w w w . r b o . o r g . b r
Original
Article
Radiological
analysis
on
femoral
tunnel
positioning
between
isometric
and
anatomical
reconstructions
of
the
anterior
cruciate
ligament
夽
,
夽夽
Rodrigo
Barreiros
Vieira
∗,
Leonardo
Augusto
de
Pinho
Tavares,
Rodrigo
Campos
Pace
Lasmar,
Fernando
Amaral
da
Cunha,
Lucas
Araujo
de
Melo
Lisboa
OrthopedicsandTraumatologyService,FaculdadedeCiênciasMédicasdeMinasGerais,HospitalUniversitárioSãoJosé,BeloHorizonte, MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24February2012 Accepted8February2013 Availableonline25March2014
Keywords:
Knee
Anteriorcruciateligament Reconstructivesurgicalprocedures
a
b
s
t
r
a
c
t
Objective:theaimofthisstudywastoradiologicallyevaluatethefemoraltunnelposition inanteriorcruciateligament (ACL)reconstructions usingtheisometricandanatomical techniques.
Methods:aprospectiveanalyticalstudywasconductedonpatientsundergoingACL recon-structionbymeansoftheisometricandanatomicaltechniques,usinggraftsfromtheknee flexortendonsorpatellartendon.Twenty-eightpatientswererecruitedduringthe immedi-atepostoperativeperiod,atthekneesurgeryoutpatientclinicofFCMMG-HUSJ.Radiographs oftheoperatedkneewereproducedinanteroposterior(AP)viewwiththepatientstanding onbothfeetandinlateralviewwith30◦offlexion.Thelinesweretracedoutandthe dis-tancesandanglesweremeasuredonthelateralradiographtoevaluatethesagittalplane. Thedistancefromthecenterofthescrewtotheposteriorcorticalboneofthelateralcondyle wasmeasuredanddividedbytheBlumensaatline.Inrelationtotheheightofthescrew,the distancefromthecenterofthescrewtothejointsurfaceofthelateralcondyleoftheknee wasmeasured.OntheAPradiograph,evaluatingthecoronalplane,theanglebetweenthe anatomicalaxisofthefemurandalinetracedatthecenterofthescrewwasmeasured.
Results:withregardtothepmeasurement(posteriorizationoftheinterferencescrew),the testsshowedthatthep-value(0.4213)wasgreaterthanthesignificancelevelused(0.05); thenullhypothesiswasnotrejected anditcouldbestated thatthere wasno statisti-callysignificantdifferencebetweentheanatomicalandisometrictechniques.Withregard totheHmeasurement(heightofthescrewinrelationtothelowercorticalboneofthe knee),thep-valueobserved(0.0006)waslessthanthesignificancelevelused(0.05);the nullhypothesiswasrejectedanditcouldbestatedthattherewasastatisticallysignificant differencebetweentheanatomicalandisometrictechniques.Itcanbeconcludedthatthe
夽
Pleasecitethisarticleas:VieiraRB,dePinhoTavaresLA,PaceLasmarRC,daCunhaFA,deMeloLisboaLA.Análiseradiológicado posicionamentodotúnelfemoralcomastécnicasdereconstruc¸ãoisométricaoudereconstruc¸ãoanatômicadoLCA.RevBrasOrtop. 2014;49:160–166.
夽夽
WorkperformedattheFaculdadedeCiênciasMédicasdeMinasGerais,HospitalUniversitárioSãoJosé(FCMMG-HUSJ),BeloHorizonte, MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.B.Vieira).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
latterdifferenceoccurredbecausetheisometrictechniquegeneratedgreatervaluesforthe Hmeasurementthantheanatomicaltechnique.WithregardtotheMEDvariable(positionof thescrewontheAPradiograph),theobservedp-value(0.000)waslessthanthesignificance level(5%);thenullhypothesiswasrejectedanditcouldbestatedwith95%confidencethat therewasasignificantdifferencebetweentheanatomicalandisometrictechniques.
