www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
REVIEW
ARTICLE
Use
of
a
monitoring
tool
for
growth
and
development
in
Brazilian
children
---
systematic
review
Ana
Claudia
de
Almeida
a,∗,
Larissa
da
Costa
Mendes
b,
Izabela
Rocha
Sad
a,
Eloane
Gonc
¸alves
Ramos
a,
Vânia
Matos
Fonseca
a,
Maria
Virginia
Marques
Peixoto
aaInstitutoNacionaldeSaúdedaMulher,daCrianc¸aedoAdolescenteFernandesFigueira(IFF/Fiocruz),RiodeJaneiro,RJ,Brazil bOrganizac¸ãoNãoGovernamentalCasadaÁrvore,RiodeJaneiro,RJ,Brazil
Received1April2015;accepted24June2015 Availableonline29December2015
KEYWORDS
Children’shealth; Growthand development; Development; Childcare
Abstract
Objective: ToassesstheuseofahealthmonitoringtoolinBrazilianchildren,withemphasis onthevariablesrelatedtogrowthanddevelopment,whicharecrucialaspectsofchildhealth care.
Datasource: A systematicreview ofthe literaturewas carried outinstudies performedin Brazil,usingtheCochraneBrazil,Lilacs,SciELOandMedlinedatabases.Thedescriptorsand key-wordsusedwere‘‘growthanddevelopment’’,‘‘childdevelopment’’,‘‘childhealthrecord’’, ‘‘childhealthhandbook’’,‘‘healthrecordandchild’’and‘‘childhandbook’’,aswellasthe equivalenttermsinPortuguese.Studieswerescreenedbytitleandsummaryandthose consid-eredeligiblewerereadinfull.
Datasynthesis: Sixty-eight articles were identifiedand eight articles were includedin the review,astheycarriedoutaquantitativeanalysisofthefillingoutofinformation.Fivestudies assessedthecompletionoftheChild’sHealthRecordandthreeoftheChild’sHealthHandbook. Allarticlesconcludedthattheinformationwasnotproperlyrecorded.Growthmonitoringcharts wererarelyfilledout,reaching96.3%inthecaseofweightforage.TheuseoftheBMIchart wasnotreported,despitethegrowingratesofchildhoodobesity.Onlytwo studiesreported the completionofdevelopment milestonesand, in these,themilestones were recordedin approximately20%oftheverifiedtools.
Conclusions: The results ofthe assessed articles disclosed underutilization ofthe tool and reflectlowawareness byhealth professionalsregardingtherecordingofinformationinthe child’shealthmonitoringdocument.
©2015SociedadedePediatriadeSãoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(https://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:[email protected](A.C.Almeida).
http://dx.doi.org/10.1016/j.rppede.2015.12.002
PALAVRAS-CHAVE
Saúdedacrianc¸a; Crescimentoe desenvolvimento; Desenvolvimento; Cuidadodacrianc¸a
Usodeinstrumentodeacompanhamentodocrescimentoedesenvolvimento
dacrianc¸anoBrasil---Revisãosistemáticadeliteratura
Resumo
Objetivo: Avaliarousodeinstrumentodeacompanhamentodesaúdedacrianc¸a,comênfase nas variáveis do acompanhamento do crescimento e do desenvolvimento, eixo central do cuidadoàsaúdeinfantil.
Fontesdosdados: Feita revisão sistemáticadaliteratura deestudos noBrasil nas basesde dados Cochrane Brasil,Lilacs, SciELOe Medline.Os descritorese aspalavras-chave usadas foram‘‘crescimentoedesenvolvimento’’,‘‘desenvolvimentoinfantil’’,‘‘cartãodacrianc¸a’’, ‘‘cadernetadesaúdedacrianc¸a’’,‘‘cartãoecrianc¸a’’e‘‘cadernetadacrianc¸a’’.Osestudos foram rastreados por título e resumo e foi feitaa leitura completa daqueles considerados elegíveis.
Síntesedosdados: Foramidentificados68artigoseoitoforamincluídosnoestudoporfazera análisequantitativadopreenchimento.CincoestudosavaliaramopreenchimentodoCartãoda Crianc¸aetrêsdaCadernetadeSaúdedaCrianc¸a.Todososartigosconcluíramqueasinformac¸ões nãoforamadequadamenteregistradas.Osgráficosdeacompanhamentodocrescimento rara-menteforampreenchidosechegarama96,3%nocasodepesoparaaidade.Ousodográficodo IMCnãofoirelatado,adespeitodoquadrocrescentedaobesidadeinfantil.Apenasdoisestudos referirampreenchimentodosmarcosdodesenvolvimentoe,nesses,houveregistrodosmarcos emaproximadamente20%dosinstrumentosverificados.
Conclusões: Os resultados dos artigos revistos evidenciam subutilizac¸ão do instrumento e refletembaixasensibilizac¸ãodosprofissionaisdesaúdeparaoregistronodocumentode acom-panhamentodesaúdedacrianc¸a.
©2015SociedadedePediatriadeSãoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Thefunctionanduseofachildhealthmonitoringtoolhave beendiscussedinthecontextofprimaryhealthcarepolicy over thepast threedecadesin Brazil.1---5 Thistool’s form,
features,andcontenthavegonethroughmanychanges. Fur-thermore, it had its goals and target audience expanded inan attempttobecome aneffective toolin childhealth promotion.3,6,7
In thosesamethreedecades,theeconomic,social and demographictransformations havechanged the epidemio-logicalprofileofthepopulation.8,9Thesewereaccompanied
by changes in the country’s policy and health system,10
whichcausedareorderingofprioritiesintheBrazilian pub-lichealthagenda.4,5Therehavebeenmanyadvancesinthe
indicatorsofprimarycare,suchasincreasedaccessto pre-natal and immunization servicesand breastfeeding rates, andallcontributedtothedeclineinchildmortality.8,11 All
these changes have posed new challenges to ensure the health of a growingand developing individual.12---15 It also
causedthetransitionfromamodelofcarefocusedonacute illnesstoonebasedontheintegrationofhealthservicesand intersectoralhealthpromotion.8,10,16
Inthistransition,theFamilyHealthProgram(FHP)isthe key strategy torestructure the care model of the Brazil-ian Unified HealthSystem (SistemaÚnico de Saúde----SUS) since1994.10 The firstcontactof the population withthe
local health system is through the family health teams, whichcoordinatecareandseektointegratehealthservices. Thehealthpromotionactivitiesgobeyondthewallsofthe healthcentersandtakeplaceintheterritory,thatis,inthe homesandcommunity,10anditisintheperformanceofsuch
activitiesthatthechildmonitoringtoolrecoversits histori-calfunction.17
The actions carried out in child’s primary health care areessential for early detection of potential growth and developmentchanges,aswellastodecreasemorbidityand mortalityrisks.Child growthis a dynamic andcontinuous process of differentiation from conception to adulthood, whichdependsontheinteractionofbiological characteris-ticsand life experiencesin the environment.2,17 The best
monitoring method is the periodic record of the child’s weight and height18 and, currently, the body mass index
(BMI).5 Thedevelopment,in turn,isbroadandreferstoa
progressivetransformationthatalsoincludesgrowth, mat-uration,learning,andpsychicandsocialaspects.2Its
mon-itoringinvolvesactivitiesthatassessstepsormilestonesof psychomotordevelopmentofchildrenineachagegroupand candetectproblemsandchangesinchilddevelopment.19
Originally,theChildHealthCard(CHC),proposedforthe country in 1984,2 was the monitoring of basic actions of
theMinistry of Health(MOH) for child health. From 1984 to2003,2,3theCHChasbeenmodifiedandrevised,withthe
additionof children’srights andsome milestones of child development.TheadoptionoftheCHCwasexplicitly men-tionedin2004intheAgendaofCommitmentsforComplete HealthandMortalityReduction.4
In2005,theCHChastakentheformofabookletandis nowcalledtheChildHealthRecord(CHR).6,7Inthisbooklet,
the child’sfull potential of growth and developmentand preventingprevalentchildhooddiseases.Currently,theMOH distributesthreemillioncopiesoftheCHRtothemunicipal departments,which mustpass themtopublicandprivate hospitals.Itisafreedocumentdeliveredtothenewborn’s family.There is no quantitativestudy compiling evidence frompreviousstudiesregardingtheuseofCHC/CHR.17,20---26
Therefore,thepurposeofthisarticle is toperforma sys-tematicreviewtoassessthecompletenessofCHCorCHRby healthprofessionalsinBrazil,basedonevidencepublished intheliterature,withemphasisonvariablesofmonitoring thegrowthanddevelopmentofthechild.
Method
The search was performed without restriction on year of publicationinthefollowingelectronicdatabases:Cochrane Brazil, Latin American and Caribbean Health Sciences (Lilacs),ScientificElectronicLibraryOnline(SciELO), Medi-calLiteratureAnalysisandRetrievalSystemOnline(Medline) and reference lists of articles, according to Preferred ReportingItemsfor Systematic reviewsandMeta-Analyses (Prisma).27 The following descriptors and keywords were
used:‘‘growthand development’’,‘‘child development’’, ‘‘childhealthrecord’’,‘‘childhealthhandbook’’,‘‘health recordandchild’’,and‘‘childhandbook’’.
Thearticlesincludedattendedthefollowingcriteriafor methodologicalquality28:hypothesesordefinedobjectives,
outcomedescription,characteristics ofparticipants, stud-iedvariables,mainresultsandcharacteristicsoflosses,and adequacyofstatisticaltestsused.
ThisreviewincludesonlyworksperformedinBraziland publishedinindexedjournals, whichmeasured the useof thegrowthanddevelopmentmonitoringtoolpreparedand
distributedbytheMinistryofHealthfrom1984,and quan-titativelyassessedthefillingoutofbooklets.
Exclusion criteria were review articles, manuals, and completionofcoursework;themethodofdataanalysiswas qualitative, restricted only tovaccination or thosewhose sample consistedof specificrisk groups,suchaslow birth weight and prematurity, with genetic and underlying dis-eases.
The1984versionofCHCisabrochureoncoatedpaper, printedindifferentcolorsandsizesforboysandgirls,which canbefolded inthree,withspacesforchildidentification data,consultations,weightmeasurementaccordingtoage, growthmonitoringchartupto5yearsold,and immuniza-tionsdone.Since1995,CHCincluded11milestonesofchild developmentwithspaces torecordthe agein whichthey wereachieved.
CHR, in booklet format that has been reprinted since 2005, has spaces for recording information of the basic health care of children from gestation to 9 years old, complications,treatmentsandgraphicstoindicatethe vari-ationofweight-for-age, height,headcircumference(HC), andBMI.Italsoprovidesaspaceforrecordingthepresence ofthepsychomotordevelopmentalmilestonesaccordingto thechild’sage.
TheCHRshouldbefilledintheroutinefollow-upvisits. TheMinistryofHealthrecommendssevenvisitsinthefirst 12months(1stweekand1st,2nd,4th,6th,9th,and12th month),twointhesecondyear(18thand24thmonth),and fromthatageon,onevisitperyear.7
Results
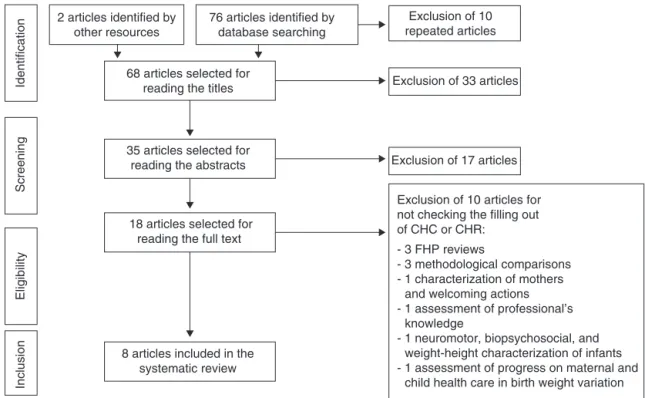
Sixty-eightnon-repeatedarticleswereidentifiedinthe elec-tronic databases and reference lists (Fig. 1). In the first
2 articles identified by other resources
68 articles selected for reading the titles
35 articles selected for reading the abstracts
18 articles selected for reading the full text
Exclusion of 10 articles for not checking the filling out of CHC or CHR:
- 3 FHP reviews
- 3 methodological comparisons - 1 characterization of mothers and welcoming actions - 1 assessment of professional’s knowledge
- 1 neuromotor, biopsychosocial, and weight-height characterization of infants - 1 assessment of progress on maternal and child health care in birth weight variation 8 articles included in the
systematic review
Identification
Screening
Eligibility
Inclusion
76 articles identified by database searching
Exclusion of 10 repeated articles
Exclusion of 33 articles
Exclusion of 17 articles
screening stage, four qualitative theses and 29 articles were excluded by reading the titles. Of these, 12 stud-ieswererestrictedtovaccination,nineinvolveriskgroups and/orunderlyingdisease,threewereofinstructional mate-rials (handbooks), three copies of booklets, one review, andoneprofessionaltrainingstudy inprimaryhealthcare (PHC).
