REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
ORIGINAL
ARTICLE
CLARIPED:
a
new
tool
for
risk
classification
in
pediatric
emergencies
Maria
Clara
de
Magalhães-Barbosa
a,∗,
Arnaldo
Prata-Barbosa
a,
Antonio
José
Ledo
Alves
da
Cunha
b,
Cláudia
de
Souza
Lopes
caInstitutoD’OrdePesquisaeEnsino(Idor),RiodeJaneiro,RJ,Brazil
bDepartamentodePediatria,FaculdadedeMedicina,UniversidadeFederaldoRiodeJaneiro(UFRJ),RiodeJaneiro,RJ,Brazil cInstitutodeMedicinaSocial(IMS),UniversidadedoEstadodoRiodeJaneiro(Uerj),RiodeJaneiro,RJ,Brazil
Received13October2015;accepted29December2015 Availableonline27June2016
KEYWORDS
Triage;
Emergencymedical services;
Pediatrics
Abstract
Objective: Topresentanewpediatricriskclassificationtool,CLARIPED,anddescribeits devel-opmentsteps.
Methods: Development steps: (i) first round of discussion among experts, first prototype; (ii)pre-testofreliability,36 hypotheticalcases;(iii) secondroundofdiscussiontoperform adjustments;(iv)teamtraining;(v)pre-testwithpatientsinrealtime;(vi)thirdroundof dis-cussiontoperformnewadjustments;(vii)finalpre-testofvalidity(20%ofmedicaltreatments infivedays).
Results: CLARIPEDfeaturesfiveurgencycategories:Red(Emergency),Orange (veryurgent), Yellow(urgent),Green(littleurgent)andBlue(noturgent).Thefirstclassificationstepincludes themeasurementoffourvitalsigns(VIPEscore);thesecondstepconsistsintheurgency dis-criminationassessment.Eachstepresultsinassigningacolor,selectingthemosturgentone forthefinalclassification.Eachcolorcorrespondstoamaximumwaitingtimeformedicalcare andreferral tothemostappropriate physicalarea for thepatient’s clinicalcondition. The interobserver agreementwassubstantial (kappa=0.79)andthefinalpre-test, with82 medi-caltreatments,showedgoodcorrelationbetweentheproportionofpatientsineachurgency categoryandthenumberofusedresources(p<0.001).
Conclusions: CLARIPEDis anobjectiveandeasy-to-usetool for simple riskclassification,of which pre-testssuggestgoodreliability andvalidity.Larger-scalestudies onitsvalidityand reliabilityindifferenthealthcontextsareongoingandcancontributetotheimplementation ofanationwidepediatricriskclassificationsystem.
©2016SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:[email protected](M.C.Magalhães-Barbosa).
http://dx.doi.org/10.1016/j.rppede.2016.02.002
PALAVRAS-CHAVE
Triagem; Servic¸osmédicos deemergência; Pediatria
CLARIPED:umnovoinstrumentoparaclassificac¸ãoderiscoememergências pediátricas
Resumo
Objetivo: Apresentarumnovoinstrumentodeclassificac¸ãoderiscopediátrico,oCLARIPED,e descreverasetapasdeseudesenvolvimento.
Métodos: Etapas do desenvolvimento:(i) primeira rodada de discussão entre especialistas, primeiroprotótipo;(ii)pré-testedeconfiabilidade,36casoshipotéticos;(iii)segundarodada dediscussãoparaajustes;(iv)treinamentodaequipe;(v)pré-testecompacientesemtempo real;(vi)terceirarodadadediscussãoparanovosajustes;(vii)pré-testefinaldevalidade(20% dosatendimentosdecincodias).
Resultados: O CLARIPED apresenta cinco categorias de urgência: Vermelha (emergência), Laranja (muitourgente), Amarela (urgente), Verde(poucourgente) eAzul (sem urgência). A primeira etapa da classificac¸ão inclui a aferic¸ão de quatro sinais vitais (escoreVIPE); a segunda etapaconsistenaavaliac¸ãodediscriminadores deurgência.Cada etaparesulta na atribuic¸ãodeumacor,selecionando-seademaiorurgênciaparaaclassificac¸ãofinal.Cadacor correspondeaumtempomáximodeesperapeloatendimentomédicoeaoencaminhamentoà áreafísicamaisadequadaàcondic¸ãoclínicadopaciente.Aconcordânciainterobservadorfoi substancial(kappa=0,79)eopré-testefinal,com82atendimentos,evidenciouboacorrelac¸ão entreaproporc¸ãodepacientesemcadacategoriadeurgênciaeonúmeroderecursosusados (p<0,001).
Conclusões: OCLARIPEDéuminstrumentoparaclassificac¸ãoderiscosimples,objetivoede fácil uso,cujospré-testessugerem boaconfiabilidadeevalidade. Estudosem maiorescala sobresuavalidadeeconfiabilidadeemdiferentescontextosdesaúdeestãoemcursoepodem contribuirparaaadoc¸ãodeumsistemadeclassificac¸ãoderiscopediátricoemâmbitonacional. ©2016SociedadedePediatriadeS˜aoPaulo. PublicadoporElsevier EditoraLtda.Este ´eum artigoOpenAccesssobumalicenc¸aCCBY(http://creativecommons.org/licenses/by/4.0/).
