www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
REVIEW
ARTICLE
Vitamin
D
in
children
and
adolescents
with
sickle
cell
disease:
an
integrative
review
Jacqueline
Faria
de
Oliveira,
Natália
Gomes
Vicente,
Juliana
Pereira
Pontes
Santos,
Virgínia
Resende
Silva
Weffort
∗UniversidadeFederaldoTriânguloMineiro(UFTM),Uberaba,MG,Brazil
Received12May2014;accepted23September2014 Availableonline29June2015
KEYWORDS
VitaminD;
VitaminDdeficiency; Sicklecellanemia; Child;
Adolescent
Abstract
Objective: ToreviewtheliteratureabouttheprevalenceofvitaminDdeficiencyandits
con-sequencesinchildrenandadolescentswithsickle-celldisease.
Datasources:Theliteraturesurveywasperformedthroughthebibliographicdatabases
MED-LINE;U.S.NationalLibraryofMedicineandNationalInstitutesofHealth(PubMed);Literatura
Latino-Americana edoCaribeem CiênciasdaSaúde(Lilacs),andtheCochraneLibrary.The
keywordswereselectedusingMedicalHeadingTerms(MeSH):‘‘vitaminD’’OR‘‘vitaminD
defi-ciency’’AND‘‘anemia,sicklecell’’AND‘‘child’’AND‘‘adolescent’’.Thesearchwaslimited
toarticlesinEnglish,SpanishandPortuguese,publisheduntilApril2014.
Datasynthesis: Eleven articles were selected among the 18 found. In 6of the 11 studies,
serum levelsofvitaminD inchildren and/oradolescentswith sickle-cell anemiawere low.
The prevalenceofvitaminDdeficiencyinpatientswithsickle-cell anemiaexceededthatof
thecomparisongroup.The lowintakeofvitaminD, seasonality,exposuretosun,increased
metabolismassociatedwiththehemoglobinopathy,andageincreasewerefactorsassociated
with the deficiency. There was an association between a significant vitamin D deficiency
and boneweaknessandpainful crises.There wasa positive correlationbetween increased
levelsofvitaminDbysupplementationandfunctional,physicalcapacity.
Conclusions: ThevitaminDdeficiencyinchildrenandadolescentswithsickle-celldisease is
prevalent andrequiresfurtherstudiestodemonstrateitsassociationwithcomorbiditiesand
possiblebenefitsofvitaminDsupplementation.
© 2015 Sociedadede Pediatriade São Paulo. Publishedby Elsevier Editora Ltda. Allrights
reserved.
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rpped.2014.09.008 ∗Correspondingauthor.
E-mail:[email protected](V.R.S.Weffort).
PALAVRAS-CHAVE
VitaminaD; Deficiênciade vitaminaD; Anemiafalciforme; Crianc¸a;
Adolescente
VitaminaDemcrianc¸aseadolescentescomdoenc¸afalciforme:umarevisão
integrativa
Resumo
Objetivo: RevisaraliteraturasobreafrequênciadadeficiênciadevitaminaDesuas
conse-quênciasemcrianc¸aseadolescentescomanemiafalciforme.
Fontesdedados: OlevantamentobibliográficofoifeitonasbasesbibliográficasMEDLINE,U.S.
National Library of Medicine e National Institutes of Health (PubMed), Literatura
Latino-Americana e do Caribe em Ciências da Saúde (Lilacs) e Cochrane. Os descritores foram
selecionadoscomousodoMedicalHeadingTerms(MeSH):‘‘vitaminD’’OU‘‘vitaminD
defi-ciency’’E‘‘anemia,sicklecell’’E‘‘child’’E‘‘adolescent’’.Abuscalimitou-seaosartigosem
inglês,espanholeportuguês,comdatadepublicac¸ãoatéabrilde2014.
Síntesedosdados: Foramselecionados11estudos,entreos18encontrados.Apesquisarevelou
que osníveis séricos de vitamina Dem crianc¸as e/ou adolescentes comanemia falciforme
encontram-sebaixosemseisde11artigosanalisados.Essafrequênciadedeficiênciadevitamina
Dempacientescomanemia falciformeexcedeadogrupodecomparac¸ãosaudável.A baixa
ingestadevitaminaD,asazonalidade,aexposic¸ãosolar,ometabolismoaumentadopróprioda
hemoglobinopatiaeoaumentodaidadesãofatoresassociadosàdeficiência.Houveassociac¸ão
entredeficiênciasignificativadevitaminaDefraquezaósseaecrisesdolorosas.Hácorrelac¸ão
positivaentreaumentodosníveisdevitaminaDpormeiodasuplementac¸ãoeacapacidade
funcionalfísica.