Inthesecondscreeningstage,17articleswereexcluded afterreadingthe abstractsfor notverifyingtheCHC/CHR completion. Elevenarticlesmaybegrouped asevaluation studies:threeofnutritionalindicators,threeofSupervised PracticalActivities, twoof care practices,twoof records analysis,andoneofprofessionals’knowledge.Fivearticles maybegrouped asqualitative studies: twostudies of the meaningofchild care,onediscourseanalysis,one experi-encereport,andonemultidisciplinaryapproachtogrowth anddevelopmentfollow-up.Inadditiontothese,a litera-ture review of the role of nurses in children’s nutritional healthisexcluded.
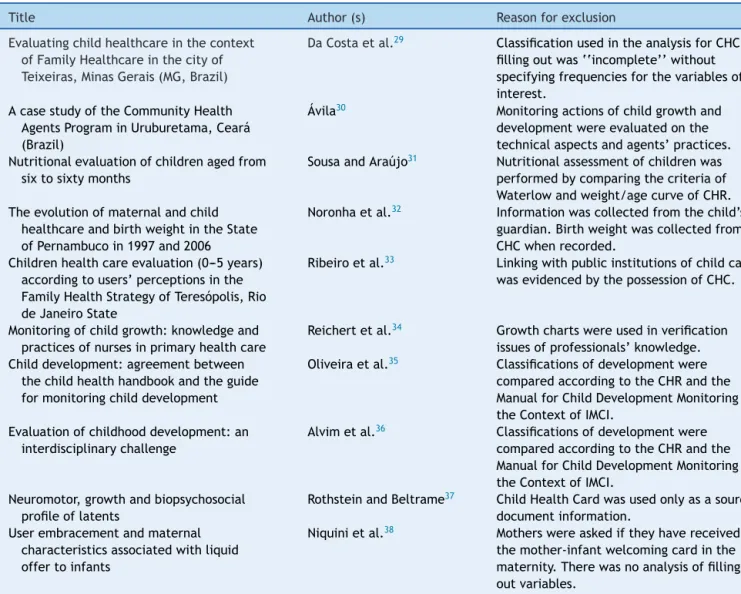
Eighteen articles remained for full text reading. Ten articles29---38 wereexcludedfor notquantitatively assessing
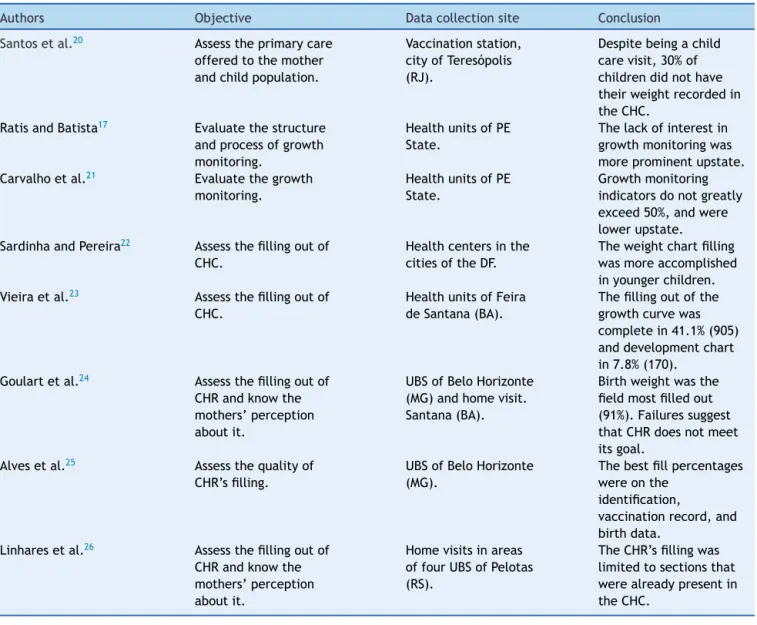
thechildren’shealthmonitoringtools(Table1).Oftheeight includedarticles(Table2),fiveevaluatedthefillingoutof
CHC17,20---23andthree24---26ofCHR.Thesearchesweremadein
theNortheast,17,21,23Southeast,20,24,25South,26andMidwest
regions.22
Informationwasobtainedfromquestionnairesaddressed tothe mother or child’s guardian, or to the directors of healthservices,or wascollecteddirectly fromthe instru-mentstudied.Thesurveysweremadeinserviceswithinthe publichealthnetworkandhomevisits.
The variabilityof themeasured items andof the eval-uation criteria of filling out the tool made it difficult to comparethefillingfrequencyforallitemsofCHCorCHR.
The percentage of tools filled out withdata regarding identification,pregnancymonitoring,andbirthispresented inTable3.In2005,only55.6%oftheCHRhadthenameof thechildfilledin.24Theauthorsreportedthatthemeanage
of these ‘‘unnamed’’ children was68 days(2.2 months), medianof 59days(1.9months),timeat whichthis infor-mationshouldhavebeen filledoutbyhealthprofessionals afterseveral opportunities tosee child----in the maternity andprimary care visits. We alsonotedthat there wasan increaseinthepercentageofCHC/CHRfilledoutbetween 2005 and 2008 for all the identification variables, except forthenumberoftheCertificationofLiveBirth(CLB).The
Table1 Articlesselectedforreadingthefulltextandexcludedfromsystematicreview.
