SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Elderly
with
proximal
hip
fracture
present
significantly
lower
levels
of
25-hydroxyvitamin
D
夽
Marcelo
Teodoro
Ezequiel
Guerra
a,b,∗,
Eduardo
Terra
Feron
b,
Roberto
Deves
Viana
b,
Jonathan
Maboni
b,
Stéfany
Ignêz
Pastore
b,
Cyntia
Cordeiro
de
Castro
baUniversidadeLuteranadoBrasil(Ulbra),DepartamentodeOrtopediaeTraumatologia,Canoas,RS,Brazil
bUniversidadeLuteranadoBrasil(Ulbra),HospitalUniversitárioMãedeDeus,Servic¸odeOrtopediaeTraumatologia,Canoas,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14January2016 Accepted15February2016 Availableonline31August2016
Keywords:
VitaminDdeficiency Hipfractures
Osteoporoticfractures
a
b
s
t
r
a
c
t
Objective:Tocompareserum25-hydroxyvitaminD(25[OH]D)levels,aserummarkerof vita-minD3,betweenpatientswithandwithoutproximalhipfracture.
Methods:Thiswasacase–controlstudyinwhichserumsamplesof25(OH)Dwereobtained from110proximalhipfractureinpatientsand231controlpatientswithoutfractures,all over60yearsofage.Levelsof25(OH)Dlowerthanorequalto20ng/mLwereconsidered deficient;from21ng/mLto29ng/mL,insufficient;andabove30ng/mL,sufficient.Sex,age, andethnicitywereconsideredforassociationwiththestudygroupsand25(OH)Dlevels.
Results:Patientswithproximalhipfracturehadsignificantlylowerserum25(OH)Dlevels (21.07ng/mL)thancontrols(28.59ng/mL;p=0.000).Amongpatientswithproximalhip frac-ture,54.5%haddeficient25(OH)Dlevels,27.2%hadinsufficientlevels,andonly18.2%had sufficientlevels.Inthecontrolgroup,30.3%ofpatientshaddeficient25(OH)Dlevels,30.7% had insufficient levels, and38.9% hadsufficient levels. Femalepatientshad decreased serum 25(OH)Dlevelsboth inthefracturegroupand inthecontrolgroup(19.50ng/mL
vs.26.94ng/mL;p=0.000)whencomparedwithmalepatientswithandwithoutfracture (25.67ng/mLvs.33.74ng/mL;p=0.017).Regardingage,therewasasignificantassociation between25(OH)Dlevelsandriskoffractureonlyfortheagegroups71–75yearsandabove 80years.
Conclusion: Patientswithproximalhipfracturehadsignificantlydecreasedserum25(OH)D levelswhencomparedwiththecontrolgroup.Femalepatientshadsignificantlylowerserum 25(OH)Dlevelsinbothgroups.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheUniversidadeLuteranadoBrasil(Ulbra),HospitalUniversitário,DepartamentodeOrtopediaeTraumatologia, Canoas,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.T.Guerra). http://dx.doi.org/10.1016/j.rboe.2016.08.013
Idosos
com
fratura
da
extremidade
proximal
do
fêmur
apresentam
níveis
significativamente
menores
de
25-hidroxivitamina
D
Palavras-chave:
DeficiênciadevitaminaD Fraturasdoquadril Fraturasporosteoporose
r
e
s
u
m
o
Objetivo:Compararosníveisséricosde25-hidroxivitaminaD[25(OH)D],marcadorséricoda vitaminaD3,entrepacientescomesemfraturadaextremidadeproximaldofêmur(FEPF).
Métodos: Estudocaso-controleemqueforamobtidasamostrasséricasde25(OH)Dde110 pacientescomFEPFinternadosede231pacientesdegrupocontrolequenãoapresentaram fraturas,todosacimade60anos.Níveisde25(OH)Dmenoresouiguaisa20ng/mLforam consideradosdeficitários;entre21ng/mLe29ng/mL,insuficientes;eacimade30ng/mL, suficientes.Foramconsideradasasvariáveissexo,idadeeetniaparaassociac¸ãocomos gruposemestudoeosníveisde25(OH)D.