Conclusions: therewerestatisticallysignificantdifferencesintheradiologicalevaluations ofthe femoraltunnel,both inthe sagittaland inthecoronal plane,betweentheACL reconstructiontechniques.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Análise
radiológica
do
posicionamento
do
túnel
femoral
com
as
técnicas
de
reconstruc¸ão
isométrica
ou
de
reconstruc¸ão
anatômica
do
LCA
Palavras-chave:
Joelho
Ligamentocruzadoanterior Procedimentoscirúrgicos reconstrutivos
r
e
s
u
m
o
Objetivo:avaliarradiologicamenteaposic¸ãodotúnelfemoralnareconstruc¸ãodoligamento cruzadoanteriorpelastécnicasisométricaeanatômica.
Métodos: foifeitoestudoanalíticoprospectivoempacientessubmetidosàreconstruc¸ãodo ligamentocruzadoanterior(LCA),pormeiodatécnicaisométricaeanatômica,comousode enxertodetendõesflexoresdojoelhooudetendãopatelar.Foramcaptados28pacientes,em pós-operatórioimediato,noambulatóriodecirurgiadojoelhodaFCMMG-HUSJ.Foramfeitas radiografiasdojoelhooperadonasincidênciasemanteroposterior(AP)comapoiobipodálico eperfilem30◦deflexão.Foramtrac¸adasaslinhasemedidososânguloseasdistâncias naradiografiaemperfilparaavaliaroplanosagital.Foimedidaadistânciadocentrodo parafusoàcorticalposteriordocôndilolateraledivididopelalinhadeBlumensaat.Com relac¸ãoàalturadoparafuso,foimedidaadistânciadocentrodeleatéasuperfíciearticular docôndilolateraldojoelho.NaradiografiaemAP,queavaliaoplanocoronal,mede-sea angulac¸ãoentreoeixoanatômicodofêmureumalinhatrac¸adanocentrodoparafuso.
Resultados: pelostestes,op-valor(0,4213)émaiordoqueoníveldesignificânciaadotado (0,05),ahipótesenulanãoérejeitadaepodeserafirmadoquenãohádiferenc¸a estatistica-mentesignificativaentreastécnicasanatômica(TAN)eisométrica(TIS)noquedizrespeito àMedidaP(posteriorizac¸ãodoparafusodeinterferência).Comoop-valor(0,0006)observado émenordoqueoníveldesignificânciaadotado(0,05),rejeita-seahipótesenulaepodeser afirmadoquehádiferenc¸aestatisticamentesignificativaentreaTANeaTISnoquediz respeitoàMedidaH(alturadoparafusoemrelac¸ãoàcorticalinferiordojoelho).Pode-se concluirqueessadiferenc¸aocorreporqueaTISgeravaloresmaioresparaaMedidaHdo queaTAN.Comoop-valorobservado(0,000)émenordoqueoníveldesignificância(5%), rejeitou-seahipótesenulaeafirmamoscom95%deconfianc¸aquehádiferenc¸asignificativa entreaTANeaTISnoquedizrespeitoàvariávelMED(posic¸ãodoparafusonaradiografia emAP).
Conclusões: houvediferenc¸aestatisticamentesignificativanaavaliac¸ãoradiológicadotúnel femoral,tantonoplanosagitalcomonocoronal,entreastécnicasdereconstruc¸ãodoLCA. ©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Reconstructionoftheanteriorcruciateligament(ACL)isone ofthe most frequently performed orthopedicsurgical pro-ceduresanditparticularlyaffectsyoungadults.Ithasbeen estimatedthatbetween75,000and100,000suchprocedures are carried out in the United States every year.1
Reestab-lishmentofkneebiomechanicsisthemainobjectiveofthe treatment, inorder toavoidearly degenerative alterations, with consequent reduction in work capacity and sports performance.
Overrecentdecades,thearthroscopicprocedureof intra-articularACLreconstructionhasbeen consideredtobethe
gold standardtreatmentbecauseofits lowmorbidity,with betterandfasterpostoperativeevolution.