Title Author(s) Reasonforexclusion
Evaluatingchildhealthcareinthecontext ofFamilyHealthcareinthecityof Teixeiras,MinasGerais(MG,Brazil)
DaCostaetal.29 ClassificationusedintheanalysisforCHC fillingoutwas‘‘incomplete’’without specifyingfrequenciesforthevariablesof interest.
AcasestudyoftheCommunityHealth AgentsPrograminUruburetama,Ceará (Brazil)
Ávila30 Monitoringactionsofchildgrowthand developmentwereevaluatedonthe technicalaspectsandagents’practices. Nutritionalevaluationofchildrenagedfrom
sixtosixtymonths
SousaandAraújo31 Nutritionalassessmentofchildrenwas performedbycomparingthecriteriaof Waterlowandweight/agecurveofCHR. Theevolutionofmaternalandchild
healthcareandbirthweightintheState ofPernambucoin1997and2006
Noronhaetal.32 Informationwascollectedfromthechild’s guardian.Birthweightwascollectedfrom CHCwhenrecorded.
Childrenhealthcareevaluation(0---5years) accordingtousers’perceptionsinthe FamilyHealthStrategyofTeresópolis,Rio deJaneiroState
Ribeiroetal.33 Linkingwithpublicinstitutionsofchildcare wasevidencedbythepossessionofCHC.
Monitoringofchildgrowth:knowledgeand practicesofnursesinprimaryhealthcare
Reichertetal.34 Growthchartswereusedinverification issuesofprofessionals’knowledge. Childdevelopment:agreementbetween
thechildhealthhandbookandtheguide formonitoringchilddevelopment
Oliveiraetal.35 Classificationsofdevelopmentwere comparedaccordingtotheCHRandthe ManualforChildDevelopmentMonitoringin theContextofIMCI.
Evaluationofchildhooddevelopment:an interdisciplinarychallenge
Alvimetal.36 Classificationsofdevelopmentwere comparedaccordingtotheCHRandthe ManualforChildDevelopmentMonitoringin theContextofIMCI.
Neuromotor,growthandbiopsychosocial profileoflatents
RothsteinandBeltrame37 ChildHealthCardwasusedonlyasasource documentinformation.
Userembracementandmaternal characteristicsassociatedwithliquid offertoinfants
Table2 Descriptionofthestudiesincludedinthesystematicreview.
Authors Objective Datacollectionsite Conclusion
Santosetal.20 Assesstheprimarycare offeredtothemother andchildpopulation.
Vaccinationstation, cityofTeresópolis (RJ).
Despitebeingachild carevisit,30%of childrendidnothave theirweightrecordedin theCHC.
RatisandBatista17 Evaluatethestructure andprocessofgrowth monitoring.
HealthunitsofPE State.
Thelackofinterestin growthmonitoringwas moreprominentupstate. Carvalhoetal.21 Evaluatethegrowth
monitoring.
HealthunitsofPE State.
Growthmonitoring indicatorsdonotgreatly exceed50%,andwere lowerupstate. SardinhaandPereira22 Assessthefillingoutof
CHC.
Healthcentersinthe citiesoftheDF.
Theweightchartfilling wasmoreaccomplished inyoungerchildren. Vieiraetal.23 Assessthefillingoutof
CHC.
HealthunitsofFeira deSantana(BA).
Thefillingoutofthe growthcurvewas completein41.1%(905) anddevelopmentchart in7.8%(170).
Goulartetal.24 Assessthefillingoutof CHRandknowthe mothers’perception aboutit.
UBSofBeloHorizonte (MG)andhomevisit. Santana(BA).
Birthweightwasthe fieldmostfilledout (91%).Failuressuggest thatCHRdoesnotmeet itsgoal.
Alvesetal.25 Assessthequalityof CHR’sfilling.
UBSofBeloHorizonte (MG).
Thebestfillpercentages wereonthe
identification,
vaccinationrecord,and birthdata.
Linharesetal.26 Assessthefillingoutof CHRandknowthe mothers’perception aboutit.
Homevisitsinareas offourUBSofPelotas (RS).
TheCHR’sfillingwas limitedtosectionsthat werealreadypresentin theCHC.
highestincrease(four-folds)wasinthenumberofBirth Cer-tificates(BC).
Onlyonestudyevaluatedtheserologydatafilledinduring prenatal24andfoundthatthiswasthelowestfilling
percent-ageofthepregnancymonitoringvariables:about50%ofthe CHRstudied.
Birth weightwasthemost describedrecord amongthe variablesrelatedtothe child’sbirth (Table 3).There was an increase in the filling percentages among the studied CHC/CHR,buttherewasadecreasewhenthetoolchanged, suchasthegestationalage,forexample.Between2001and 2006,therewasanincreaseinthefillingoutofApgarand littlevariationinthefillingof heightandhead circumfer-ence.
The results of the monitoring variables of growth and development are shown in Table 4. Only two studies20,26
reportedconsultationrecordsconcerninggrowth.The low-est percentage of CHR filling out was 74.6%, weight monitoringin1998.20 However,10yearslater,theweight,
height,andHCrecordsweremorethan80%filledoutinthe workbyLinharesetal.26
RecordsofweightandHCatbirthinthegraphsshowed low frequency of CHR filled out. In works performed in
Pernambuco,birthweightatbirthwasonlyindicatedonthe chartin36.9%17 and44.1%21 ofthecards,although itwas
recordedin86.8%17 and89.4%21 (Table4),respectively, of
thesecards.Similarly, inBeloHorizonte,25 only 69.3%and
15.5%oftheCHRhadmarkingsonthechartsofweightand HCatbirth,respectively.