Conclusões: A deficiênciade vitaminaDem crianc¸ase adolescentescomdoenc¸afalciforme
éprevalenteenecessitademaisestudosparaevidenciarasuarelac¸ãocomcomorbidadese
possíveisbenefíciosdasuplementac¸ãodavitaminaD.
© 2015SociedadedePediatria de SãoPaulo. Publicado porElsevier EditoraLtda. Todosos
direitosreservados.
Introduction
Sicklecell diseaseis caused by amutation resultingfrom an exchange of nitrogenous bases in the sixth codon of thebeta-globulinhemoglobingene,generatinganabnormal hemoglobincalledhemoglobinS(HbS).1Themanifestations
of sickle-cell disease are due to the presence of HbS, of whichmoleculesareorganizedintopolymericbeamswhen deoxygenated and give the RBC an elongated and rigid conformation, called a ‘‘sickle-shaped red blood cell’’.2
After the sickling process, the red blood cells begin to showchangesinmembraneproteinsandincreased expres-sion of adhesion molecules that, consequently, lead to red blood cell adhesion tothe endothelium. This process triggersaninflammatoryphenomenon,activationof coagu-lation,hypoxia,ischemiaandlocalinfarction,inadditionto reducedRBCsurvival.2Sickle-celldiseaseisoneofthemost
commongeneticdiseases inBrazil andin theworld.3 The
chronichemolysis,anemia,andvaso-occlusive phenomena that occur in patients with the disease are triggers of an accelerated metabolism, and this process leads to a basalmetabolicrate20%higherinpatientwithsickle-cell anemia than in the normal population.1,4 However, there
are no records of methodologies and equations to esti-mate the energy expenditure in children with sickle-cell anemia.5
Children with sickle cell anemia have a higher risk of developing nutritional deficiencies due to reduced appetite,6 poor dietary intake of nutrients7 and
infec-tiouscomplications,whichdemandsgreaterattentionfrom
healthprofessionals.Amongthevitamins,vitaminDmustbe carefullyevaluatedinchildrenwithsickle-cellanemia.This isduetothehighconcentrationofmelaninintheskin,low levelsofphysicalactivity,8andlowfoodintake.7,9Children
withsickle-cellanemiaaremorelikelytodevelop vitamin Ddeficiencywhencomparedtothehealthycontrols.10
Cal-ciumandvitaminDareimportantforbonemetabolism,and the low calcium intake leads to a reduction in the ideal bone mass peak in children and adolescents with sickle-cellanemia,whichdeterminesgrowthfailure.11 VitaminD
deficiency,inturn,isassociatedwithincreasedrespiratory infections,muscleweaknessandincreasedriskoffallsand microlesions.12Additionally,inchildrenwithsickle-cell
ane-mia,whose bonesareaffectedbyinfarction,osteoporosis and osteonecrosis,vitamin D deficiency mayworsenbone condition.13
Considering thesefacts, this study aimed to carry out anintegrativeliteraturereviewtoanalyzethefrequencyof vitamin Ddeficiency anditsconsequencesinchildren and adolescentswithsickle-cellanemia.
Literature
review
usingMedicalSubjectHeadingTerms (MeSH).Thoseterms were used for the search in the MEDLINE database, and subsequentlyadaptedandtranslatedintoSpanishand Por-tuguese for the search in other databases. The following parameterswere used: ‘‘vitaminD’’ OR ‘‘vitamin D defi-ciency’’ AND ‘‘anemia, sickle cell’’ AND ‘‘child’’ AND ‘‘adolescent’’.
Inclusioncriteriafortheselectionwerearticlespublished inEnglish,PortugueseandSpanish,withastudypopulation intheagerangeofchildrenandadolescents,youngerthan 18yearsold,withsickle-celldisease.Exclusioncriteriawere animalstudiesandhumanstudiesthatdidnotincludethe predeterminedagerangeandthathadnoassociationwith sickle-cellanemia.Notimelimitwasconsideredforthe bib-liographicsearch.Thereferencesearchwascarriedoutfrom December2013toApril2014.