In the 1990s, it was believed that the isometric arthro-scopic reconstruction technique forthe ACL, in which the neoligament maintains its lengththroughout the range of motionoftheknee,wouldmoreadequatelyrestorethe biome-chanicsofthisjoint.Thiswasachievedbyconstructingthe femoraltunnelatanorientationofcloseto12o’clock,which would make the graft vertical. Although this concept was partially true, with restoration of translational stability, a recent study revealed afailureto reachrotationalstability, withmaintenanceofthepivotshift.2Consequently,thejoint
In2003,Yasudaetal.3werethefirstofseveralauthorsto
studyanatomicalACLreconstructioningreaterdepth,with constructionofafemoraltunnel,ortunnelsinthecaseofa doubleband,atthepointwherethesebandsoriginate,inthe medialwallofthelateralfemoralcondyle.Somemorerecent studieshaveshownthat,withthisprocedure,both transla-tionalandrotationalstabilityareachieved,thusreproducing thebiomechanicalcharacteristicsofthekneefaithfully.4–6
Withregardtoevaluatingthepositioningofthefemoral tunnelaftertheoperation,therearesomestudiesinthe liter-atureshowingthatthisobjectivecanbeestablishedthrough radiologicalstudies.7–9
The aim of this study was to radiologically evaluate thepositionofthe femoraltunnelusingthe isometricand anatomicalreconstructiontechniques.
Materials
and
methods
Aprospectiveanalyticalstudywasconductedon28patients who underwent ACL reconstruction using grafts from the flexortendonsofthe kneeorfrom thepatellar tendon.All the procedures were performedby the same author (RBV). Fourteen patients underwent isometric reconstruction and theother14patientsunderwentanatomicalreconstruction; patients were allocated randomly. All ofthe patients were evaluated,beforeandaftertheoperation,atthekneesurgery outpatientclinic ofSão José University Hospital, School of MedicalSciences of MinasGerais(HUSJ-FCMMG), and they underwentthesurgicalprocedureinthesamehospital.The patients included in this study presented a condition of anteriorkneeinstabilitythathadbeendiagnosedboth clin-icallyandbymeans ofmagneticresonance examination,a closedgrowth plate intheproximaltibia anddistalfemur, and an age of less than 50 years. All the patients were referredthroughtheBrazilianNationalHealthSystem(SUS). We excluded patients who required corrective osteotomy during the reconstructive procedure, those with advanced osteoarthrosisandthosewithinjuriestoperipheralligament structuresoftheknee.Inthissample,27weremenandone wasawoman,andthemeanagewas32.5years(range:16–48). Therewere16patients(57.14%)withinjuriestotheleftknee and 12 (42.86%) to the right knee. All the patients under-wentradiologicalexaminationswithinthefirstpostoperative month.
Withfollow-upfromoneoftheauthors,thepatientswere referredforimagingexaminationsintheradiologysectorof HUSJ-FCMMG.Radiographswereperformed in anteroposte-rior(AP)viewontheoperatedknee,withweight-bearingon bothfeet,andinlateralviewatflexionof30◦.These
exami-nationsweredulyidentifiedwiththepatient’sname,thedate ofthesurgeryandthetechniqueused(isometricor anatomi-cal).Wetracedoutthelinesandmeasuredthedistancesand anglesinthefollowingmanner:onthelateralradiograph,the distancesfromthecenterofthescrewtotheposteriorcortical boneofthelateralcondyleandfromthecenterofthescrew totheanteriorcorticalboneweremeasured(Fig.1).In rela-tiontotheheightofthescrew,thedistancefromthecenter ofthescrewtothejointsurfaceofthelateralcondyleofthe kneewasmeasured(Fig.1).OntheAPradiograph,theangle
Fig.1–Theposteriorizationoftheinterferencescrew (measurementP)wasmeasuredbydividingthedistance betweenpoints1and2(posteriorcorticalbonetothe centerofthescrew)bythedistancebetween1and3(center ofthescrewtotheanteriorcorticalbone).Theheightofthe screwinrelationtothelowercorticalboneoftheknee (measurementH)wasalsomeasured,bymeansofthe distancebetween2and5.
betweentheanatomicalaxisofthefemurandalinetraced throughthecenterofthescrewwasmeasured(Fig.2).