The filling out percentage of the weight-for-age chart showed greatvariationbetween studies (21.1---96.3%) due tothecriteriausedtoconsiderthefillingoutas appropri-ate.Forchildrenuptooneyear,whenarecordeverythree monthswasrequired,Vieiraetal.23reported41.1%of
ade-quatefilling outin theweight-for-age chart.In the study that considered a singlemarking as sufficient,a percent-ageof96.3%wasreported.26IntheFederalDistrict,2221.1%
of correctfillingoutwerefound, accordingtothe recom-mended by the Ministry of Health. It was found that the filling out percentage decreased withage, from53.8% in the agegroupup tofivemonthsto6.6%in theage group of 48---60 months. In Pernambuco,17 59.9% of CHC had a
Table3 Fillingoutpercentageofidentification,pregnancyandbirthmonitoringdatareportedinthestudiesincludedinthe systematicreview.a
Authors Ratisand
Batista17
Carvalho etal.21
Vieira etal.23
Goulart etal.24
Alves etal.25
Linhares etal.26
Researchyear 1998 1998 2001 2005 2006 2008
Document CHC CHC CHC CHR CHR CHR
N 1194 662 2215 797 355 107
Age <5years <12months ≤12months <9months <16months <12months
Identification
Name --- --- 99.8 55.6 93.8 93.5
Birthdate --- --- 99.3 90.1 99.7 100
Birthplace --- --- 76.6 --- --- 98.1
Mother’sname --- --- --- 90.7 98.9 99.1
Address --- --- --- 38.9 --- 73.8
Telephone --- --- --- 22.1 --- 47.7
Neighborhood --- --- --- 33.4 --- 67.3
Zipcode --- --- --- 14.6 --- 21.5
City --- --- --- 34.3 --- 64.5
Ethnicity/Color --- --- --- 50.1 --- 66.4
N◦CLB --- --- --- 60.9 --- 33.6
N◦BC --- --- --- 2.0 --- 8.4
Gestation
Prenatal --- --- --- 59.6 58.0
---N◦prenatalvisit --- --- --- 68.5 69.9
---Serology --- --- --- 50.0 ---
---Typeofdelivery --- --- 93.3 84.9 89.3
---Birth
Gestationalage --- --- --- 75.8 72.4
---Apgar5’ --- --- 28.4 76.7 53.5
---Weight 86.8 89.4 97.2 91.1 96.9
---Length --- --- 91.8 89.6 91.2
---Headcircumference --- --- 88.9 84.9 85.6
---CLB,CertificateofLiveBirth;BC,BirthCertificate.
a ThestudiesbySantosetal.20 andSardinhaandPereira22showednofillingoutresultsofidentification,pregnancymonitoring,and birth.
groups: 27.8% (<12 months), 21.7% (12---24 months), and 27.2%(48---60months).However,40.5%oftheCHChadtwo tosixpointsonthe chart.Of these,46% intheage group wereunderoneyearand29.7%between48and60months. Linhares etal.26 weretheonlyonestoobservethe
fill-ingoutinthelength/height-for-agechart.Ofthe107CHR, 42.1%hadatleastonerecord,regardlessofthechild’sage. TherewasnoreportonrecordsofBMIchartforagebythe authorsoftheworksincludedinthisreview.
Onlytwostudiesassessedthepresenceofrecordsinthe developmentmonitoringtool.InFeiradeSantana,2322.1%of
CHChadrecordsinthechart,butonly7.8%werecomplete, consideringthechild’sage.InBeloHorizonte,25 only18.9%
ofCHRmetthecriteriafor presentingrecordsinthreeor moreagegroups.
Discussion
Forthreedecades,the children health programsin Brazil proposedasastrategyatooltomonitorandpromotechild health.The resultspresented inthisstudyhave identified important issues in using this instrument to provide the child’sprimaryhealthcare.
Although studies report that most children have the CHCor CHR,themonitoring ofchild growthseemsnot to receivetheproperattentionbyhealthteams.Ofthethree studies that assessed the CHR,24---26 two presented results
regarding the filling out of the HC chart, one regarding thelength/heightandnoneregardingBMIforage, regard-less of the epidemiological nutritional profile in Brazil. Currently, the coexistence of two antagonistic situations justifiestheconductofdifferentclinicaland epidemiologi-calapproaches:nutritionaldeficiencyand,attheopposite pole,thecombinationofproblemsrelatedtoovereatingand unhealthylifestyles.39,40Astheoccurrenceofmalnutrition
declines,theprevalenceofanemia,overweightandobesity increasesin the Brazilian population.39 The IMC has been
validatedasamarkerofadiposity andoverweightin chil-drenandasaobesitypredictorinadulthood.41 Therefore,
itsuseisrecommendedsincethechild’sbirth.42
To assess the cranial growth rate and its inter-nal structures in childhood, HC systematic measurement and recording on the HC chart for age are needed. It draws attention to a filling out as low as 30.7%25 and
35.5%26 of a parameter that reflects the state of child
Table4 Fillingoutpercentageofgrowthanddevelopment monitoringvariablesinthe studiesincludedinthesystematic review*
Authors Santos
etal.20
Ratisand Batista17
Carvalho etal.21
Sardinhaand Pereira22
Vieira etal.23
Alves etal.25
Linhares etal.26
Tool CHC CHC CHC CHC CHC CHR CHR
Age <12months <5years <12months <5years ≤12months <16months <12months
Growth
Datafrommedicalvisits
(N=299) (N=107)
Visitdate 91.6
Age 90.7
Weight 74.6a 89.7b
Height 87.9b
Headcircumference 82.2b
Birthdataincharts
(N=1193) (N=662) (N=355)
Weight 36.9 44.1 69.3
Headcircumference 15.5
Datafromvisitsincharts
(N=307) (N=624) (N=402) (N=3543) (N=2200) (N=355) (N=107)
Weigh 70.4a 59.9c 58.2d 21.1e 41.1f 59.4g 96.3h
Length/height 42.1h
Headcircumference 30.7g 35.5h
Development
(N=2191) (N=355)
Milestones0---36months 7.8i 18.9j
* Goulartetal.24didnotpresentfillingoutdataonthevariablesofgrowthanddevelopmentmonitoring. aAtleastonerecordinthethreemonthspriortotheinterview.
b Recordsaccordingtothechild’sage. c Recordsintheconsultationday. d Lastupdatedrecord.
e Recordsproperlypunctuated,accordingtotheMinistryofHealth. f Atleastonerecordeverythreemonths.
gWeightandHCrecordsmarkedonthechartwhosedifferencebetweentheageatthetimeoftherecordandthechild’schronological
agewas≤3months.
h Atleastonerecordverified. iAllrecordsmatchingthechild’sage.
j RecordsinthreeormoreagegroupspresentinCHR.
individualfollow-upofchildrenupto24months,theperiod ofgreatestpostnatalgrowth.5,45
Low birth weight is one of the best indicators of the qualityofhealth andlifeofchildrenduetoitsclose rela-tionshipwithchildrenmortality anddamagetothelinear growth,weight,andmentalandmotordevelopment.46
How-ever,thelowrecordingofweightatbirthinthechartshows theunderestimatedroleassignedtothisindicatorin mon-itoringthechild’shealthstatusattheplacesevaluatedby theworksreviewedhere.