Resultados: PacientescomFEPFapresentaramníveisséricosde25(OH)Dsignificativamente inferiores(21,07ng/mL)comparadoscomosdogrupocontrole(28,59ng/mL;p=0,000).Entre ospacientescomFEPF,54,5%apresentaramníveisde25(OH)Ddeficitários,27,2% insufi-cienteseapenas18,2%suficientes.Jánogrupocontrole,30,3%dospacientesapresentaram níveisdeficitários,30,7%insuficientese38,9%suficientes.Pacientesdosexofeminino apre-sentaramníveisséricosde25(OH)Dreduzidostantonogrupocomfraturaquantonogrupo controle(19,50vs.26,94ng/mL;p=0,000)comparadoscomosdosexomasculinocomesem fratura(25,67vs.33,74ng/mL;p=0,017).Quantoàidade,houveassociac¸ãosignificativaentre osníveisde25(OH)Deriscodefraturaapenasparaasfaixas71-75anoseacimade80.
Conclusão: PacientescomFEPFapresentaramníveisséricosde25(OH)Dsignificativamente reduzidosemcomparac¸ãocomosdogrupocontrole.Pacientesdosexofeminino apresen-taramníveisséricosde25(OH)Dsignificativamentemenoresemambososgrupos.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Proximal femoral fracture (PFF) has a high incidence in patientsolder than 65 years andusuallyresults from low-energytrauma.Despite the resourcesofmodern medicine, there is a high mortality rate, around 25–30% yearly.1–3
Mortality is mainly due to factors such as advanced age, comorbidities,previous cognitiveimpairment,and delay in theprocedure.1,2 PFFalsorepresentsamajorcosttopublic
health,mainlyduetoprolongedhospitalizationandrelated surgicalprocedures.3,4
VitaminDplaysanimportantroleincalciummetabolism, andconsequentlyinbonemineralizationandtheosteoporotic picture.Itsdeficiencyisthereforeanimportantriskfactorfor PFFintheelderly.1,5,6Thebestserummarkerofthisvitamin
is25-hydroxyvitaminD(25(OH)D),whosemetabolicproductis vitaminD3;valuesequaltoorabove30ng/mLareconsidered sufficient.7TheuseofvitaminD3hasbeenrecommendedto
preventfracturesinelderlypatientswithosteoporosis. How-ever,itisnotalwaysroutinelyusedinpublichealthcare.8–10
Thisstudyaimedtocompareserum25(OH)Dlevelsamong elderlypatientswithandwithoutPFF,andtoanalyzethe asso-ciationofvariablessuchasgender,age,andethnicitywiththis condition.
Material
and
methods
This was a case–control study conducted in the Depart-ment of Orthopedics and Traumatology of this institution
betweenJanuary2013andMay2015.Thestudywasapproved bytheEthics CommitteeoftheinstitutionunderCAAENo. 33760914.8.0000.5349.
The fracture group comprised patients over 60 years with PFF. The study included patients with femoral neck, subtrochanteric, and transtrochanteric fractures who had experiencedalow-energyfall.Thecontrolgroupincluded age-matchedindividualswithoutPFFhistory,recruitedamongthe patientsattendedtoattheorthopedicsclinicandother med-icalspecialtiesatthishospital,aswellasinpatientsadmitted for non-orthopedic/traumatological reasons. The exclusion criteriacomprisedpatientsoutsidetheagerange;with frac-tureswithknownhistoryofhighenergy;withmissingdataon medicalrecords,suchasethnicityandsex;orwithunknown serumlevelsorwithoutresultsprovidedbythelaboratory.
