asignificantdifferenceoftheactivetreatmentsbetweenthetwo.
b p<0.001,comparedtoimmobilizedRHLI(positivecontrol)group;legs.
Normal controlRHLI control RHLI + ZOL RHLI + ALF
RHLI + ZOL + ALF Normal control
RHLI control RHLI + ZOL RHLI + ALF
RHLI + ZOL + ALF
0 50 100
150 ***
***
* **
Peak load (N)
0 100 200 300
**
*** ** ***
Ultimate
Stiffness (N/mm)
Normal control RHLI control
RHLI + ZOL RHLI + ALF
RHLI + ZOL + ALF Normal control
RHLI control RHLI + ZOL RHLI + ALF
RHLI + ZOL + ALF
Normal control RHLI control
RHLI + ZOL RHLI + ALF
RHLI + ZOL + ALF
0 10 20 30 40 50
*
a***
***
**
aToughness (mJ)
0 100 200 300
***
***b ***c
***
Ultimate
strength (MPa)
0 2 4 6
**
a***
***
**
aYoung's
Modulus (GPa)
Fig.2–Effectsofzoledronicacid,alfacalcidol,orzoledronicacidplusalfacalcidolonthemechanicalstrengthofthefemoral diaphysis.Thediaphysiswassubjectedtothree-pointbendingtofailure,whichprovideddataonpeakload,ultimate stiffness,toughness,ultimatestrength,andYoung’smodulus.Dataareshownasthemean±SD(n=6),evaluatedbyTukey’s multiplecomparisontest.*p<0.05;**p<0.01;***p<0.001,comparedtoRHLI(positivecontrol)group;ap<0.05;bp<0.01,c
p<0.001;comparedtoZOL+ALFgroup.Allgroupsexceptnormalgroupunderwentrighthind-limbimmobilization(RHLI).
ashweightsweresignificantlyheavierthanthoseintheRHLI (positivecontrol)group.TheRHLIfemuroftheratstreated withZOL+ALF,thedryweightwassignificantlyheavierthan thoseinZOLorALFtreatedgroups(p<0.05intheALFgroup). Moreover,theRHLIfemuroftheratstreatedwithZOL+ALF
Comparisonbetweennon-immobilized(left)legand immobilized(right)legwithinasamegroup
Theboneporosityandmechanicalpropertiesoftheleftand rightlegsareplottedas“split-bar”diagramsinFigs.3and4, respectively. Anasterisk indicates thatthere was a signifi-cantdifferencebetweentheleftandrightlegwithinthesame group.AtR1,R2,R3andR4regions,theX-raytransmission intensityfortheimmobilizedside(right)seemedsignificantly higherthanthosefromthenon-immobilizedside(left)inthe RHLI(positivecontrol)group(p<0.001).Similarly,atR1,R2,R3 andR4regions,theX-raytransmissionintensityforthe immo-bilizedside(right)seemedsignificantlyhigherthanthosefrom thenon-immobilizedside(left)intheRHLIgroupstreatedwith ZOLorALF(p<0.05).Incontrast,theRHLIgrouptreatedwith ZOL+ALFshowedfullprotectionagainstdisuseosteoporosis atR1,R2,R3andR4regions,asindicatedbyX-raytransmission intensityvalues(Fig.3).
Atthe femoralmid-diaphysis(three-point bendingtest), the effect ofimmobilization was very pronouncedin RHLI (positivecontrol)group;thatis,theimmobilizedside(right) hadsignificantlylowervaluesofstrengthparameters includ-ingpeakload,ultimatestiffness,fracturetoughness,ultimate strengthandYoung’smodulusthanthenon-immobilizedside (left) (p<0.001). Similarly, in the RHLI groups treated with ZOL or ALF, the immobilized side (right) had significantly (p<0.01)lowervaluesofstrengthparametersincludingpeak load,ultimatestiffness,fracturetoughness,ultimatestrength andYoung’smodulusthanthenon-immobilizedside(left).In contrast,theRHLIgrouptreatedwithZOL+ALFshowedfull protectionagainstimmobilization(Fig.4).