Anotherproblemfound inthisreview isthepoorresult in the filling out of the milestones of child development chart.The monitoring action consistsof performing phys-icalexamination, thorough neuropsychomotor evaluation, identificationofriskfactors,andrecordintheCHRofall pro-ceduresperformedinthechild,aswellasthefindingsofthe medicalvisits.5Thisactionisaformofpreventive
interven-tionthatincludesactivitiesrelatedtopromotionofnormal developmentanddetectionofproblemsintheprocess.47It
bringstogetherdifferentevaluationsthatincludethe per-ceptionofparents,teachers,andhealthprofessionals.33,36,48
Anestimated200 millionchildrenworldwideunderthe ageoffiveareatriskoffailingtoachievetheirdevelopment potential.49WiththeuseofCHR,Alvimetal.36wereableto
trace35%ofchildrenwithprobableorpossible developmen-taldelay,whenevaluating122childrenfromtwomonthsto twoyearsoldinthecityofBeloHorizonte.
Costa et al.29 (2011) found failure in the filling out
of CHR when assessing the health care provided to chil-dren by the Family Health Program (FHP) in the city of Teixeiras (MG). The authors reported that most children (77.2%)hadtheCHC,butall(171)wereincomplete.There was no informationon weight and height, recordsin the growth chart, and many mothers did not understand the meaning of the curve. The card worked just asa record for vaccine control, and not asa child health monitoring tool.
The child’s health monitoring tool led to operational changes in the health services. Since2005, hospitals and maternities have become responsible for the distribution and recording of information regarding pregnancy, child-birth, and neonatal period. CHR, as a health promotion tool,alsocausedchangesinhealthstatusperceivedbythe population.24 Demandforhealthservicescannolongerbe
motivatedonly bythepresence ofdiseaseor vaccination, asreportedbyVitolo etal.50 in 2010.The findingsof this
studyindicatedthat66.2%(n=393)ofthoseresponsiblestill considered the child monitoring by the childcare service unnecessary in the absence of disease. This frequency is incontrastwiththehigh coverage(90%)oftheup-to-date immunizationschedule.
The results presented in this review should take into accountthatthemethodologyusedinthearticlesreviewed toassess thefilling outof theCHC andCHR wasnot uni-form.Insomestudies,thecriterionwasbasedonatleast onerecordinthethreemonthsprecedingtheinterview. Cer-tainly,thevalueswouldbelowerthanthosereportedifthe criterionusedwasmore restrictive,suchasthe minimum consultationtimetableproposedbytheMOH.Anotherissue toconsideristhecomparisonbetweensurveysperformedin differentsocioeconomicandculturalrealities.
Anyway,theabsenceorrecordsincorrectnesssuggestsa weaklinkofprofessionalswithbasichealthcareactionsand adiscontinuitybetween theactionsinitiated inmaternity andtheproposalsforprimarycare.
Healthprofessionalsoftenbecomeoverwhelmedintheir routines.Beyondtheuniverseofcare,theworkinvolves fill-ingoutvariousformsdemandedbytheinstitution.Thefilling outofaCHRcannotbeconsideredanadditional administra-tiverecord,butatoolforchildrenhealthpromotionandto obtaingoodqualityinformationtobettertargettheactions ofservices.
However,itisimportanttoemphasizethattheabsence of records does not mean exactly the non-performance of medicalprocedures.30,51,52 However,the importanceof
recordstobuildtheepidemiologicalprofileofapopulation andasachannelofcommunicationbetweenhealth profes-sionals in thedevelopmentof their actionsis recognized. Whendoneright,itallowsthepracticeofpersonalizedcare andreflectsthequalityofcare.25
Inthechildhealthmonitoringprogram,theprofessional focusshouldbemissingnoopportunitiesforaction,whether inthepromotionand/orpreventionand/orassistance,keep bondwiththe family,andencourage continuousandjoint responsibilityserviceandfamily.53Co-responsibilityof
fam-ilies, professionals,and servicescan bethekey tobetter usetheCHR25inchildcare.
The actofprovidingexplanations,involving thefamily, and recordinginformation about the child’shealth condi-tionsisawayofcaringforandencouragingthecontinuity ofcare.Theunderstandingbythefamiliesofthistool func-tioninchildhealthmonitoringisessentialforthemtotake holdofitandappreciateit.
Conclusion
ThirtyyearsaftertheimplementationoftheChildrenHealth Integral Assistance Program (PAISC), the use of the child
health monitoring tool is not consolidated, according to researchreports.Thelackofawarenessofthehealth pro-fessionalsforfillingoutthestudyinstrumentwasevident.
This review also shows that the diagnostic of use and fillingoutquality ofsuch tools inBrazil is restricted toa fewlocal works,which donot evaluate allvariables con-sidered essential for child health monitoring. Therefore, furtherstudiesaredesirable,withamethodologyconsistent withpreviousstudiesthatallowdrawinganationalandmore updatedpicture.Thisknowledgecouldbeenhancedif com-binedwithotherqualitativestudies,inwhichprofessionals fromthebasic unitsandFHPteamsexpresstheirviewson therelationshipofpromotionandmonitoringactionsforthe child’scompletehealthwiththefillingoutandappreciation ofCHR.