To eliminate article duplication, documents were ordered by titles and authors, and those that appeared morethanoncewereexcluded.Fortheselection of stud-ies,areview oftitles andabstractswasperformed. After the first review, 18 articles were selected: 2 from the Cochrane Library database, 15 from PubMed and 1 from LILACS database. After the initial selection, a new text evaluation was carried out in full texts, resulting in the exclusionof7items.Thesearticleswereexcluded,asthey didnotcontemplatetheagerangedescribedinthe inclu-sioncriteria.Attheendoftheevaluation,weselectedone articlefromtheCochranedatabaseand10fromthePubmed database.
The studies were entered in a Microsoft Office Excel 2007® spreadsheet with recorded information on title, authors, journal, year of publication, objective, study design, population, level of evidence, main results and conclusions of thestudy.The developed studies had their experimentalprotocolsapprovedbytheInstitutionalReview Boardoftherespectiveinstitutions.Becausethisisareview andupdateonthesubject,thepresentstudywasnot sub-mittedtotheInstitutionalReviewBoardatourinstitution.
The aforementioned hierarchizationbasedonthelevel of evidence was carried out following the classification methodologyaccordingtostudydesign, whichcategorizes the studies inseven levels.14,15 In the firstlevel, the
evi-denceisderivedfromsystematicreviewormeta-analysisof allrelevantrandomizedcontrolledclinicaltrials;atlevel2, fromatleastonerandomized,controlledandwell-designed clinicaltrial;inlevel3,evidencefromwell-designedclinical trials,withoutrandomization;level4,evidencefrom well-designed cohort and case-control studies; level 5, results of systematic review of descriptive and qualitative stud-ies;level6,evidencederivedfromdescriptiveorqualitative study,andlevel7,evidencefromexperts’opinionsand/or reportsofexpertcommittees.
Thefinalreviewsampleconsistedof11articles,ofwhich representationsareshowninTable1.
Discussion
SerumlevelsofvitaminDandsicklecellanemia
Intheselectedstudies,vitaminDdeficiencywastreatedas an objectof primaryor secondary research,when
associ-atedtothemainsubjectofthestudy.AccordingtoDietary ReferenceIntakes,vitaminDdeficiencyoccurswhenserum 25-hydroxyvitaminDlevelsare<11ng/mL.11
SevenoftheninearticlesanalyzedserumvitaminDlevels inchildrenand/oradolescentswithsickle-celldiseaseand showedadeficiencyofthisnutrient.9,16---21Jacksonetal.,ina
cohortofchildreninwhomvitaminDlevelsweremeasured, found that96.4% had vitamin D deficiency and,of these, 64.0%hadseveredeficiency (<10ng/mL);1.4%had insuffi-cient levels,andonly threechildren (2.2%)had adequate levels.16VanderDijsetal.observedthat,whencomparedto
healthycontrols,patientswithsickle-cellanemiahadlower serumcalciumconcentrations.Theselevels,however,were notbelowthereferencevalues.Inthesamestudy,therewas nodifferencebetweenthegroupsregardingthephosphate, parathormoneandvitaminDlevels.22However,other
stud-iesdemonstratedthatthefrequencyoflowserumlevelsof vitaminDinthegroupwithsickle-cellanemiaexceededthe frequencyfoundinthehealthygroup.9,10
Due to the participation of solar radiation in vita-min D metabolism, a review study evaluated seasonal variations, demonstrating higher serum levels of vitamin D in the seasons with higher temperatures, spring and summer.9,16Inanotherstudy,however,thisvariationwasnot
demonstrated.18
Anotherdetermining factor for the adequacy of serum levelsof vitamin D and calciumis proper foodintake. In sickle-celldisease,nutritionalneedsaregreaterduetothe higherenergyrequirement.10Studiesevaluatingfoodintake
ofsubjectsthathadvitaminD deficiencyhaveshownthat dietary intake of the vitamin is not appropriate.9,10 The
intakeofvitaminDwasbelowtherecommendedvaluesof 200IU(5mg/day).9,11 Thelowconsumptionofmilk,source
ofcalciumandvitaminD,tendstodeclineevenmorewith age,leadingtoincreasingly lowerserumlevelsof vitamin withincreasingage.9
Thedifferenceduringtheagingprocesswasalso demon-strated by Garrido etal., whoreported low serum levels ofvitaminDinchildrenyoungerthan5years,but,in chil-drenolderthan5years,thisdeficiencywasevenhigher.No childolderthan 5yearsshowedacceptablelevelsof vita-min D.18 These results arein parallel withanother study,
whichshowedaninversecorrelationbetweenthelevelsof vitaminDandage,thatis,theoldertheage,thelowerthe levelsofvitamin D.Inthisstudy,osteocalcinserumlevels werelowerthanthosefoundinhealthychildren,whichmay be a consequence of vitamin D deficiency.20 Osteocalcin,
whichparticipatesinbonemineralization,issynthesizedby osteoblasts,andtheirinductionoccursbyvitaminD3. Osteo-calcinlevels are higher during childhood, and their peak occursduringpuberty.23Thisfactcouldexplaintheinverse
correlation,astheoldertheage,thehighertheproduction ofosteocalcin.