Serum 25(OH)D samples were collected forall patients. Inthefracturegroup,bloodsampleswerecollected immedi-atelyafterthepatient’s admission,beforethefinalsurgical procedure.Inthecontrolgroup,sampleswerecollectedafter outpatientcare.Serumlevelswere measuredinastandard laboratory for all samples, measured as nanograms per milliliter(ng/mL).
Theresultsofthebloodcollectionof25(OH)Dweredivided in accordancewith theHorlick classification,wherevalues below 20ng/mL are considered deficient; between 21 and 29ng/mL,insufficient;andabove30ng/mL,normal.7The
vari-ablesgender,age,andethnicitywereconsideredforpurposes ofassociationwiththestudygroupsandlevelsof25(OH)D.
Table1–Samplecharacterization.
Variable Group p
Control(n=231) Fracture(n=110) Total(n=341)
n % n % n %
Ethnicity
White 218 94.4 106 96.4 324 95.0 0.839a
Black 9 3.9 3 2.7 12 3.5
Mixed 4 1.7 1 0.9 5 1.5
Sex
Female 175 75.8 82 74.5 257 75.4 0.808b
Male 56 24.2 28 25.5 84 24.6
Age(years)
60–65 24 10.4 12 10.9 36 10.6 0.850b
66–70 16 6.9 8 7.3 24 7.0
71–75 50 21.6 21 19.1 71 20.8
76–80 51 22.1 20 18.2 71 20.8
>80 90 39.0 49 44.5 139 40.8
Source:Authors
a Chi-squaredtest.
b Fisher’sexacttest.
samplesizecalculatedtoobtainstatisticallysignificantresults was60 patients withPFF(fracture group)and 120patients withoutPFF(controlgroup).
Statisticalanalysis
ThestatisticalprogramusedwasSPSS,version13.0.Results were considered significantata levelof 5%(p≤0.05). Data were expressed as mean and standard deviation or per-centage(%).Thestatisticaldifference betweenthe fracture and control groups and their respectivevariables was cal-culated with the chi-squared and Fisher’s exact tests. The Kolmogorov–Smirnov test of normality indicated that the study variables did notpresent normal distribution; there-fore, a nonparametric test was used in the analysis. The Mann–Whitneytestwas usedtocompare themean serum levelsof25(OH)Dbetweengroups,andthesevalueswere strat-ifiedbyageandgender.Fortheethnicityvariable,itwasnot possibleto perform statisticaltests due to the insufficient numberofcasesforthemixedandblackethnicities.
Results
The present sample comprised 341 patients. The fracture groupincluded110patients,ofwhom82(74.5%)werefemale, and the control group consisted of231 patients, of whom 175(75.8%)were female. Meanageofthe fracturepatients was 78.76±9.52 years, and mean age of the controls was 77.31±7.85years.Therewas nodifferencebetweengroups regarding sex or age (p>0.05). Sample characteristics are describedinTable1.
The serum levels of 25(OH)D in the control group (28.59±12.31ng/mL) were significantly higher than in the fracturegroup(21.07±10.28ng/mL)(p=0.000).Inthefracture group, considering the Horlick classification, 54.5% (n=60)
patientshaddeficientserum25(OH)Dlevels,andonly18.2% (n=20)hadsufficientvalues.Amongthecontrols,38.9%(n=90) were considered tohavesufficientserumlevels; 30.3% had deficientserumlevels(n=70)(Table2).
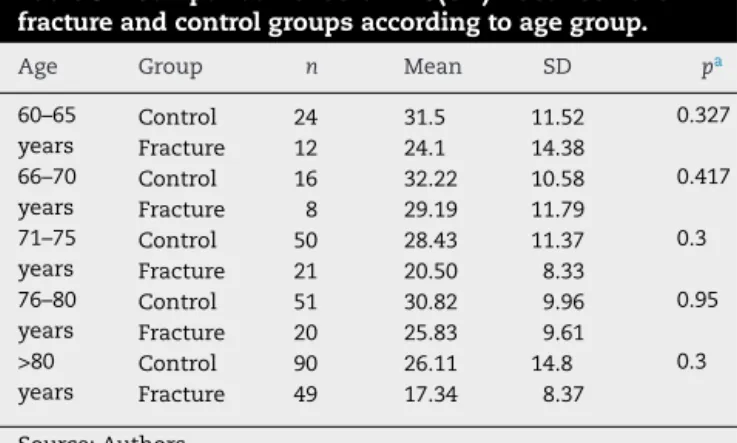
Therewerenosignificantdifferencesbetweenthegroups regardingtheserumlevelsof25(OH)Dfortheagerangesof 60–65years(p=0.327),66–70(p=0.417),and76–80(p=0.095). However, significant differences were observed in the age groups71–75years(p=0.003)andover80(p=0.003)(Table3).