Funding
FundoNacionaldeSaúde(SMS/FNS/MS)bytheagreement signedbyCoordenac¸ãoGeraldaSaúdedaCrianc¸ae Aleita-mentoMaterno(CGSCAM/DAPES/SAS/MS)withtheInstituto NacionaldeSaúdedaMulher,daCrianc¸aedoAdolescente FernandesFigueira(IFF/Fiocruz).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Brasil --- Ministérioda Saúde.Assistência integralà saúdeda crianc¸a:ac¸õesbásicas.Brasília:MinistériodaSaúde;1984. 2.Brasil---MinistériodaSaúde.SecretariadePolíticasdeSaúde
--- Departamento de Atenc¸ão Básica. In: Saúde da crianc¸a: acompanhamentodocrescimentoedesenvolvimentoinfantil. Brasília:MinistériodaSaúde;2002[CadernosdeAtenc¸ãoBásica n◦11].
3.Brasil --- Ministério da saúde. Informe Saúde; 2014. Avail-able from: http://bvsms.saude.gov.br/bvs/periodicos/ informesaude/informe208.pdf[accessed02.08.14].
4.Brasil --- Ministério da Saúde. Secretaria de Atenc¸ão à Saúde--- Departamento deac¸ões Programáticas Estratégicas. Agenda de compromissos para a saúde integral da crianc¸a e reduc¸ão da mortalidade infantil. Brasília: Ministério da Saúde;2004.Available from:http://bvsms.saude.gov.br/bvs/ publicacoes/agendacomprocrianca.pdf
5.Brasil---MinistériodaSaúde.SecretariadeAtenc¸ãoàSaúde ---DepartamentodeAtenc¸ãoBásica.In:Saúdedacrianc¸a: cresci-mentoedesenvolvimento.Brasília:MinistériodaSaúde;2012 [CadernosdeAtenc¸ãoBásica,n◦33].
6.Brasil---Ministério daSaúde.Cadernetadesaúdedacrianc¸a: menino;2013.Availablefrom:http://bvsms.saude.gov.br/bvs/ publicacoes/cadernetasaudecriancamenino.pdf [accessed 01.10.13].
7.Brasil---MinistériodaSaúde.SecretariadeAtenc¸ãoàSaúde ---DepartamentodeAc¸õesProgramáticasEstratégicas.In:Manual parausodacadernetadesaúdedacrianc¸a.Brasília:Ministério daSaúde;2005.
9.MenezesRC,LiraPI,OliveiraJS,LealVS,SantanaSC,Andrade SL, et al. Prevalence and determinants of overweight in preschoolchildren.JPediatr(RioJ).2011;87:231---7.
10.Paim J, Travassos C, Almeida C, Bahia L, Macinko J. O sistema de saúde brasileiro: história, avanc¸os e desafios. Séries: Saúde no Brasil 1. Lancet. 2014. Available from: http://www.abc.org.br/IMG/pdf/doc-574.pdf [accessed 24.06.14].
11.VictoraCG,AquinoEM,LealMC,MonteiroCA,BarrosFC, Szwar-cwald CL.Saúde demães ecrianc¸as no Brasil:progressos e desafios.Séries:SaúdenoBrasil2.Lancet.2014.Availablefrom: http://www.thelancet.com[accessedJune2014].
12.Goldani MZ, Barbieri MA, Rona RJ, Da Silva AA, Bettiol H. Increasingpre-termandlow-birth-weightratesovertimeand theirimpactoninfantmortalityinsouth-eastBrazil.JBiosoc Sci.2004;36:177---88.
13.MoreiraME.Problemasdesaúdenainfância:desafiosdo trata-mentoàprevenc¸ão[editorial].CiencSaudeColet.2010;15:318. 14.Moreira ME,GoldaniMZ.Acrianc¸aéopaidohomem:novos desafiosparaaáreadesaúdedacrianc¸a.CiencSaudeColet. 2010;15:321---7.
15.GomesMA.Aspolíticaspúblicasnaáreadasaúdedacrianc¸a. CiencSaudeColet.2010;15:328---36.
16.Frota MA,Maia JA,PereiraAS,NobreCS, VieiraLJ.Reflexão sobre políticas públicas e estratégias na saúde integral da crianc¸a.RevEnfermFoco.2010;1:129---32.
17.Ratis CA,Batista FilhoM. Aspectosestruturaiseprocessuais da vigilância do crescimento de menores de cinco anos em servic¸ospúblicosdesaúdedoEstadodePernambuco.RevBras Epidemiol.2004;7:44---53.
18.BarrosFC,VictoraCG.Saúdematerno-infantilemPelotas,Rio GrandedoSul,Brasil:principaisconclusõesdascomparac¸õesde coortesdenascimentode1982,1993e2004.CadSaudePublica. 2008;24Suppl.3:S461---7.
19.Figueiras AC, Souza IC, Rios VG, Benguigui Y. Manual para vigilânciado desenvolvimento infantilno contexto daAIDPI. Washington:OPAS;2005.
20.SantosSR,CunhaAJ,GambaCM,MachadoFG,LealFilhoJM, Moreira NL.Avaliac¸ãodaassistênciaàsaúdedamulhereda crianc¸aemlocalidadeurbanadaregiãoSudestedoBrasil.Rev SaudePublica.2000;34:266---71.
21.CarvalhoMF,LiraPI, RomaniSA,SantosIS,VerasAA,Batista FilhoM.Acompanhamentodocrescimentoemcrianc¸asmenores de um ano:situac¸ão nosservic¸os desaúdeem Pernambuco, Brasil.CadSaudePublica.2008;24:675---85.
22.Sardinha LM, Pereira MG. Avaliac¸ão do preenchimento do cartão dacrianc¸a noDistritoFederal.Brasilia Med.2011;48: 246---51.
23.VieiraGO,VieiraTO,CostaCO,SantanaNettoPV,CabralVA. Usodocartãodacrianc¸aemFeiradeSantana,Bahia.RevBras SaudeMaterInfant.2005;5:177---84.
24.GoulartLM,AlvesCR,VianaMR,MoulinZS,CarmoGA,CostaJG, etal.Cadernetadesaúdedacrianc¸a:avaliac¸ãodo preenchi-mentodosdadossobregravidez,partoerecém-nascido.Rev PaulPediatr.2008;26:106---12.