Introduction
Inthe lasttwodecades,amajorchallengein healthcare hasbeentofindsolutionstotheincreasedovercrowdingin emergencyservicehospitals.Oneofthestrategiesadopted inmanycountriestodealwiththisproblemwasthe imple-mentationoftriagesystemsusedtoclassifyeachpatient’s degree of clinical urgency shortly afterhis/her arrival to theEmergencyDepartment(ED),establishingawaitinglist basedonclinicalrisk,andnotinorderofarrival,toundergo medicalevaluationandtreatment.
The Australian Triage Scale (ATS), Canadian Triage & AcuityScale (CTAS),ManchesterTriageSystem (MTS),and EmergencySeverity Index(ESI) arethe tools for triagein emergencyservicesmostusedworldwide,allwithfivelevels ofurgency.1,2
In Brazil, the risk classification system developed by the Ministry of Health in the Qualisus Program has only fouremergencycategories,doesnotaddress thepediatric grouppeculiarities,andhasnotachievedsignificantnational adherence.3,4Ontheotherhand,thosedevelopedinEurope,
North America, andAustralia arecomplex,which hinders large-scaleadoptionina heterogeneoushealth contextas theBrazilian.Moreover,thereareinsufficientliteratureon thevalidityandreliabilityofthepediatricversionsofthese triagesystems.
Theaimofthisstudyistopresentanewriskclassification tool,theCLARIPED,forpediatricemergenciesanddescribe the steps of its development. The intent is to obtain a
reliableand validtool thatis best suitedtothe Brazilian healthcontext.
Method
chartsreview.ThestudywasapprovedbytheInstitutional Review Board of the Instituto D’Or de Pesquisa e Ensino (IDOR),underthenumber209075/2013.
Results
A group of experts (three doctors and two nurses) with extensiveexperiencein pediatricemergencieswas assem-bledinordertochooseandtestariskclassificationtoolfor thepediatricemergencydepartment.Afterextensive liter-aturereview,itwasconcludedthatthefourtriagesystems designedinNorthAmerica(CTASandESI),UnitedKingdom (MTS),andAustralia (ATS)werenotsuitablefor our coun-try,astheyareextensive,complexorlackspecific-pediatric features.TheSouthAfrican TriageScale (SATS),5 although
simplerandmoreadaptabletotheBrazilianhealthcontext, onlyhadfourlevelsofurgency,insufficientstratificationof pediatricagegroups,inadditiontohavingfewstudiesofits useinchildren.Itwasdecided,therefore,todesignanew triagesystemspecificforpediatricemergencies.
TheCLARIPEDsystem
CLARIPED comprises five urgency categories: Red (immi-nent life threat), Orange (very urgent), Yellow (urgent), Green(littleurgent)andBlue(noturgent). Eachcategory isassignedamaximumwaitingtimeformedicalevaluation andreferraltoanappropriateserviceareaofadequatecare tothepatient’slevelofurgency,asfollows:red,immediate careintheressucitationroom;orange,carewithin10minin theobservationroom;yellow,upto30min,waitingroom;
green,upto90min,waitingroom;andblue,upto180min, waitingroom.Theriskclassificationshouldstartina max-imumof 10min after patient’s arrival and registration; it shouldbeperformedbyanurseandlast2---5min.
Thefirststepstartswithsixquestionsaboutcomplaints, drugallergies,regular pediatric care, associated morbidi-ties,usingmedicationsand lastmeasured weight.Nextis theevaluationoffourvitalsigns:respiratoryrate(RR),heart rate(HR), oxygensaturation(SpO2),andskintemperature
(Temp).Eachvitalsignmeasuredisassignedavaluefrom0 to4,which willcomposethePediatricVitalSignals(VIPE) scorethatrangesfrom0to12,consistingofthesumofthe firstthreeparametersvaluessubtractedfromthe temper-aturevalueincaseof increasedHR(RR+HR+SpO2-Temp,if
increasedHR).TheVIPEscoreshouldthenbeassociatedwith oneof fivecolors: score 0=Blue; 1---2=Green; 3---5=Yellow; 6---9=Orange;≥10=Red(Table1).