Fortheethnicityvariable,statisticalanalysiswasnot pos-sibleduetoinsufficientnumberofcasesforthemixedand blackethnicities.Descriptivedataforthisvariableareshown inTable4.
Regarding gender, a significant difference was observed in thelevels of25(OH)D betweenthe groups. Lower serum 25(OH)D levels were observed in female patients, with a mean of 19.50±10.01ng/mL in the fracture group and 26.94±11.23ng/mL in the control group (p=0.000). Among males,themeanwassignificantlyhigherinthecontrolgroup (33.74±14.08ng/mL)whencomparedwiththefracturegroup (25.67±9.85ng/mL,p=0.017).
Table2–Serumlevelsof25(OH)Dinthefractureand controlgroupsaccordingtotheHorlickclassification.
25(OH)D Control Fracture Total
n % n % n %
Deficient 70 30.3 60 54.5 130 38.1 Insufficient 71 30.7 30 27.2 101 29.6 Sufficient 90 38.9 20 18.2 110 32.2 Total 231 100.0 110 100.0 341 100.0
Source:Authors
Table3–Comparisonofserum25(OH)Dbetweenthe fractureandcontrolgroupsaccordingtoagegroup.
Age Group n Mean SD pa
60–65 years
Control 24 31.5 11.52 0.327
Fracture 12 24.1 14.38
66–70 years
Control 16 32.22 10.58 0.417
Fracture 8 29.19 11.79
71–75 years
Control 50 28.43 11.37 0.3
Fracture 21 20.50 8.33
76–80 years
Control 51 30.82 9.96 0.95
Fracture 20 25.83 9.61
>80 years
Control 90 26.11 14.8 0.3
Fracture 49 17.34 8.37
Source:Authors SD,standarddeviation.
a p=0.01.
Table4–Comparisonofserumlevelsof25(OH)D betweenthefractureandcontrolgroupsaccordingto ethnicity.
Ethnicity Control Fracture
n Mean SD n Mean SD
White 218 28.73 12.30 106 20.76 10.10 Mixed 9 23.38 10.77 3 29.59 16.32 Black 4 32.83 16.24 1 28.50 0.0
Source:Authors SD,standarddeviation.
Discussion
Thisstudyshowed thatpatients withPFFhad significantly lower serum 25(OH)D levels than the control group. Val-uesconsideredinsufficientintheHorlickclassificationwere observedinboththecontrolgroup(28.59ng/mL)andinthe fracturegroup(21.07ng/mL).Consideringthis classification, halfofpatientswithPFFhaddeficientlevelsofthisvitamin. Lowlevelsof25(OH)D werealsofoundinthe control sam-ple,with30.7%ofpatientswithinsufficientlevelsand30.3% deficient.