Discussion
To our knowledge, the combined effects ofanti-resorptive andanabolicagentsontheskeletonhavenotspeciallybeen assessedin rat model ofdisuse osteoporosis. The present study was conducted to clarify the efficacy of combined administrationofZOLandALFonoverallqualityofbonein RHLIrats.TheresultsofthisstudyshowedthatZOLandALF monotherapywasable tocounteractthebonelossinarat modelofdisuseosteoporosis.Theanti-osteoporoticproperty ofZOL plusALF combinationtherapyappearedtobemore effectivewhencomparedtoZOLorALFmonotherapy.Thus, weconfirmedthebeneficialeffectsofcombined administra-tionofZOLandALFfortreatmentofdisuseosteoporosisin rats.
Bodyweightinthenormalgroupwasgreaterthaninthe RHLI(positivecontrol)group.Thismayhavebeenduetothe anesthesiaadministeredduringtheRHLIprocedure.Reduced eatingandoverallreducedmobilityareotherpossiblefactors thatmayhavecontributedinaminorwaytothedevelopment oflowerbodyweightandboneloss.Earlierstudieshaveshown asimilardecreaseinbodyweightafterRHLI.9,23 Thelength ofthe femurofthe immobilizedlimbwasnotsignificantly differentfromthatofthenon-immobilizedintactfemurofthe samerat,suggestingthatthelongitudinalgrowthofthebone isnotretardedintheseanimals.Itisthereforemorelikelythat weareheredealingwithimmobilizationosteoporosisrather thansimplegrowthretardation.
ProminentincreaseinboneporositywasobservedatR1, R2,R3and R4,afterimmobilizationofrighthind-limb.The increase in the bone porosity at R1, R2, R3, R4 regions of rat femoral bone,due tounloading ofright hind-limbwas suppressed by treatment with ZOL, ALF and ZOL+ALF. In the analysis ofthe boneporosity ofrat femur usingX-ray imaging, it was foundthat combination therapy with ZOL +ALFwasstatisticallysuperiortoZOL orALFmonotherapy insuppressingtheincreaseinboneporosityduetoRHLI.This indicatesthatcombinationtherapywithZOL+ALFthickens andstrengthenscorticalbone.
Itshouldbenotedthat,inratstreatedwithZOL,ALFand ZOL+ALF,dryandashweightsintherightimmobilizedfemur weresignificantlygreaterthanthoseoftheRHLI(positive con-trol)group.Moreover,intheanimalstreatedwithcombined therapyofZOL+ALF,dryandashweightsintheright immo-bilizedfemurweresignificantlygreaterthanthoseoftheZOL orALFgroups.Theseresultsshowedthatthecombined treat-mentwithZOL+ALFisbeneficialforincreasingthemassof ratfemoralbonesthatwasdecreasedduetoRHLI.
Bone mechanicalproperties are relatedtobonedensity, architecture,connectivityandmineralization.23 Immobiliza-tion resultsindecreasedmechanical properties9,24 and the samewasobservedinthepresentstudy.Inthisexperiment, themechanicalpropertiesoftheratfemoralbonedecreased in RHLI (positive control) group when compared to non-immobilized normal control group, suggesting an increase in thefragilityofthe corticalboneofRHLIrats. Resultsof thebendingtestinratstreatedwithZOL,ALFandZOL+ALF indicatehigherultimatepeakload,stiffness,energy,bending stressandYoung’smoduluscomparedtoRHLI(positive con-trol)grouprats.CombinationtherapywithZOL50+ALFwas statisticallysuperiortoZOLorALFmonotherapyatincreasing femoralmid-shafttoughness,ultimatestrength,andYoung’s modulus.
Comparisonmadebetweennon-immobilized(left)legand immobilized(right)legwithinasamegroupshowedthatbone propertieswereimprovedbyalltherapeuticinterventions,but themarkedosteopeniainducedbyRHLIwasnotcompletely corrected withZOL or ALFmonotherapy. In contrast, com-binedtreatmentwithZOL+ALFshowedfullprotectionagainst disuseosteoporosis,suggestingthatthecombinationtherapy hasatherapeuticadvantageovereachdrugmonotherapyfor thetreatmentofdisuseosteoporosis.