Results
Table1presentsadescriptiveanalysisonthemeasurements P and H from the lateral view, stratified according to the technique used: anatomical technique (ANT) or isometric technique(IST).Itcouldbeseenthat,onaverage,thevalues
Table1–DescriptivestatisticsforthemeasurementsP andHaccordingtothetechniqueused.
Technique MeasurementP MeasurementH
ANT IST ANT IST
Count 14 14 14 14
Mean 0.4556 0.4352 0.2023 0.3119
Standarddeviation 0.1236 0.0835 0.1224 0.0583
Minimum 0.2370 0.3320 0.0570 0.2270
Firstquartile 0.3662 0.3858 0.1430 0.2615
Median 0.4525 0.4045 0.1855 0.3065
Thirdquartile 0.5435 0.4688 0.2122 0.3668
Fig.2–Theanglebetweentheanatomicalaxisofthefemur andthecenterofthescrewwasmeasuredin
anteroposterior(AP)view.TheangleMEDwasdefined.
foundformeasurementPusingANTwereslightlylargerthan thosefoundusingIST.Thesamewasfoundwiththestandard deviationsandmedians.
InthecaseofmeasurementH,it couldbeseenthatthe valuesfoundthroughusingISTwereonaveragegreaterthan thoseusingANTandalsopresentedlower variability,since thestandarddeviationwassmaller.
Fig.3showsahistogramofthe distributionof measure-mentPforANTandIST.ForANT,therewasaveryirregular distribution,andforIST,thedistributionwasasymmetricalto theright.
Fig.4showsahistogramofthe distributionof measure-mentHforANT andIST.Itcanbeseenthatthevaluesfor
ANThadasymmetricaldistributiontotheright,whileforIST, thedistributionwasapproximatelyuniform.
FromtheboxplotpresentedinFig.5, itcanbeseenthat thedistributionofmeasurementPwasconcentratedonclose valuesbothforANTandforIST.Aswasseenintheinitial descriptiveanalysis,theboxplotmadeitpossibletoseethat therewaslessvariabilityinISTthaninANT,sincethe“box” wassmaller.
RegardingmeasurementH,thedistributionofthevalues forANT wasconcentrated onsmallervaluesthan thoseof IST.Thisindicatesthattheremaybeasignificantdifference betweenthesetwotechniquesinrelationtomeasurementH. Tocheckthishypothesis,anappropriatestatisticaltestwas performed.
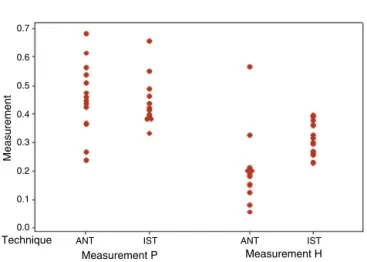
Fig. 6 presents a plot of the individual values of each measurement, to compare ANT and IST. Thisgraph ledto conclusionssimilartothosefromtheprecedinggraph.
Sinceasmallsamplewasusedtocomparemeasurements PandHinrelationtothetechniqueusedand,moreover,itwas seenthroughastatisticaltestthattheassumptionofnormal distribution ofthe datawasviolated, themostappropriate statisticaltestforevaluatingthe hypothesisofinterestwas thenonparametricMann–Whitneytest.
Thehypothesestobetestedwereasfollows:
Test1:measurementP.
H0:ANTandISTpresentthesamedistribution.
Ha:ANTandISTpresentdifferentdistributions.
Test2:measurementH.
H0:ANTandISTpresentthesamedistribution.
Ha:ANTandISTpresentdifferentdistributions.
Thesignificancelevelusedwas˛=0.05.
Test1:measurementP.
Estimateddifference:median(ANT)–median(IST)=0.0355. Confidenceintervalforthisdifference:(−0.0520;0.1050).
p-Value=0.4213.
Therefore,sincethep-value(0.4213)wasgreaterthanthe significance level used (0.05), the null hypothesis was not rejectedanditcouldbestatedthattherewasnostatistically significant difference betweenANT and IST withregard to measurementP.