SerumlevelsofvitaminDandcomorbidities
Someselected studiesassessed theassociation of vitamin D deficiency with comorbidities in patients with sickle-cellanemia.9,16,17,20,21,24 Jackson et al.,in a retrospective
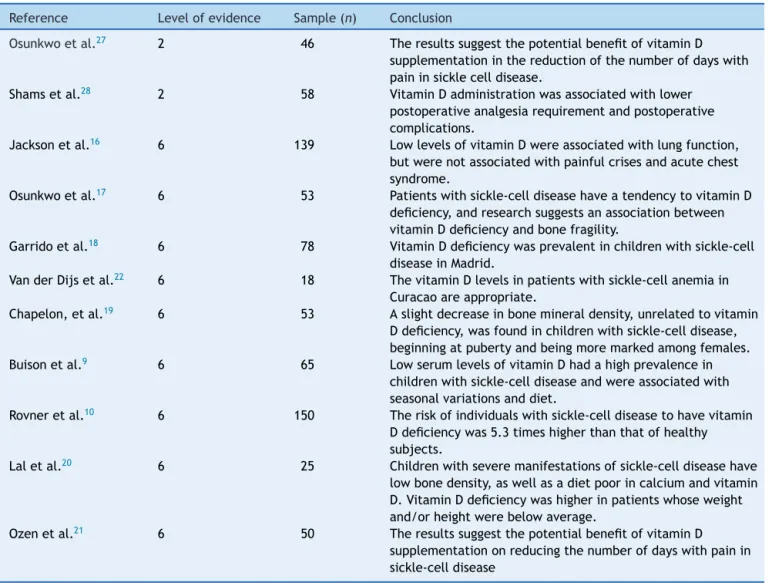
Table1 Summaryofselectedarticlesforthereview:sicklecelldiseaseandvitaminD.
Reference Levelofevidence Sample(n) Conclusion
Osunkwoetal.27 2 46 TheresultssuggestthepotentialbenefitofvitaminD
supplementationinthereductionofthenumberofdayswith paininsicklecelldisease.
Shamsetal.28 2 58 VitaminDadministrationwasassociatedwithlower
postoperativeanalgesiarequirementandpostoperative complications.
Jacksonetal.16 6 139 LowlevelsofvitaminDwereassociatedwithlungfunction,
butwerenotassociatedwithpainfulcrisesandacutechest syndrome.
Osunkwoetal.17 6 53 Patientswithsickle-celldiseasehaveatendencytovitaminD deficiency,andresearchsuggestsanassociationbetween vitaminDdeficiencyandbonefragility.
Garridoetal.18 6 78 VitaminDdeficiencywasprevalentinchildrenwithsickle-cell diseaseinMadrid.
VanderDijsetal.22 6 18 ThevitaminDlevelsinpatientswithsickle-cellanemiain Curacaoareappropriate.
Chapelon,etal.19 6 53 Aslightdecreaseinbonemineraldensity,unrelatedtovitamin Ddeficiency,wasfoundinchildrenwithsickle-celldisease, beginningatpubertyandbeingmoremarkedamongfemales.
Buisonetal.9 6 65 LowserumlevelsofvitaminDhadahighprevalencein
childrenwithsickle-celldiseaseandwereassociatedwith seasonalvariationsanddiet.