Distal femoral epiphysis (R1)
0 10 20 30
Normal control RHLI control IPTD + ZO L
RHLI + ZOL
RHLI + ZOL + ALF
Normal control RHLI control RHLI + ZOL IPTD + AL
F
RHLI + ZOL + ALF
Normal control RHLI control RHLI + ZOL IPTD + AL
F
RHLI + ZOL + ALF Normal control RHLI control RHLI + ZOL
IPTD + AL F
RHLI + ZOL + ALF
***
*
*
Pixel intensity, %
Distal femoral shaft (R2)
0 5 10 15 20 25
***
*
*
Pixel intensity, %
Proximal femoral shaft (R3)
0 5 10 15 20
25
***
*
*
Pixel intensity, %
Proximal femoral epiphysis (R4)
0 10 20 30
***
* *
Pixel intensity, %
Fig.3–Femoralporosityforthenon-immobilized(leftbar)andtheimmobilized(rightbar)sidewithinthesamegroup. Asteriskdenotessignificantdifferencebetweenthenon-immobilizedsideandtheimmobilizedside(mean±SD).Allgroups exceptnormalgroupunderwentrighthind-limbimmobilization(RHLI).
eventslikeesophagitis7;(3)itwasfoundthatunderconditions likelytostimulatebisphosphonatebindingontobone,ZOLhas higherbindingaffinityamongallotherbisphosphonatesfor bonehydroxyapatite27;(4)the costofZOLiscomparableto theannual costoforalbisphosphonates andless than the costoftheotherintravenousbisphosphonate(ibandronate), whichisadministeredevery3months.27However,parenteral administrationsofbisphosphonateshaveshownacutephase response,hypocalcemiaandsecondaryhyperparathyroidism, musculoskeletalpain,renalcomplications, osteonecrosisof thejawandoculareventsinsomecases.7,27,28Theresultsof ourpreviousstudyshowedthatalowerdoseofZOL(50g/kg,
singleintravenousdose)hadshowedsimilarpromisingand beneficial effects in treating osteoporosis when compared withthetherapeuticdoseofZOL(100g/kg,singleintravenous
dose)inestrogendeficientrats.29Therefore,toreducetherisk ofknown adversedrugreactionsbyZOL,wechosealower doseofZOL(50g/kg,singleintravenousdose).
ALFisused totreatosteoporosis becauseit exerts both anabolic and antiresorptive effects on the skeleton.13,18,19
However, higher doses of ALF may increase the risk of hypercalciuria or hypercalcemia.On the other hand, treat-ment withZOL maycause hypocalcemiabysuppressionof bone resorption.17 The different mechanisms of ZOL and ALF suggest that a combination therapy using ZOL with ALF may eliminateor minimizethe riskofknown adverse drug reactions previously seen by these two drugs when administeredalone.Basedontheresultsofourpreviousand presentfindings,weproposethatcombinationtherapywith ZOL+ALFactsbyincreasingboneformation(bystimulating theformationandactionofosteoblastcells)anddecreasing bone resorption (by inducing osteoclast apoptosis), thus rebalancing bone turnover in favor of bone formation, an effect that results in increased bone mass and strength. This can possibly explain how combination therapy with ZOL+ALFwasmoreeffectivethanZOLorALFmonotherapy inincreasingbonemassandstrengthinRHLIrats.
0 50 100 150 200
Normal control
RHLI control RHLI + ZOL RHLI + AL
F
RHLI + ZO
L + AL F
Normal control RHLI
con trol
RHLI + ZOL RH LI +
ALF
RH LI +
ZOL + AL
F
Normal control RHLI
con trol
RHLI + ZOL RH LI + ALF
RH LI +
ZOL + AL
F
Normal control RH
LI con trol
RHLI + ZOL RH LI +
ALF
RHLI + ZOL + AL
F Normal control
RHL I con
trol
RHLI + ZOL RHLI + ALF
RHLI + ZO
L + AL F
***
*
*
Peak load (N)
0 100 200 300 400
*** * *
Ultimate stiffness
(N/mm
)
0 10 20 30 40
50
***
**
**
Toughness (m
J)
0 100 200 300
*** ** **
Ultimate strength
(MPa
)
0 2 4 6
***
**
**
Young's modulus (GPa)
Fig.4–Mechanicalpropertiesforthenon-immobilized(leftbar)andtheimmobilized(rightbar)sidewithinthesame group.Thefemoralmid-shaftwassubjectedtothree-pointbendingtofailure,whichprovideddataonpeakload,ultimate stiffness,toughness,ultimatestrength,andYoung’smodulus.Asteriskdenotessignificantdifferencebetweenthe non-immobilizedsideandtheimmobilizedside(mean±SD).Allgroupsexceptnormalgroupunderwentrighthind-limb immobilization(RHLI).