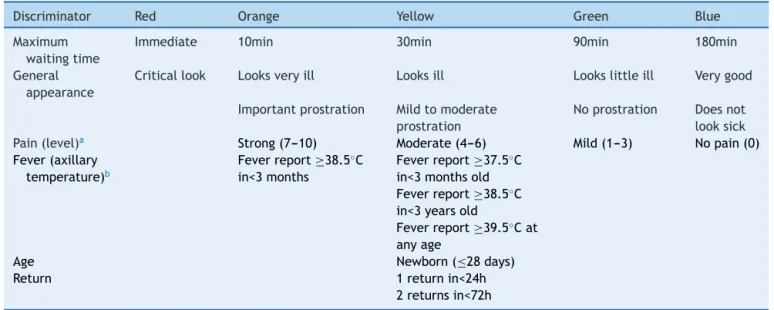
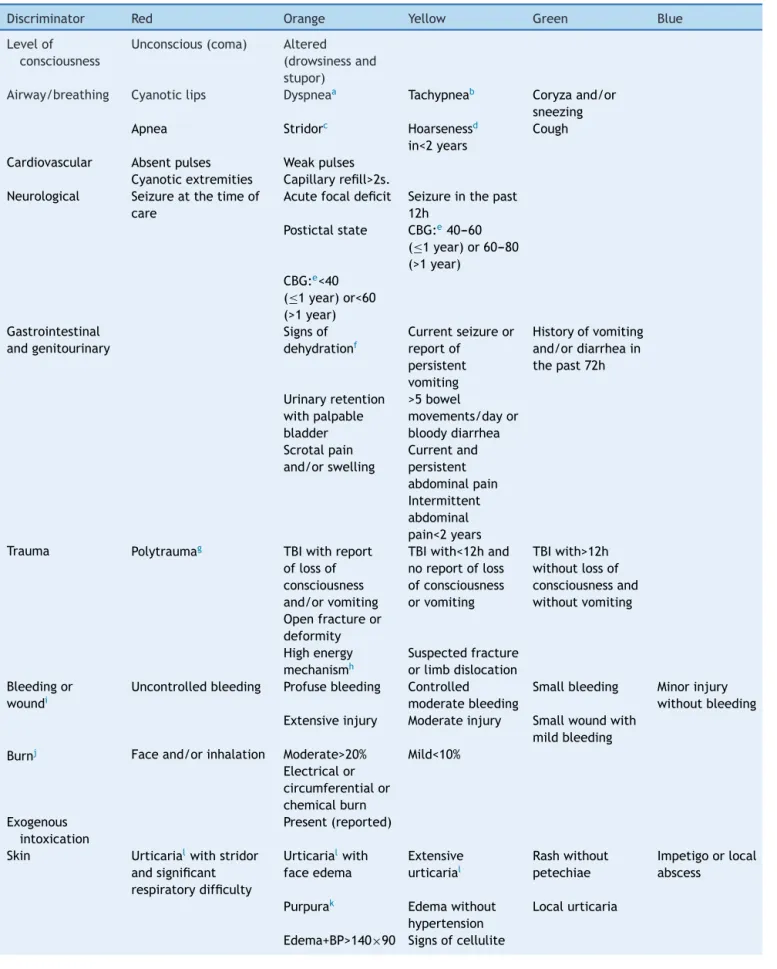
The second stepis toconsult the tablesof discrimina-tors categorized by type or organ system involved (lines) and by urgency levels (columns). Assessment of five gen-eraldiscriminators(pain,generalappearance,feverreport, age, and return to the ED) is mandatory for all patients (Table2). The other discriminators are evaluated accord-ingtothepatient’scomplaint(Table3).Itisnotnecessary toconsultall linesandcolumns ofthe second table,only therelevantlinesassociatedwiththereportedcomplaints andthecolumnscorrespondingtolevelsofurgencyhigher thantheassignedbytheVIPEscore.Ifthereisa discrimi-natorcorrespondingtoahigherlevelofurgencythanthat assignedbytheVIPEscore,thehigherlevelofurgencywill
determinethefinalclassification.Theurgencydetermined bytheVIPEscoremaynotbedecreased,onlyincreasedfrom theevaluationofthediscriminators.
Inthe presence ofdiscriminators indicating risk of life threatening,suchassseizures,impairedlevelof conscious-ness,apnea,cyanosis,andothers,thepatientmustbesent for rapid or immediatemedical care before any adminis-trative procedure. The risk classification process is then performedretrospectively.
Pre-teststudies
Thehypotheticalclinicalscenariosdesignedbyexpertsfor training had the following distribution of urgency levels: Red11%,Orange42%,Yellow31%,Green8%,andBlue8%. Theoverallkappaformultipleobserversresultingfromthe firstpre-testwith36hypotheticalclinicalscenarioswas0.79 andkappaforeachurgencycategory was0.93(Red);0.82 (Orange);0.73(Yellow);0.65(Green),and0.93(Blue),with astandarddeviationof0.03andp<0.001,whichrepresented substantialreliability.
The second pre-test, performed with patients in real time, determined changes for the treshholds and values attributedtothephysiologicalparametersandforsome dis-criminators(newborn,returninlessthan24h,feverreport, abdominalpain,andcranialtrauma).