Inameta-analysisthatincluded 15case–controlstudies amongpatientswithandwithoutPFF,ofthe17patients ana-lyzed,theserumlevelsof25(OH)Dinpatientswithfracture weresignificantlylowerthan inthecontrolgroup.11
Rama-sonetal.12conductedastudywith485elderlywithPFFand
alsofound low levelsof 25(OH)D inthese patients, with a meanvalueof19.1ng/mL,57.5%deficient,34.5%insufficient, andonly8%hadsufficientlevels.Browneetal.,13usinga
dif-ferentserum measuringunit(nmol/L) inastudy inIreland with156 elderlypatients with PFF,foundthat over 67% of theirsamplehadinsufficientordeficient25(OH)Dserum lev-els.Gumieroetal.,14inaBrazilianstudyongaitinpatients
withPFF,alsoobservedlowlevelsof25(OH)D,withamean valueof27.8ng/mL;33.7%ofthe samplehaddeficient val-ues,whichdiffersfromthefindingsofthepresentstudy.7,14
Reducedserum levelsof25(OH)D weresignificantlyrelated to PFF both in the present study and in previous studies;
however, specific differences in serum levels of this vita-min are recognized by various authors,due to its relation tosunexposureandthegeneticcharacteristicsofthelocal population.11–13
ConsideringpatientswithoutPFF,Saraivaetal.15alsofound
thepresenceofhypovitaminosisinastudyinanelderly pop-ulation, having subdivided the sample into two groups. In thefirst group,consistingofhospitalizedpatients, 80%had 25(OH)Ddeficiencyorinsufficiency.Inthesecondgroup, con-sisting ofoutpatients, lower values– albeitstill significant – were observed: around 55%insufficiency or deficiencyin serumlevels,whicharesimilartothosefoundinthecontrol groupofthepresentstudy.
Femaleshadsignificantlylowerlevelsof25(OH)Dinboth groups of the present study, demonstrating the predomi-nanceofthishypovitaminosisinwomen,afeaturerecognized by many authors.In a reviewstudy, Pattonet al. reported that 25(OH)D levels were comparatively lower in women, regardlessofthecut-offcriteriaused.6,13–18Labronicietal.,18
when assessing post-menopausal women, found that 82% of the patients had 25(OH)D levels considered insufficient. Severalstudieshavereportedagradualdeclineofthis vita-min’s levels aftermenopause,which ismoresignificant in olderpatients.Cauleyetal.,19inastudyofover90,000
post-menopausal women,observedaprevalenceoflowlevelsof 25(OH)D amongthese patients, as well as the subsequent increaseintheriskassociatedwithPFF,suggestingserum con-trolinpost-menopausalpatientsasmethodtoinvestigatethis risk.16,17,19–21
Despitethepredominanceinfemales,malesfromthe frac-turegroupalsopresentedserumlevelsconsideredinsufficient (25.67ng/mL)inthepresentstudy.Inaprospectivestudyof 1,608 elderly males,Cauleyet al.22 demonstrated a
signifi-cantincreaseintheriskofhipfracturesinpatientswithlow levelsof25(OH)D.Theriskoffracturewassignificantonlyin malepatientswithdeficientserumlevels,whichwas associ-atedwithbothPFF23andbonemineraldensityoftheproximal
femur.24
Inthe presentstudy,theassociationbetweenvitaminD deficiencyandtheagevariablewassignificantonlyinpatients agedbetween71and75years(p=0.003)andover80(p=0.003). Ensrudetal.,24consideringonlythemalepopulation,found
a significant association between boneloss and low levels of25(OH)D amongthose agedover75 years.Someauthors consider that 25(OH)D levels could present an uneven dis-tribution, characterizedby a stable pattern after a certain age.17–19Inthepresentstudy,adivisionaccordingtoageofthe