9
8
7
6 5
4
3
2
1
0
0.4 0.3
0.3
0.4 0.5 0.6 0.7
0.7 0.6 0.5
Measurement P
ANT
Frequency
IST
Measurement H
ANT
Frequency
IST
0.08 0.16 0.24 0.32 0.40 0.48 0.56
6
5
4
3
2
1
0
0.08
0.16
0.24
0.32
0.40
0.48
0.56
Fig.4–HistogramofthemeasurementH,stratifiedaccordingtotechnique.
ANT IST Measurement P Technique
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Measurement
Measurement H ANT IST
Fig.5–BoxplotofthemeasurementsPandHaccordingto thesurgicaltechniqueused.
Test2:measurementH.
Estimateddifference:median(ANT)–median(IST)=−0.1275. Confidenceintervalforthisdifference:(−0.1820;−0.0710).
p-Valor=0.0006.
Sincethep-value(0.0006)wassmallerthanthesignificance levelused(0.05),thenullhypothesiswasrejectedanditcould bestatedthattherewasastatisticallysignificantdifference betweenANTandISTwithregardtomeasurementH.Itcould beconcludedthatthisdifferenceoccurredbecauseIST gener-atedlargervaluesformeasurementHthanANTdid.
AccordingtoTable2,thepatientsonwhomISTwasused presentedgreatermean valuesforthe variable MED,inAP view,andsmallervariability.
ItcanbeseenfromFig.7thatthemeasurementsobserved forthevariableMEDwereapparentlygreaterforthepatients onwhom ISTwas applied.However,ahypothesistestwas neededinordertoascertainwhetherthisdifferencewas sta-tisticallysignificant.
Fig.8showsthatthepatientsonwhomANTwasusedhad lowervaluesforthevariableMEDandgreatervariabilitythan thepatientsonwhomISTwasused.Again,thisprovedthe needforahypothesistestinordertoascertainwhetherthis differencewasstatisticallysignificant.
Measurement P Measurement H
Technique
Measurement
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
ANT IST
ANT IST
Fig.6–IndividualvaluesforthemeasurementsPandH, accordingtothetechnique
50
40
30
20
10
ANT IST
Technique
MED
Fig.7–BoxplotforthevariableMED.
Table2–DescriptivestatisticsforthevariableMED.
Variable Technique N Mean Standarddeviation Minimum Q1 Median Q3 Maximum
MED ANT 14 26.93 8.51 12.00 20.75 27.50 31.25 42.00
IST 14 42.21 6.78 25.00 39.00 42.00 48.50 51.00
50
Technique
MED
40
30
20
10
ANT IST
Fig.8–IndividualvaluesforMED.
therewasasignificantdifferencebetweenANTandISTwith regardtothevariableMED.
It could also be stated, with 95% confidence, that the patientsonwhomISTwasappliedpresentedresultsforMED thatonaveragewere16.74times[CI(21.93;11.55)]greaterthan amongthosewithANT.
Discussion
The importance of correct positioning of both the tibial and the femoral tunnel in ACL reconstruction cannot be underestimated. Poor positioning of the tunnels is a very common mistake in ACL reconstruction, and the possible problemsincludediminishedrange ofmotionofthe knee, graftfailure,impactingofthegraftontheintercondylarroof and continuation of feelings of instability, which generate revisionsurgicalproceduresthat oftenpresentmajor com-plexity. Since the center of rotation of the knee is closer tothefemoralinsertionthan tothetibialinsertion,greater accuracyoftunnel placement in the femur, in ACL recon-struction, is more critical than tibial tunnel positioning.10
For this reason, our study onlyaddressed analysis of this tunnel.
Inmostorthopedicsurgicalproceduresinvolvingthebone structure, radiological parameters that have already been welldefinedguidecriticalanalysisontheircorrectnessand the possible technical mistakes that could affect the final result.ThisisnotthecasewithregardtoACLreconstruction; althoughsomestudiesintheworldwideliteraturehaveshown differentmethodsforradiologicallypositioningofthefemoral tunnel,9–12noneofthemhasbeenshowntobeeffectiveorhas
becomewidelydisseminated.