25.AlvesCR,LasmarLM,GoulartLM,AlvimCG,MacielGV,Viana MR, et al. Qualidade do preenchimento da caderneta de saúde da crianc¸a e fatores associados. Cad Saude Publica. 2009;25:583---95.
26.Linhares AO, GiganteDP, Bender E,Cesar JA. Avaliac¸ãodos registros eopinião dasmãessobrea caderneta desaúdeda crianc¸aemunidadesbásicasdesaúde,Pelotas,RS.RevAMRIGS. 2012;56:245---50.
27.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting sys-tematic reviewsand meta-analysesof studies that evaluate
healthcare interventions:explanationandelaboration.BMJ. 2009;62:e1---34.
28.SzkloM.Qualidadedeartigos científicos.RevSaudePublica. 2006;40:30---5.
29.DaCostaGD,CottaRM,ReisJR,FerreiraML,ReisRS, Frances-chiniSC.Avaliac¸ãodaatenc¸ãoàsaúdedacrianc¸anocontexto dasaúdedafamílianomunicípiode Teixeiras,MinasGerais. CiencSaudeColet.2011;16:3229---40.
30.Ávila MM. O Programa de agentes comunitários de saúde no Ceará: o caso de Uruburetama. Cienc Saude Colet. 2011;16:349---60.
31.SousaFG,AraújoTL.Avaliac¸ãonutricionaldecrianc¸asdeseis asessentameses.REBEn.2004;57:534---6.
32.NoronhaGA,LimaMC,LiraPI,VerasAA,Gonc¸alvesFC,Batista FilhoM.Evoluc¸ãodaassistênciamaterno-infantiledopesoao nascernoEstadodePernambucoem1997e2006.CiencSaude Colet.2012;17:2749---56.
33.RibeiroJM,SiqueiraSA,PintoLF.Avaliac¸ãodaatenc¸ãoàsaúde da crianc¸a (0-5 anos) no PSF de Teresópolis (RJ) segundo a percepc¸ãodosusuários.CiencSaudeColet.2010;15:517---28. 34.ReichertAP,AlmeidaAB,SouzaLC,SilvaME,ColletN.Vigilância
do crescimento infantil: conhecimento e práticas de enfer-meirosdaatenc¸ãoprimáriaàsaúde.RevRene.2012;13:114---26. 35.Oliveira LL, Costa VM, Requeijo MR, Rebolledo RS, Pimenta AF,LemosSM.Desenvolvimentoinfantil:concordânciaentrea cadernetadesaúdedacrianc¸aeomanualparavigilânciado desenvolvimentoinfantil.RevPaulPediatr.2012;30:479---85. 36.AlvimCG,GuimarãesFG,MeinbergNL,AguiarLT,CaetanoLC,
CarruscaLC, etal. A avaliac¸ãodo desenvolvimento infantil: umdesafiointerdisciplinar.RevBrasEducMed.2012;36Suppl. 1:51---6.
37.Rothstein JR, Beltrame TS. Características neuromotoras, pondo-estaturais e biopsicossociais de lactentes. Rev Bras CrescimentoDesenvolvimentoHum.2011;21:269---81.
38.NiquiniRP,BittencourtSA,LacerdaEM,OliveiraMI, LealMC. Acolhimentoecaracterísticasmaternasassociadosàofertade líquidosalactentes.RevSaudePublica.2010;44:677---85. 39.Batista Filho M, Rissin A. A transic¸ão nutricional no Brasil:
tendênciasregionaisetemporais.CadSaudePublica.2003;19 Suppl.1:S181---91.
40.Batista Filho M,Souza AI,Miglioli TC, SantosMC. Anemiae obesidade:umparadoxodatransic¸ãonutricionalbrasileira.Cad SaudePublica.2008;24Suppl.2:S247---57.
41.Brock RS, FalcãoMC, Leone C. Body mass index references valuesfor newborn accordingto gestational age. NutrHosp 2008;23:487---92.
42.CardosoLE,FalcãoMC.Importânciadaavaliac¸ãonutricionalde recém-nascidospré-termopormeioderelac¸ões antropométri-cas.RevPaulPediatr.2007;25:135---41.
43.Bartholomeusz HH, Courchesne E, Karns CM. Relationship between head circumference and brain volume in healthy normal toddlers, children, and adults. Neuropediatrics. 2002;33:239---41.
44.García-AlixA,Sáenz-dePipaónM,MartínezM,Salas-Hernández S,QueroJ.Utilidaddelperímetrocefálicoenelreciénnacido para anticipar problemas en el neurodesarrollo.Rev Neurol 2004;39:548---54.
45.JaldinMG,PinheiroFS,SantosAM,MunizNC,BritoLM. Cresci-mento do perímetro cefálico nos primeiros seis meses em crianc¸asemaleitamentomaternoexclusivo.RevPaulPediatr. 2011;29:509---14.
47.Zeppone SC, Volpon LC, Del Ciampo LA. Monitoramento do desenvolvimento infantil feito no Brasil. Rev Paul Pediatr. 2012;30:594---9.
48.FigueirasAC,PucciniRF,SilvaEM,PedromônicoMR.Avaliac¸ão das práticas e conhecimentos de profissionais da atenc¸ão primáriaàsaúdesobrevigilânciadodesenvolvimentoinfantil. CadSaudePublica.2003;19:1691---9.
49.Grantham-McGregorS,CheungYB,CuetoS,GlewweP,Richter L,StruppB. Developmentalpotentialin thefirst5 yearsfor childrenindevelopingcountries.Lancet.2007;369:60---70. 50.VitoloMR,GamaCM, CampagnoloPD. Frequência deuso do
servic¸opúblicodepuericulturaefatoresassociados.JPediatr (RioJ).2010;86:80---4.
51.Pordeus AM, Forte LB, Vieira JE. Acompanhamento antropométrico de crianc¸as: o ideal e o realizado. Rev BaianadeSaudePublica.2007;31:212---22.
52.SantosNetoET,OliveiraAE,ZandonadeE,GamaSG,LealMC. O que os cartões de pré-natal das gestantes revelam sobre a assistência nos servic¸os do SUS da Região Metropolitana daGrandeVitória,EspíritoSanto,Brasil. CadSaudePublica. 2012;28:1650---2166.