Rovneretal.10 6 150 Theriskofindividualswithsickle-celldiseasetohavevitamin Ddeficiencywas5.3timeshigherthanthatofhealthy subjects.
Laletal.20 6 25 Childrenwithseveremanifestationsofsickle-celldiseasehave
lowbonedensity,aswellasadietpoorincalciumandvitamin D.VitaminDdeficiencywashigherinpatientswhoseweight and/orheightwerebelowaverage.
Ozenetal.21 6 50 TheresultssuggestthepotentialbenefitofvitaminD
supplementationonreducingthenumberofdayswithpainin sickle-celldisease
withsickle-cellanemia.AlthoughvitaminDdeficiencywas prevalentinthepopulation, thestudyfoundnostatistical associationbetween vitamin Ddeficiency andthenumber of painful crises and asthma.16 Osunkwo et al. assessed
53 children and adolescents with sickle-cell anemia, of which32%hadchronicpain,and42%,bonefragility.A signifi-cantassociationwasobservedbetweenvitaminDdeficiency andpainfulcrises.Thesamestudyalsofoundanassociation betweenlowvitaminDlevelsandboneweakness.17
In sickle cell anemia, the bone can be affected by microinfarctions, osteopenia, osteonecrosis, osteoporosis and osteomyelitis.25 Risk factors for the occurrence of
osteopenia in sickle-cell disease include delayed puberty and the low competence of bone mass metabolism peak,microinfarctionsresultingfromvaso-occlusiveevents, chronicpainwithimmobilization,andof theefficiencyof calcium,vitaminDandothernutrients.20,26
LowlevelsofvitaminDareassociatedwiththedecrease inmineralacquisitionbythebone.9,24Laletal.observed
sig-nificantbonedensitydeficitintheproximalendofthefemur and lumbar spine in children with severe manifestations of sickle-cell anemia. There was no correlation between theintakeofcalciumorvitaminDandbonedensity.Inthe samestudy,however,therewasastrongnegativecorrelation
betweenvitaminDvaluesandserumlevelsofalkaline phos-phatase, suggesting that vitamin D significantly affected bonemetabolisminthesepatients.20 InthestudybyOzen
et al., an insufficient intake of vitamin D was observed, whichwasmoresignificantamongpatientswithosteopenia and osteoporosis, compared to thosewithout alterations, whichdemonstratestheimportanceofadequatevitaminD intakeforthepreventionofcomorbidities.21
VitaminDsupplementation
TherearefewstudiesthataddressedvitaminD supplemen-tationinchildrenandadolescentswithsickle-cellanemia. In our review,we found only threestudies. The study by Garridoetal.,whichassessedthestatusofvitaminDin chil-drenwithsickle-cellanemiainSpain,observedthatvitamin Dlevelsinchildrenyoungerthan1yearwerebelow appro-priate levels,despite thesupplementation.The vitamin D supplementation,inthissituation,promotedavitamin defi-ciencystabilization,preventingthedevelopmentofamore severedeficiency.18
of vitamin D for a period of 6 months in 46 subjects with sickle-cell anemia, aged 7---21 years. The patients, previouslydiagnosedwithvitaminDdeficiencybyserum 25-hydroxyvitaminDmeasurements,wererandomlyassignedto receivecalciumandvitaminDsupplementationorplacebo. During the study, the recording of painful crises and the assessmentofqualityoflifescoresinthephysicaldomain wereperformed,towhichscoreswereattributedregarding thepatient’sperformanceofeverydayactivities.Theresults showed an inverse correlation between vitamin D levels and theincidence of pain,demonstrating that the higher thelevelsofvitaminD,thelowertheincidenceofpainful crises.Therewerealsopositivecorrelationsbetween vita-minDlevelsandthephysicaldomainscores,demonstrating the benefits of vitamin D for the quality of life of these patients.27
InthestudybyShamsetal.,58childrenwithsickle-cell anemiawererandomlydividedintotwogroups,oneofwhich receiveddailysupplementationof400IUofvitaminDfora periodof6monthspriortocircumcisionsurgery,whilethe othergroupreceivednointerventionbeforetheprocedure. Inthepostoperativeperiod,thegroupswereevaluatedfor theneedofanalgesia,thepresenceofpainandthe occur-renceofcomplications relatedtosickle-celldisease,such ascerebrovascularaccidentsandpainfulcrises,aswellas those unrelated to sickle-cell disease, such as fever and infection signs. Vitamin D administration was associated withalowerincidenceofpostoperativecomplications asso-ciated with sickle-cell anemia, as well as less need for analgesiapostoperatively.28
Theaforementionedstudiesbringresultsfromsmall pop-ulation samples, with the first one being a pilot study. Additionally, the second study was carried out withmale patientsonly,submittedtominorsurgery,whichresultsin limited external validity. Dueto thelow number of clini-cal trialsincluded in this review that analyzed vitamin D supplementationinchildrenandadolescentswithsickle-cell disease,thebenefitsofthissupplementationfor this pop-ulationarenotconclusiveyet,demonstratingtheneedfor furtherstudiesonthissubject.