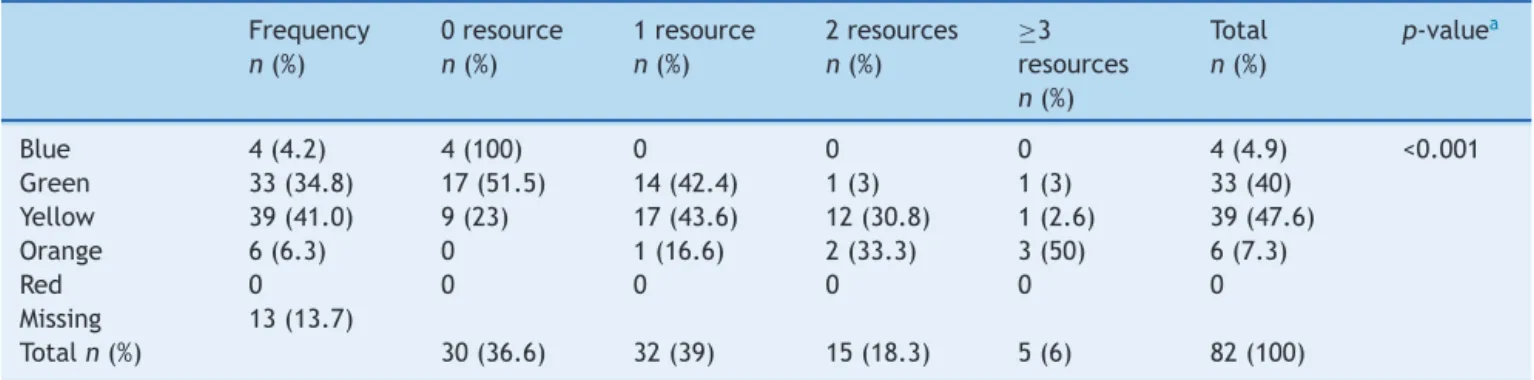
The final validity pre-test, included the retrospective analysisof95medicalcharts,selectedbyasystematic samp-ling of 20%of the cases attendedin thefirst fivedays of December2013. The aimwastoevaluate thedistribution ofthelevelsofurgencyandtheirassociationwithan out-come, which could work as a proxy of urgency, such as the numberofdiagnostic andtherapeutic resourcesused. The distributionofthelevelsofurgencywas: Blue(4.2%); Green(34.7%);Yellow(41%);Orange(6.3%),andRed(0%). NoneoftheattendancesclassifiedasBlueusedadiagnostic and/ortherapeuticresourceintheemergencydepartment; onethirdoftheGreenattendances,halfoftheYellowones usedoneresourceand20%usedtwoormoreresources;over 80%oftheOrangeonesusedtwoormoreresources(Table4;
p<0.001).
Discussion
The proposal todevelop asimple, objective, andeasy to use tool for risk classification in pediatric emergencies, appropriate toa Brazilian health context, resulted in the CLARIPED.Brazil’scontinentalmagnitudeand heterogene-ity make it difficult to adopt a risk classification system nationwide. The option to develop a new instrument, insteadofusingother triagesystemsalreadyevaluated, is justified. The most commonly used systems in the world weredevelopedincountriesinNorthAmerica,6,7 Europe,8
andAustralia.9Thehealthcontextofthesecountriesisquite
Table1 VIPEscorecalculation(vitalsignsinPediatrics).
Newbornto2monthsold
4 2 1 0 2 3 4
RR <16 16---19 20---29 30---60 61---80 81---90 >90 HR <81 81---90 91---110 111---149 150---179 180---189 >189 SpO2 <90 90---92 93---94 95---100
3monthsto11monthsold
4 2 1 0 2 3 4
RR <16 16---19 20---24 25---50 51---70 71---80 >80 HR <71 71---80 81---100 101---139 140---169 170---179 >179 SpO2 <90 90---92 93---94 95---100
1yearto4yearsold
4 2 1 0 2 3 4
RR <13 13---15 16---19 20---40 41---60 61---70 >70 HR <61 61---70 71---90 91---119 120---149 150---169 >169 SpO2 <90 90---92 93---94 95---100
5yearsto12yearsold
4 2 1 0 2 3 4
RR <11 11---14 15---17 18---24 25---36 37---50 >50 HR <51 50---60 61---70 71---109 110---129 130---149 >149 SpO2 <90 90---92 93---94 95---100
>12years
4 2 1 0 2 3 4
RR <10 10 11 12---16 17---22 23---29 >29 HR <41 41---50 51---60 61---99 100---119 120---139 >139 SpO2 <90 90---92 93---94 95---100
Assessmentofaxillarytemperature(regardlessofage) IfHRisincreased(score2,3or4)Subtract:
0 −1 −2
AxT 36---37.4 37.5---38.5 >38.5
VIPEscore(0---12)isthesumofthepointsassignedtoeachvitalsign.However,ifheartrateisincreased(score2,3or4);−1shouldbe subtractedfromthefinalscoreiftheaxillarytemperatureisbetween37.5and38.5◦Cand
−2iftheaxillarytemperature(AxT)is>38.5◦C. Urgencyclassification:Blue(0),Green(1---2),Yellow(3---5),Orange(6---9),andRed(≥10).
Table2 CLARIPEDgeneralandmandatorydiscriminators.
Discriminator Red Orange Yellow Green Blue Maximum
waitingtime
Immediate 10min 30min 90min 180min General
appearance
Criticallook Looksveryill Looksill Lookslittleill Verygood Importantprostration Mildtomoderate
prostration
Noprostration Doesnot looksick Pain(level)a Strong(7---10) Moderate(4---6) Mild(1---3) Nopain(0)
Fever(axillary temperature)b
Feverreport≥38.5◦C
in<3months
Feverreport≥37.5◦C
in<3monthsold Feverreport≥38.5◦C
in<3yearsold
Feverreport≥39.5◦Cat
anyage
Age Newborn(≤28days)
Return 1returnin<24h
2returnsin<72h
a Thelevelofpainshouldbeevaluatedbyappropriatescalesforthepatient’sage,suchasFLACCScaleorFacesScale(<5years)and
VisualAnalogicScale(>5years).