thatofhumans;(3)inthepresentstudy,agrowingratmodel wasused.Thus,maturation-relatedgainsinbonemasscould notbeignoredinRHLIrats;(4)furthermore,theeffectofZOL andALFoncorticalporosity,whichcouldbeobservedinaged RHLIratswasnotassessed.Therefore,theresultsofpresent studycannotbetranslatedintohumanwithprimarydisuse osteoporosis.Thus,furtherstudiesareneededtoconfirmthe
beneficialeffectsofcombinedadministrationofZOLandALF onthebonemassinRHLIrats.
Conclusions
inimproving thebonepropertiesinanratmodelofdisuse osteoporosis,suggestingthatthecombinationtherapyhasa therapeuticadvantageoverZOLorALFmonotherapyforthe treatmentofdisuseosteoporosisinducedbymechanical inac-tivity.Assuch,thiscombinedregimenmaybeofinterestfor furtherevaluationinclinicalstudies.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
AuthorswouldwholeheartedlythankProf.B.G.Shivananda, Principal,Al-AmeenCollegeofPharmacyforhiskindsupport andencouragementtocarryoutthisproject.Theauthorsare thankful toMr. B.K Jain,Naprod Life Sciences, Maharash-tra,India forprovidinggiftsampleofZoledronic acid.The authorsalsogratefullyacknowledgethecontributionofMr. VijayKumarandMr.ManishKumarPriydarshifrom Depart-mentofAerospaceEngineering,IndianInstituteofScience,in carryingouttheX-rayimagingandthreepoint-bendingtests.
r
e
f
e
r
e
n
c
e
s
1. LiCR,ZhangGW,NiuYB,PanYL,ZhaiYK,MeiQB. AntiosteoporosiseffectofRadixScutellariaeextracton densityandmicrostructureoflongbonesintail-suspended Sprague-Dawleyrats.Evidence-BasedComplemAlternat Med.2013;2013:753703.
2. BarouO,Lafage-ProustMH,MartelC,ThomasT,TirodeF, LarocheN,etal.Bisphosphonateeffectsinratunloaded hindlimbbonelossmodel:three-dimensional
microcomputedtomographic,histomorphometric,and densitometricanalyses.JPharmacolExpTher.1999;291:321–8.
3. WatersDJ,CaywoodDD,TurnerRT.Effectoftamoxifencitrate oncanineimmobilization(disuse)osteoporosis.VetSurg. 1991;20:392–6.
4. RussellRG,WattsNB,EbetinoFH,RogersMJ.Mechanismsof actionofbisphosphonates:similaritiesanddifferencesand theirpotentialinfluenceonclinicalefficacy.OsteoporosInt. 2008;19:733–59.
5. BlackDM,DelmasPD,EastellR,ReidIR,BoonenS,CauleyJA. Once-yearlyzoledronicacidfortreatmentofpostmenopausal osteoporosis.NEnglJMed.2007;356:1809–22.
6. LambrinoudakiI,VlachouS,GalapiF,PapadimitriouD, PapadiasK.Once-yearlyzoledronicacidinthepreventionof osteoporoticbonefracturesinpostmenopausalwomen.Clin IntervAging.2008;3:445–51.
7. KhajuriaDK,RazdanR,MahapatraDR.Drugsforthe managementofosteoporosis:areview.RevBrasReumatol. 2011;51:365–82.
8. ReidDM,DevogelaerJP,SaagK,RouxC,LauCS,ReginsterJY, etal.Zoledronicacidandrisedronateinthepreventionand treatmentofglucocorticoid-inducedosteoporosis(Horizon):a multicentre,double-blind,double-dummy,randomised controlledtrial.Lancet.2009;373:1253–63.
9. KhajuriaDK,DishaC,RazdanR,MahapatraDR,VasireddiR. Prophylacticeffectsofpropranololversusstandardtherapy onanewmodelofdisuseosteoporosisinrats.SciPharm. 2014;82:357–74.