Final
considerations
The performance of this review and the small numberof identifiedarticlesshowsthescarcityofstudiesonthe nutri-tional status of children and adolescents with sickle-cell diseaseandtheinfluenceofvitaminDontheclinical pro-fileofthesepatients.Therewerenostudiescarriedoutin Brazil. Itshould benoted thatthe review wasperformed using the keywords in Portuguese, Spanish and English, and no time limit was established. Although many stud-ies reported on the prevalence of vitamin D deficiency in children and adolescents with sickle-cell disease, its consequencesandtheeffectsofsupplementationare incon-sistent.
According to the literature, vitamin D deficiency is commoninthispopulation.Italsoshowedasignificant dif-ferenceindeficiencywhenthestudygroupwascompared withhealthysubjects.Asforcauses,theinfluenceof nutri-entintakeandhigherdietaryrequirements,seasonalityand sunexposure,ageandcommondiseasecomplications,such
asboneinfarctions,wasdemonstrated.As forthe associa-tionbetweenserumlevelsofvitaminDandcomorbidities, theresultsarestillcontroversial,showingapossible associ-ationofvitaminDdeficiencywiththeoccurrenceofpainful crises,decreasedphysicalperformanceandimpairedbone metabolism. In studies in which vitamin D and calcium supplementation intervention was performed, an associ-ation between adequate levels of vitamin D and the improvementinthepatient’squalityofliferelatedto phys-icalperformanceandreductionofcomplicationsassociated ornotwithsickle-celldiseaseandpaininthepostoperative periodwasdemonstrated.
Itcanbeconcluded,withthisreview,thatvitaminD defi-ciencyinchildrenandadolescentswithsickle-celldiseaseis frequent,andthatmorestudiesarerequiredtoprovide evi-denceoftheassociationofvitaminDdeficiencywithpainful crisesandbonemetabolism,aswellastoassessthe poten-tial therapeutic benefits of vitamin D supplementation in thispopulation.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Zago MA.Considerac¸õesGerais. In:AgênciaNacionalde Vig-ilância Sanitária,editor. Manualdediagnósticoetratamento dedoenc¸asfalciformes.Brasília:ANVISA;2002.
2.ZagoMA,PintoAC.Thepathophysiologyofsicklecelldisease: from thegeneticmutationtoultiorgan disfunction.RevBras HematolHemoter.2007;29:2007---14.
3.Fixler J, Styles L. Sickle cell disease. Pediatr Clin N Am. 2002;49:1193---210.
4.Carneiro J, Murad Y. Crescimento e Desenvolvimento. In: AgênciaNacionaldeVigilânciaSanitária,editor.Manualde diag-nósticoetratamentodedoenc¸asfalciformes.Brasília:ANVISA; 2002.p.77---82.
5.DeSouzaKC,DamiãoJJ,SiqueiraKS,dosSantosLC,dosSantos MR.Nutritionalfollow-upofchildrenwithsickle cellanemia treated in a primary care unit. Rev Paul Pediatr. 2008;26: 400---4.
6.MitchellMJ,KawchakDA,StarkLJ,ZemelBS,Ohene-Frempong K,StallingsVA.Briefreport:parentperspectivesofnutritional statusandmealtimebehaviorsinchildrenwithsicklecell dis-ease.JPediatrPsychol.2004;29:315---20.
7.KawchakDA,SchallJI,ZemelBS,Ohene-FrempongK,Stallings VA.Adequacyofdietaryintake declineswithageinchildren withsicklecelldisease.JAmDietAssoc.2007;107:843---8.