Table3 CLARIPEDdiscriminatorsaccordingtoreportedcomplaints.
Discriminator Red Orange Yellow Green Blue Levelof
consciousness
Unconscious(coma) Altered (drowsinessand stupor)
Airway/breathing Cyanoticlips Dyspneaa Tachypneab Coryzaand/or
sneezing Apnea Stridorc Hoarsenessd
in<2years
Cough
Cardiovascular Absentpulses Weakpulses Cyanoticextremities Capillaryrefill>2s. Neurological Seizureatthetimeof
care
Acutefocaldeficit Seizureinthepast 12h
Postictalstate CBG:e40---60
(≤1year)or60---80
(>1year) CBG:e<40
(≤1year)or<60
(>1year) Gastrointestinal
andgenitourinary
Signsof dehydrationf
Currentseizureor reportof
persistent vomiting
Historyofvomiting and/ordiarrheain thepast72h
Urinaryretention withpalpable bladder
>5bowel
movements/dayor bloodydiarrhea Scrotalpain
and/orswelling
Currentand persistent abdominalpain Intermittent abdominal pain<2years Trauma Polytraumag TBIwithreport
oflossof consciousness and/orvomiting
TBIwith<12hand noreportofloss ofconsciousness orvomiting
TBIwith>12h withoutlossof consciousnessand withoutvomiting Openfractureor
deformity Highenergy mechanismh
Suspectedfracture orlimbdislocation Bleedingor
woundi
Uncontrolledbleeding Profusebleeding Controlled moderatebleeding
Smallbleeding Minorinjury withoutbleeding Extensiveinjury Moderateinjury Smallwoundwith
mildbleeding Burnj Faceand/orinhalation Moderate>20% Mild<10%
Electricalor circumferentialor chemicalburn Exogenous
intoxication
Present(reported)
Skin Urticarialwithstridor
andsignificant respiratorydifficulty
Urticarialwith
faceedema
Extensive urticarial
Rashwithout petechiae
Impetigoorlocal abscess
Purpurak Edemawithout
hypertension
Localurticaria
Table3 (Continued)
Discriminator Red Orange Yellow Green Blue Locomotor Claudication+fever
Acutegaitdisorder Foreignbody Present
Unspecific Unabletostand Inconsolablecrying Behaviorchange Irritability
Suspectedabuse Comorbidities Diabetes,withsevere
hypoglycemia (CBG<20)e
Diabeteswith hypo-orhyperglycemia: CBGe<60or>400
DiabeteswithCBGe
between250and400
Immunosuppression withfever
Neuromuscular diseasesm
Immunosuppressionn
withoutfever Suspecteddengue
(alwaysmeasure BPolyingand
sitting)
Signsofshock Presenceofwarning signsp
Absenceofwarning signsp
Signsofrespiratory failure
a Dyspnea:respiratorydistresswithpresenceofintercostalretractions. b Tachypnea:increasedRRaccordingtotheVIPEtable(RRscore>0).
c Stridor:noiseduringinspirationwithvaryingdegreesofrespiratorydistress. d Hoarseness:hoarsecryorvoiceorcough,withoutstridororrespiratorydistress.
e Capillarybloodglucose(CBGmg/dL):performthetestinallpatientswithalteredlevelofconsciousness,recentorcurrentseizure,
lethargyorprevioushistoryofdiabetes.
f Signsofdehydration:drymouth,sunkeneyes,noturinatinginthelast12h,decreasedskinturgor. g Polytrauma:patientswithtraumaticinjuryintwoormoreorgans.
h Highenergymechanism(intheabsenceofinformation,consideranytrafficaccidentashighenergymechanism):(a)motorvehicle
accident>60km/h(beltcollision);>40km/h(unbeltedcollision);>30km/h(motorcycle),and>10km/h(runover);(b)afallfromhigher than1m.
i Wound:(a)mild: abrasionsand contusionsrequiring nosuture; (b)moderate: contusionsrequiring sutures,butwithcontrolled
bleeding;(c)severe:extensivecontusionsrequiringsutures,profuseandcontinuousbleeding.
j Burn:Ruleofnines.
k Purpura:presenceofpetechiaand/orecchymosis.
l Urticaria:unlikeotherskinrashes;hyperemiaandelevatedplaques,usuallyveryitchy,butnotalways. m Neuromusculardiseases:chronicencephalopathy,myopathy,myelomeningocele,hydrocephalus.
n Immunosuppression:afterchemotherapy,nephroticsyndromeinactivity,chronicuseofcorticosteroids.
o Bloodpressure(BP):Alwaysmeasureincaseofalteredlevelofconsciousness,recentorcurrentseizure,suspecteddenguefever,
edemaofthelowerlimbsorgeneralized(anasarca).
p Warning signs in dengue (presence of one or more signs): abdominal pain, persistent vomiting, respiratory distress, postural
hypotensionordizziness,drowsiness,and/orirritability,spontaneousbleeding,decreasedurineoutput,suddendropintemperature, hypothermia,edema.