patientswasmadeinordertodiscriminatetheriskincertain agegroups.However,nootherstudieswiththismethodology wereretrieved,hinderingapropercomparison.Thevariable ethnicitypresentedaninsufficientsample,alimitationalso found by many authors in their analysis19,25 Nevertheless,
someauthorsconsiderthatgreaterskinpigmentationdueto geneticfactorsmayberelatedtolowerserumlevelsofvitamin D.12,19,25
Chapuy et al.,8 in a classic clinical trial conducted in
vitaminisrecognizedbymanyauthorsasanimportantfactor inpreventingfractures,especiallyPFF.1–4
Themainstrengthofthepresentsamplewasits consider-ablesizeof341patients.Inthemeta-analysisperformedbyLai etal.,11ofthe15case–controlstudieswithvaluesof25(OH)D
consideredsignificantinelderlyPFF,onlythreeshowedatotal samplehigherthanthatofthepresentstudy.Evenwithagood sample,onebiasofthepresentstudywasthenon-seasonal characterizationofthecollectionyear,sincesunexposureis knowntobeassociatedwithlevelsof25(OH)D,beingrelevant eveninrelationtotheinadequateintakeofthis vitamin.11
Thetimeofserumcollectionof25(OH)D,whichwasmadeat admissionbytransferfromanotherinstitutionandshowed variations,mayalsobeconsideredalimitationofthepresent study.Furthermore,the study didnot considerthe clinical andmetabolicsituationspresentedbythepatientwho under-wenttheexam,suchaschangesinkidneyorliverfunction, hormonalchangesinthyroidfunction,andmedicationuse, amongothers.However,despiterepresentingsourcesofbias, suchsituations couldconstitute confoundingfactorstothe varioustypesofvariablestobeconsidered.10,11
Conclusion
LowerlevelsofvitaminD3wereobservedinelderlypatients withPFFwhencomparedwithcontrolpatientswithout frac-ture. Significantly lower levels of this vitamin in female patientswereobservedinbothgroups.Therewasasignificant associationbetweentheriskofthishypovitaminosiswithPFF intheagerangesbetween71and75yearsandabove80years. ThesefindingsdemonstratetheimportantroleofvitaminD3 intheoutcomeofPFF;itswidespreaduseissuggestedasa waytopreventthiscondition.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. FernandesRA,AraújoDV,TakemotoMLS,SaubermanMV. Fraturasdofêmurproximalnoidoso:estudodecustoda doenc¸asobaperspectivadeumhospitalpúbliconoRiode Janeiro,Brasil.Physis.2011;21(2):395–416.
2. RicciG,LongarayMP,Gonc¸alvesRZ,UngarettiNetoAS, ManenteM,BarbosaLBH.Avaliac¸ãodataxademortalidade emumanoapósfraturadoquadrilefatoresrelacionadosà diminuic¸ãodasobrevidanoidoso.RevBrasOrtop.
2012;47(3):304–9.
3. MadsenCM,JorgensenHL,LindB,OgarrioHW,RiisT, SchwarzP,etal.Secondaryhyperparathyroidismand mortalityinhipfracturepatientscomparedtoacontrolgroup fromgeneralpractice.Injury.2012;43(7):1052–7.
4. BortolonPC,deAndradeCLT,deAndradeCAF.Operfildas internac¸õesdoSUSparafraturaosteoporóticadefêmurem idososnoBrasil:umadescric¸ãodotriênio2006-2008.Cad SaúdePública.2011;27(4):733–42.
5. deCastroLC.OsistemaendocrinológicovitaminaD.ArqBras EndocrinolMetab.2011;55(8):566–75.
6.PattonCM,PowellAP,PatelAA.VitaminDinorthopaedics.J AmAcadOrthopSurg.2012;20(3):123–9.
7.HolickMF.VitaminDdeficiency.NEnglJMed. 2007;357(3):266–81.
8.ChapuyMC,ArlotME,DuboeufF,BrunJ,CrouzetB,ArnaudS, etal.VitaminD3andcalciumtopreventhipfracturesinthe elderlywomen.NEnglJMed.1992;327(23):1637–42.
9.KhajuriaDK,RazdanR,MahapatraDR.Medicamentosparao tratamentodaosteoporose:revisão.RevBrasReumatol. 2011;51(4):365–82.
10.RoddamAW,NealeR,ApplebyP,AllenNE,TipperS,KeyTJ. Associationbetweenplasma25-hydroxyvitaminDlevelsand fracturerisk:theEPIC-Oxfordstudy.AmJEpidemiol. 2007;166(11):1327–36.