10.VeggerJB,NielsenES,BrüelA,ThomsenJS.Additiveeffectof PTH(1-34)andzoledronateinthepreventionofdisuse osteopeniainrats.Bone.2014[Epubaheadofprint].
11.ShiraishiA,MiyabeS,NakanoT,UmakoshiY,ItoM,Mihara M.Thecombinationtherapywithalfacalcidoland risedronateimprovesthemechanicalpropertyinlumbar spinebyaffectingmaterialpropertiesinanovariectomized ratmodelofosteoporosis.BMCMusculoskeletDisord.2009; 10:66.
12.KhajuriaDK,DishaC,RazdanR,MahapatraDR.Comparative evaluationofzoledronicacid,alfacalcidol,andpropranololin pharmacologicalcorrectionofexperimentalosteoporosis.Lat AmJPharm.2013;32:968–76.
13.ErbenRG.VitaminDanalogsandbone.JMusculoskelet NeuronalInteract.2001;2:59–69.
14.SchachtE,DukasL,RichyF.Combinedtherapiesin osteoporosis:bisphosphonatesandvitaminD-hormone analogs.JMusculoskeletNeuronalInteract.2007;7:174–84.
15.deNijsRN,JacobsJW,LemsWF,LaanRF,AlgraA,Huisman AM,etal.Alendronateoralfacalcidolin
glucocorticoid-inducedosteoporosis.NEnglJMed. 2006;355:675–84.
16.IzawaY,MakitaT,HinoS,HashimotoY,KushidaK,InoueT, etal.ImmobilizationosteoporosisandactivevitaminD: effectofactivevitaminDanalogsonthedevelopmentof immobilizationosteoporosisinrats.CalcifTissueInt. 1981;33:623–30.
17.KhajuriaDK,RazdanR,MahapatraDR.Zoledronicacidin combinationwithalfacalcidolhasadditiveeffectson trabecularmicroarchitectureandmechanicalpropertiesin osteopenicovariectomizedrats.JOrthopSci.2014[Epub aheadofprint].
18.IwamotoJ,MatsumotoH,TakedaT,SatoY,XuE,YehJK. Effectsofalendronateandalfacalcidolonthefemoralbone massandbonestrengthinorchidectomizedrats.ChinJ Physiol.2008;51(December):331–7.
19.IwamotoJ,SekiA,TakedaT,SatoY,YamadaH,YehJK.Effect ofrisedronateonthecorticalandcancellousbonemassand mechanicalpropertiesinovariectomizedrats:acomparison withtheeffectsofalfacalcidol.JNutrSciVitaminol. 2006;52:393–401.
20.FredianiB,AllegriA,BisognoS,MarcolongoR.Effectsof combinedtreatmentwithcalcitriolplusalendronateonbone massandboneturnoverinpostmenopausalosteoporosis: twoyearsofcontinuoustreatment.ClinDrugInvest. 1998;15:235–44.
21.MalavoltaN,ZanardiM,VeronesiM,RipamontiC,GnudiS. Calcitriolandalendronatecombinationtreatmentin menopausalwomenwithlowbonemass.IntJTissueReact. 1999;21:51–9.
22.KhajuriaDK,RazdanR,MahapatraDR,BhatMR.
Osteoprotectiveeffectofpropranololinovariectomizedrats: acomparisonwithzoledronicacidandalfacalcidol.JOrthop Sci.2013;18:832–42.
23.FaibishD,OttSM,BoskeyAL.Mineralchangesin osteoporosis:areview.ClinOrthopRelatRes.2006;443: 28–38.
24.MosekildeL,ThomsenJS,MackeyMS,PhippsRJ.Treatment withrisedronateoralendronatepreventshind-limb immobilization-inducedlossofbonedensityandstrengthin adultfemalerats.Bone.2000;27:639–45.
25.ShirkeSS,JadhavSR,JagtapAG.Methanolicextractof Cuminumcyminuminhibitsovariectomy-inducedboneloss inrats.ExpBiolMed(Maywood).2008;233(11):
1403–10.
27.PapapoulosSE.Bisphosphonates:howdotheywork?Best PractResClinEndocrinolMetab.2008;22:831–47.
28.SuK,ShiX,VarshneyRR,WangD.Transplantabledelivery systemsforinsitucontrolledreleaseofbisphosphonatein orthopedictherapy.ExpertOpinDrugDeliv.2011;8:113–26.