8.BuchowskiMS,TownsendDW,WilliamsR,ChenKY.Patternsand energy expenditureoffree-living physicalactivity in adoles-centswithsicklecellanemia.JPediatr.2002;140:92.
9.BuisonAM,KawchakDA,SchallJ,Ohene-FrempongK,Stallings VA,ZemelBS.LowvitaminDstatusinchildrenwithsicklecell disease.JPediatr.2004;145:622---7.
11.InstituteofMedicine(US)StandingCommitteeontheScientic EvaluationofDietaryReferenceIntakes.VitaminD.In:Institute ofMedicine(US)StandingCommitteeontheScientic Evalua-tionofDietaryReferenceIntakes,editor.Drydietaryreference intakesforcalcium,phosphorus,magnesium,vitaminDand flu-oride.Washington:NationalAcademyPress;1997.p.250---87.
12.Holick MF. TheD-lightful vitamin D for child health. JPEN J ParenterEnteralNutr.2012;36Suppl.1,9S---19S.
13.SerarslanY,KalaciA, OzkanC,Do˘gramaci Y,CoklukC,Yanat AN.Morphometryofthethoracolumbarvertebraeinsicklecell disease.JClinNeurosci.2010;17:182---6.
14.Stillwell SB, Fineout-Overholt E, MelnykBM, WilliamsonKM. Evidence-basedpractice, stepbystep:searchingforthe evi-dence.AmJNurs.2010;110:41---7.
15.GalvãoCM.Evidencehierarchies.ActaPaulEnferm.2006;19:VI.
16.JacksonTC,KraussMJ,DeBaunMR,StrunkRC,ArbeláezAM. Vitamin-Ddeficiencyandcomorbiditiesinchildrenwithsickle cellanemia.PediatrHematolOncol.2012;29:261---6.
17.Osunkwo I, Hodgman EI, Cherry K, et al. Vitamin D defi-ciencyandchronicpaininsicklecelldisease.BrJHaematol. 2011;153:529---40.
18.GarridoC,CelaE,BeléndezC,MataC,HuertaJ.Statusof vita-minDinchildrenwithsicklecelldiseaselivinginMadrid,Spain. EurJPediatr.2012;171:1793---8.
19.ChapelonE,GarabedianM,BrousseV,SouberbielleJC,Bresson JL, de Montalembert M. Osteopenia and vitamin D defi-ciency in children withsickle cell disease. Eur JHaematol. 2009;83:572---8.
20.LalA,Fung EB,Pakbaz Z,Hackney-StephensE,Vichinsky EP. Bonemineraldensityinchildrenwithsicklecellanemia.Pediatr BloodCancer.2006;47:901---6.
21.ÖzenS,ÜnalS,Erc¸etinN,Tas¸delenB.Frequencyandriskfactors ofendocrinecomplicationsinTurkishchildrenandadolescents withsicklecellanemia.TurkJHematol.2013;30:25---31.
22.VanderDijsFP,vanderKlisFR,MuskietFD,MuskietFA.Serum calciumandvitaminDstatusofpatientswithsicklecelldisease inCurac¸ao.AnnClinBiochem.1997;34:170---2.
23.Bringhurst FR, Demay MB, Kronenberg HM. Hormones and disordersof mineral metabolism.In: LarsenPR, Kronenberg HM,MelmedS,KronenbergHM,editors.Williamstextbookof endocrinology.Philadelphia:Saunders;2003.p.1318---20.
24.Barden EM, Kawchak DA, Ohene-Frempong K, Stallings VA, ZemelBS.Bodycompositioninchildrenwithsicklecelldisease. AmJClinNutr.2002;76:218---25.
25.SarraiM,DuroseauH,D’AugustineJ,MoktanS,BellevueR.Bone massdensityinadultswithsicklecelldisease.BrJHaematol. 2007;136:666---72.
26.AlmeidaA,RobertsI.Boneinvolvementinsicklecelldisease. BrJHaematol.2005;129:482---90.
27.OsunkwoI,ZieglerTR, AlvarezJ,et al.HighdosevitaminD therapyforchronicpaininchildrenandadolescentswithsickle celldisease:resultsofarandomizeddoubleblindpilotstudy. BrJHaematol.2012;159:211---5.