11.LaiJK,LucasRM,ClementsMS,RoddamAW,BanksE.Hip fractureriskinrelationtovitaminDsupplementationand serum25-hydroxyvitaminDlevels:asystematicreviewand meta-analysisofrandomisedcontrolledtrialsand
observationalstudies.BMCPublicHealth.2010;10:331. 12.RamasonR,SelvaganapathiN,IsmailNH,WongWC,
RajamoneyGN,ChongMS.Prevalenceofvitaminddeficiency inpatientswithhipfractureseeninanorthogeriatricservice insunnysingapore.GeriatrOrthopSurgRehabil.
2014;5(2):82–6.
13.BrowneJG,HealyM,MaherN,CaseyMC,WalshJB.High prevalenceofvitaminDdeficiencyinIrishpatientswithhip fracture.JGerontolGeriatRes.2013;2:1–6.Availablefrom: http://www.omicsgroup.org/journals/high-prevalence-of- vitamin-d-deficiency-in-irish-patients-with-hip-fracture-2167-7182.1000137.pdf.
14.GumieroDN,PereiraGJC,MinicucciMF,RicciardiCEI, DamascenoER,FunayamaBS.Associac¸ãodadeficiênciade vitaminaDcommortalidadeemarchapós-operatóriaem pacientecomfraturadefêmurproximal.RevBrasOrtop. 2015;50(2):153–8.
15.SaraivaGL,CendorogloMS,RamosLR,AraújoLMQ,Vieira JGH,MaedaSS,etal.Prevalênciadadeficiência,insuficiência devitaminaDehiperparatireoidismosecundarioemidosos institucionalizadosemoradoresnacomunidadedacidadede SãoPaulo,Brasil.ArqBrasEndocrinolMetab.
2007;51(3):437–42.
16.SatoY,AsohT,KondoI,SatohK.VitaminDdeficiencyand riskofhipfracturesamongdisabledelderlystrokepatients. Stroke.2001;32(7):1673–7.
17.LookerAC.Serum25-hydroxyvitaminDandriskofmajor osteoporoticfracturesinolderU.S.adults.JBoneMinerRes. 2013;28(5):997–1006.
18.LabroniciPJ,BlunckSS,LanaFR,EstevesBB,FrancoJS, LabroniciPJ,etal.VitaminaDesuarelac¸ãocomadensidade mineralósseaemmulheresnapós-menopausa.RevBras Ortop.2013;48(3):228–35.
19.CauleyJA,LaCroixAZ,WuL,HorwitzM,DanielsonME,Bauer DC,etal.Serum25hydroxyvitaminDconcentrationsandthe riskofhipfractures:thewomen’shealthinitiative.Ann InternMed.2008;149(4):242–50.
20.RussoLAT,GregórioLH,LacativaPGS,MarinheiroLP. Concentrac¸ãoplasmáticade25hidroxivitaminaDem mulheresnapós-menopausacombaixadensidademineral óssea.ArqBrasEndocrinolMetabol.2009;53(9):
1079–87.
21.BandeiraF,GrizL,FreeseE,LimaDC,ThéAC,DinizET,etal. DeficiênciadevitaminaDesuarelac¸ãocomadensidade mineralósseaemmulheresnapós-menopausaresidentes nostrópicos.ArqBrasEndocrinolMetab.2010;54(2):227–32. 22.CauleyJA,ParimiN,EnsrudKE,BauerDC,CawthonPM,
23.MelhusH,SnellmanG,GedeborgR,BybergL,BerglundL, MallminH,etal.Plasma25-hydroxyvitaminDlevelsand fractureriskinacommunity-basedcohortofelderlymenin Sweden.JClinEndocrinolMetab.2010;95(6):2637–45. 24.EnsrudKE,TaylorBC,PaudelML,CauleyJA,CawthonPM,
CummingsSR,etal.Serum25-hydroxyvitaminDlevelsand
rateofhipbonelossinoldermen.JClinEndocrinolMetab. 2009;94(8):2773–80.