Table4 Pilotpre-testofvalidity:useoftreatmentresourcesinaccordancewiththelevelofriskclassification. Frequency
n(%)
0resource
n(%)
1resource
n(%)
2resources
n(%)
≥3
resources
n(%)
Total
n(%)
p-valuea
Blue 4(4.2) 4(100) 0 0 0 4(4.9) <0.001 Green 33(34.8) 17(51.5) 14(42.4) 1(3) 1(3) 33(40)
Yellow 39(41.0) 9(23) 17(43.6) 12(30.8) 1(2.6) 39(47.6) Orange 6(6.3) 0 1(16.6) 2(33.3) 3(50) 6(7.3)
Red 0 0 0 0 0 0
Missing 13(13.7)
Totaln(%) 30(36.6) 32(39) 15(18.3) 5(6) 82(100)
thecountryasSouthAfricanTriageScale(SATS). CLAR-IPEDkeptthetwo-stepslogisticsoftheSATStriageprocess, consisting of mesurement of physiological parameters, followedbyassessmentofdiscriminators.However,several modificationswereperformedinbothstepsandaredetailed below.
AlthoughSATShasfivecolors,strictlyspeakingithasonly fourlevelsofurgency,astheBlueleveldoesnotreferto non-urgentpatients,buttopatientswhoaredeadonarrival.In theBrazilianhealthcontext,thereisalargeinfluxof outpa-tientstotheemergencyservices.3,4Thus,theexistenceof
alevelfornon-urgentpatientsisjustified,similartoother systemssuchastheMTS,8ESI-4,6PaedCTAS,7andATS.9The
triagetoolswithfiveemergencycategories showedhigher reliabilityandvaliditythantoolswithfewercategories.13
InCLARIPED,weoptedforthestratificationintofiveage groups,insteadofthethreegroupsusedbySATS.Thisoption isinagreementwiththevitalsignstablesrecommendedby pediatric textbooks14,15 and other triage instruments that
usefourormoreagegroups.6,7However,thereisalackof
studiesthatvalidatethestratificationofagegroupsforvital signsinPediatrics.TheBedsidePediatricEarlyWarning Sys-temScore---BedsidePEWSScore),atooldesignedtodetect early clinical deterioration of hospitalized children, was derivedfromstatisticalmethods andrecentlyvalidated.16
ThestratificationintofiveagegroupsofCLARIPEDwasbased onBedsidePEWSScore.
Althoughthereisnotyetaninternationalconsensuson theparameterstobeincludedinatriagetool,thereis evi-dencethatvitalsignsshouldbeanintegralpartofasafety risk classification process, particularly in children.5,17,18
However,vitalsignmeasurementscanbeextremelydifficult inemergencyscenarios,particularlyinsmallor uncoopera-tivechildren.Selectingthemostobjectiveparametersthat represent an effective contribution to the discrimination of emergency is crucial toachieve the goals of timeand processimprovement.InSATS,thefirststepincludes eval-uationofsevenparameters:RR,HR,systolicbloodpressure (SBP),Temp,levelofconsciousness,mobility,andpresence oftrauma.The pediatricrevised versionofSATS excluded theSBPassessment.ThePaedCTAS7recommendsthe
mea-surementofHR,RR,andSpO2asfirstordermodifiers,while
theESI-46recommendsthemeasurementofthesamethree
vitalsignsonlyincertaincircumstances.TheATS19leavesat
thediscretionofthetriageprofessionaltheneed to mea-surevitalsigns. InCLARIPED, thefourselectedvitalsigns andthescoreassignedtoeachofthemarebasedonstudies addressingthe developmentof twoinstrumentsthat used statisticalmethodstoassesstheabilityofsome physiolog-icalparameterstopredict clinical outcomes:the Bedside Pews16andPediatricEmergencyAssessmentTool(PEAT),20a
multivariatemodeltopredictthreelevelsofcarerequired forpediatricpatientsintheemergencydepartment.
TheinclusionofSpO2inVIPEscorewasbasednotonlyon
useofthisparameterinothervalidatedinstruments,suchas theESI-4,6 PaedCTAS,7 andBedsidePewsScore,16 but also
onevidence that patients withlow SpO2 usually have no
increasedrespiratory rate and that itsmeasurement may generatesignificantchangesinthemanagementofanumber ofpatientsattendedatpediatricemergencyservices.21,22
Theexclusionofblood pressuremeasurementfromthe VIPE score wasbased on evidence that the benefitof its
mandatory assessment in pediatric patients in the emer-gency department is limited.23 On onehand, hypotension
is a late sign of shock in children and, on the other hand,thetriageofchildrenwithhypertensioninthe emer-gency department may result in high prevalence of false positives.24 Other triage tools,such asMTS,8 PaedCTAS,7
ESI-4,6 andATS,19 donotincludemandatorymeasurement
ofbloodpressure,butonlytheinitialassessmentofclinical signsofshock,suchasthinpulses,delayedcapillaryrefill, sweating,andpallor.