Overafive-yearfollow-upon89patientswhounderwent ACLreconstructionusingvideo-assistedarthroscopy,Aglietti etal.13demonstratedthat88%ofthekneeswithcorrect
posi-tioningofthefemoraltunnelpresentedsatisfactorystability. However,anteriorpositioningofthefemoraltunnelwas asso-ciatedwithafailurerateof62.5%.Khalfayanetal.14showed
that 79%ofthe caseswithpositioning ofthe femoral tun-nelentrancewithintheposterior40%portionofthe lateral condyleofthe femurpresentedgood resultsusingthe KT-1000arthrometer(upto3mmofanteriorization).Inourstudy, theISTcameclosertotheresultsofthepreviousauthor,with ameanof0.4352or43%posteriortothemeasurement, ver-sus0.4556or45%,and thuswasslightlymoreanteriorized. Thisisthereasonwhy,withthesingle-bandANT,thefemoral tunnelwasconstructedatthebifurcatedcrest,betweenthe insertionsofthefibersoftheanteromedialandposterolateral bandsoftheACL,i.e.alittlemoreanteriorizedthanwhatwas usedinalltheotherarticlesanalyzed,whichusedthe antero-medialbandasthepointatwhichthetunnelshouldbemade inthefemur.
Inourstudy,itwasshownthatintworegardsofthe posi-tioning(heightandangleinthefrontalplane),thetranstibial accessproducedresultsthatweresignificantlydifferentfrom thoseobtainedusingamedialportal.Thisdivergesfromthe studybyGironetal.,inwhichtheystatedthattheyreachedthe “ideal”pointonthefemurboththroughanout-inortranstibial accessandthroughananteromedialapproach.15
Recently,Shahetal.16conductedaradiographicevaluation
on43patientswhounderwentanatomicalACLreconstruction usingtheanteromedialportaltechniqueandtheyfoundthat theinterferencescrewwaslocatedonthefemurat approxi-mately31%ofthesagittaldiameterinrelationtotheposterior corticalboneandat25%oftheheightofthelateralfemoral condyle.
Inaradiographicanalysisonbonetunnelpositioningin ACLreconstructionthatcomparedtheopentechniquewith arthroscopyviaananteromedialportal,Dambrósetal.8found
adifferencebetweenthetwotechniquesregardingthe posi-tioningofthefemoraltunnel.Thearthroscopicrouteshowed greaterprecisionintunnelpositioning,andthisdifferencewas showntobestatisticallysignificant.Wealsoobserveda differ-enceinourstudyinrelationtofemoraltunnelpositioning,but weonlyusedarthroscopictechniques.
Bernardetal.17demonstratedthatthepositioningofthe
interferencescrewinthecondylewasat28.5%oftheheight ofthe lateral femoralcondyle, using thequadrant method describedintheiroriginalstudy,whichusedtheanteromedial portaltechnique.
Inourresult,inmeasuringtheheightofthelateralfemoral condyleinrelationtotheBlumensaatline, themeanvalue forISTwas20.2%andforANTwas31.1%.Functional evalu-ationswithlong-termfollow-upareneededinordertomake comparisonsregardingthebestsurgicaltechnique,since con-clusionscannotbereachedusingradiographicevaluationof tunnelposition.
Inrelationtothefrontalplane,ourcalculationsshowed that the mean difference between the tunnel angles was 16.74◦. The angle in the anatomical reconstruction was
byAgliettietal.,18whoin1995publishedapapershowinga
differenceof18◦betweenthetunnels.
Furtherimagingstudiescorrelatedwithfunctionalstudies arestillawaited,inordertoaffirmwhichradiographic param-etersarecorrectforfemoraltunnelpositioning.
Certainlimitationsofthepresentstudyneedtobe high-lighted.Theradiographsthatwereanalyzedinrelationtoour patientswereproducedusingdifferentradiologytechniques, withfollow-upbyoneoftheauthors.Consequently,theywere notperformedinablindedmanner,whichmighthaveledto bias.Therealpositioningofthegraftinsidethebonetunnel couldnotbecompletelyviewedontheradiographicimaging; onlythe positioningofthe screwcouldbeseen.Lastly,the samplesizewassmall.