HRcorrectedbythedegreeoffeverisauniqueaspectof CLARIPEDandwasbasedonthefactthattachycardiaisone ofthesystemicinflammatoryresponsesyndrome(SIRS)and sepsisparameters.25 Arecentstudyproposesasimilar
cor-rectionintheevaluationofchildrenwithacuteinfection.26
Noothertriagesystemconsidersthiscorrection.The assess-ment of the degree of fever is further considered in the discriminatorsstep,accordingtoageandfollowsthe guide-lines of the American College of Emergency Physicians.27
However,unlikeothertriagesystems,CLARIPEDtakesinto accountnotonlythecurrentfever,butthereportoffever inthelast24h.
In CLARIPED, the evaluation of patient’s level of con-sciousnessandpresenceoftraumaweremovedtothestep of discriminators assessment. Instead of considering the involvementofthepatient’slevelofconsciousnessintofour categories(awake,responsetopain,responsetovoice,and non-responsive),asrecommendedinSATS,11CLARIPED
con-sidersthatthepresenceofanyimpairmentofconsciousness placesthe patientat theOrangelevel (veryurgent).This strategy is already used in MTS,8 ESI-4,6 PaedCTAS,7 and
ATS.19
InCLARIPED,traumaisassessednotonlyforitspresence orabsence,asrecommendedinSATS,butaccordingtothe aspectsofmechanism,extension,locationandpresenceof symptoms.Themechanismandtraumaseverityassessment isalsousedinotherinstruments.PaedCTAS7andATS19assess
the presence of a high energy mechanism, regardless of clinical symptoms,toclassifypatients intohigherurgency categories.InMTS,8 thereisaspecificflowchartformajor
traumainwhichpatientsareclassifiedinemergencylevels one,two,oratleastthree,dependingonclinical manifes-tations.
Finally, the table of discriminators used in the second stepofCLARIPEDisverydifferentfromthatusedinSATS,in termsofcontentandorganization.AsinPaedCTAS,7
discrim-inators aregroupedby organsystems.The Canadiantool, however, is much more extensive and complex, covering 167complaintsgroupedinto17organsystems.
A recent study of the SATS5 demonstrated that in
pediatric triage the combination of the two steps, the evaluation of physiological parameters followed by the assessment of clinicaldiscriminators, increasedsensitivity (91%), compared with the use of each step alone (57.1% and75.6%,respectively).InCLARIPED,itisconsideredthat theVIPEscorecalculationhasalowerweightinthetool’s sensitivity, although this hypothesis has not been tested yet.
Thefinalpre-testwithasampleof82attendancesfounda distributionofemergenciessimilartootherstudies.28---30The
Some limitationsmaybeidentifiedin thedevelopment oftheCLARIPEDsystem.Thefirstreferstothemethodology forconsensusontheproposedmodificationsandthechoice andorganizationofdiscriminators.ADelphimethod assur-ing the participating experts anonymity, interaction with controlled feedback, and statistical analysis of responses tosuccessiveroundsofinteractionwouldbethepreferred methodtominimizebiasand noiseandensure the preva-lence of the majority opinion. On the other hand, the tooldevelopmentprocessinseveralstepsensuredthe pro-cess systematization and a broad participation of the ED professionalsin thedevelopmentandimprovementof the instrument up to its last version. The second limitation relatesto the use of CLARIPED in other health care sett-ings.Itcanbearguedthatthespecificcontextinwhichthe CLARIPED was conceived limitsits application elsewhere. Morespecificdiscriminatorsrelatedtoophthalmologicalor psychiatricemergencies,for example,areabsentin CLAR-IPED.However,thesearchforthesimplicity,objectivity,and trainingfacility oftheinstrumentcanmakeitsadaptation anddisseminationviable inother less developedBrazilian regions by including more comprehensive and/or specific discriminators suitable to different settings. The concern in refining the discrimination between intermediate lev-els of urgency (Yellow [urgent] vs. Green [little urgent]) alsomakesthetool theoreticallyapplicable to intermedi-ateandlowurgencycareservices.Howevertheinstrument is not suitablefor pre-hospitaltriageduring criticalmass events.Specificinstrumentsfocusingontriageofcritically illpatientsinnon-hospitalsettingsareneededforthis pur-pose.
Itcan beconcludedthatthedevelopmentofCLARIPED for risk classification in pediatric emergenciesresulted in asimple,objective,andeasytousetool,whose pre-tests suggestagoodreliabilityandvalidity.Larger-scalestudies ofitsvalidity,reliability,andapplicationindifferenthealth contextsareunderway andmaycontributetotheuseofa pediatricriskclassificationsystemnationwide.
Funding
CNPq(Conselho Nacionalde Desenvolvimento Científico e Tecnológico, REF. No.: 448855/2014-3). Faperj (Fundac¸ão CarlosChagasFilhodeAmparoàPesquisadoEstadodoRio deJaneiro,REF.No.:E-26/010.000196/2015).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Christ M,Grossmann F,Winter D,Bingisser R, PlatzE. Mod-erntriage inthe emergency department. Dtsch Arztebl Int. 2010;107:892---8.
2.FarrohkniaN,CastrénM,EhrenbergA,LindL,OredssonS, Jon-ssonH, etal.Emergency departmenttriagescalesand their components:a systematic reviewof thescientific evidence. ScandJTraumaResuscEmergMed.2011;19:42.
3.O’DwyerG,MattaIE,PepeVL.Avaliac¸ãodosservic¸os hospita-laresdeemergênciadoEstadodoRiodeJaneiro.CiencSaude Colet.2008;13:1637---48.
4.O’DwyerGO,OliveiraSP,SetaMH.Avaliac¸ãodosservic¸os hos-pitalaresde emergência doprograma QualiSUS.CiencSaude Colet.2009;14:1881---90.
5.TwomeyM,CheemaB,BuysH,CohenK,deSaA,LouwP,etal. Vitalsignsforchildrenattriage:amulticentrevalidationofthe revisedSouthAfricanTriageScale(SATS)forchildren.SAfrMed J.2013;103:304---8.
6.GilboyN,TanabeP,TraversDA.Theemergencyseverityindex version4:changestoESIlevel1andpediatricfevercriteria.J EmergNurs.2005;31:357---62.
7.WarrenDW,JarvisA,LeBlancL,GravelJ,CTASNational Work-ingGroup;CanadianAssociationofEmergency.Revisionstothe Canadiantriageandacuityscalepaediatricguidelines (PaedC-TAS).CJEM.2008;10:224---43.
8.Mackway-JonesKMJ,WindleJ.Emergencytriage.Manchester TriageGroup.2nded.Oxford:BlackwellPublishing,BMJBooks; 2006.
9.ConsidineJ,LeVasseurSA,CharlesA.Developmentof physio-logicaldiscriminatorsfortheAustralasianTriageScale.Accid EmergNurs.2002;10:221---34.
10.GottschalkSB,WoodD,DeVriesS,WallisLA,BruijnsS, Cape TriageGroup.TheCapetriagescore:anewtriagesystemSouth Africa. Proposal from the Capetriage group. Emerg Med J. 2006;23:149---53.
11.Wallis LA. The Cape triage score: update. Emerg Med J. 2006;23:740.
12.BruijnsSR,WallisLA,BurchVC.Effectofintroductionofnurse triageonwaitingtimesinaSouthAfricanemergency depart-ment.EmergMedJ.2008;25:395---7.
13.TraversDA,WallerAE,BowlingJM,FlowersD,TintinalliJ. Five-leveltriagesystemmoreeffectivethanthree-levelintertiary emergencydepartment.JEmergNurs.2002;28:395---400. 14.BehrmanRE,KliegmanRM,JensonHB.Nelsontextbookof
pedi-atrics.16a
ed.Philadelphia:Saunders;2011.
15.Marx J. Rosen’s emergency medicine: concepts and clinical practice.8aed.Philadelphia:Saunders;2013.
16.ParshuramCS,HutchisonJ,MiddaughK.Developmentand ini-tialvalidationoftheBedsidepaediatricearlywarningsystem score.CritCare.2009;13:R135.
17.AdsheadN,ThomsonR.Useofapaediatricearlywarningsystem inemergencydepartments.EmergNurse.2009;17:22---5. 18.BainsHS,SoniRK.AsimpleclinicalscoreTOPRStopredict
out-comeinpediatricemergencydepartmentinateachinghospital inIndia.IranJPediatr.2012;22:97---101.
19.Australian Government. Department of health and ageing. Emergencytriageeducationkit.Canberra:Commonwealthof Australia;2007.
20.GorelickMH,LeeC,CronanK,KostS,PalmerK.Pediatric emer-gencyassessmenttool(PEAT):arisk-adjustmentmeasure for pediatricemergencypatients.AcadEmergMed.2001;8:156---62. 21.MowerWR,SachsC,NicklinEL,SafaP,BaraffLJ.A compari-sonofpulseoximetryandrespiratoryrateinpatientscreening. RespirMed.1996;90:593---9.
22.MowerWR,SachsC,NicklinEL,SafaP,BaraffLJ.Effectof rou-tineemergencydepartmenttriagepulseoximetryscreeningon medicalmanagement.Chest.1995;108:1297---302.
23.PoorKM,DucklowTB.BenefitofBPmeasurementinpediatric EDpatients.ISRNNurs.2012;2012:627354.
24.RickeTL,HendryPL,KalynychC,BuzaianuEM,KumarV, Red-field C. Incidence and recognition of elevated triage blood pressureinthepediatricemergencydepartment.PediatrEmerg Care.2011;27:922---7.
26.Thompson M,HarndenA,PereraR,Mayon-White R,Smith L, McLeod D, et al. Deriving temperatureand ageappropriate heartratecentilesforchildrenwithacuteinfections.ArchDis Child.2009;94:361---5.
27.Autorianãoreferida.Clinicalpolicyforchildrenyoungerthan threeyearspresentingtotheemergencydepartmentwithfever. AnnEmergMed.2003;42:530---45.
28.Ma W, Gafni A, Goldman RD. Correlation of the Canadian Pediatric Emergency Triage and Acuity Scale to EDresource utilization.AmJEmergMed.2008;26:893---7.
29.GreenNA,DuraniY,BrecherD,DePieroA,LoiselleJ,AttiaM. Emergencyseverityindexversion4:avalidandreliabletoolin pediatricemergency departmenttriage.PediatrEmerg Care. 2012;28:753---7.