Conclusion
Thepositioningofthefemoraltunnelonradiological exami-nationpresentedresultsthatwereverysimilarinrelationto posteriorizationonthefemoralcondyle,independentofthe techniqueused.However,thereweresignificantdifferences inheightandangleinrelationtothefemoralaxis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. GriffinLY,AgelJ,AlbohmMJ,ArendtEA,DickRW,GarrettWE, etal.Non-contactanteriorcruciateligamentinjuries:risk factorsandpreventionstrategies.JAmAcadOrthopSurg. 2000;8(3):141–50.
2. JonssonH,Riklund-AhlströmK,LindJ.Positivepivotshift afterACLreconstructionpredictslaterosteoarthrosis:63 patientsfollowed5-9yearsaftersurgery.ActaOrthopScand. 2004;75(5):594–9.
3. YasudaK,KondoE,IchiyamaH,KitamuraN,TanabeY, TohyamaH,MinamiA.Anatomicreconstructionofthe anteromedialandposterolateralbundlesoftheanterior cruciateligamentusinghamstringtendongrafts. Arthroscopy.2004;20(10):1015–25.
4. YagiM,WongEK,KanamoriA,DebskiRE,FuFH,WooSL. Biomechanicalanalysisofananatomicanteriorcruciate ligamentreconstruction.AmJSportsMed.2002;30(5):660–6.
5. GabrielMT,WongEK,WooSL,YagiM,DebskiRE.Distribution ofinsituforcesintheanteriorcruciateligamentinresponse torotatoryloads.JOrthopRes.2004;22(1):85–9.
6.VanEckCF,LesniakBP,SchreiberVM,FuFH.Anatomic single-anddouble-bundleanteriorcruciateligamentreconstruction flowchart.Arthroscopy.2010;26(2):258–68.
7.KondoE,YasudaK,IchiyamaH,AzumaC,TohyamaH. Radiologicevaluationoffemoralandtibialtunnelscreated withthetranstibialtunneltechniqueforanatomic double-bundleanteriorcruciateligamentreconstruction. Arthroscopy.2007;23(8):869–76.
8.DambrósJM,FlorêncioR,LopesJúniorOV,KuhnA,SagginJ, SpinelliLF.Análiseradiológicadoposicionamentodostúneis ósseosnacirurgiadereconstruc¸ãodoligamentocruzado anterior:comparac¸ãoentreastécnicasabertaeartroscópica viaportalanteromedial.RevBrasOrtop.2001;46(3):
270–5.
9.AgliettiP,ZaccherottiG,MenchettiPP,DeBiaseP.A
comparisonofclinicalandradiologicalparameterswithtwo arthroscopictechniquesforanteriorcruciateligament reconstruction.KneeSurgSportsTraumatolArthrosc. 1995;3(1):2–8.
10.GuoL,YangL,WangAM,WangXY,DaiG.Roentgenographic measurementstudyforlocatingfemoralinsertionsiteof anteriorcruciateligament:acadavericstudywithX-Caliper. IntOrthop.2009;33(1):133–7.
11.AmisAA,BeynnonB,BlankevoortL,ChambatP,ChristelP, DurselenL,etal.ProceedingsoftheESSKAscientific workshoponreconstructionoftheanteriorandposterior cruciateligaments.KneeSurgSportsTraumatolArthrosc. 1994;2(3):124–32.
12.HarnerCD,MarksPH,FuFH,IrrgangJJ,SilbyMB,MengatoR. Anteriorcruciateligamentreconstruction:endoscopicversus two-incisiontechnique.Arthroscopy.1994;10(5):
502–12.
13.AgliettiP,BuzziR,GironF,SimeoneAJ,ZaccherottiG. Arthroscopic-assistedanteriorcruciateligament reconstructionwiththecentralthirdpatellartendon.A 5-8-yearfollow-up.KneeSurgSportsTraumatolArthrosc. 1997;5(3):138–44.
14.KhalfayanEE,SharkeyPF,AlexanderAH,BrucknerJD,Bynum EB.Therelationshipbetweentunnelplacementandclinical resultsafteranteriorcruciateligamentreconstruction.AmJ SportsMed.1996;24(3):335–41.
15.GironF,BuzziR,AgliettiP.Femoraltunnelpositioninanterior cruciateligamentreconstructionusingthreetechniques.A cadaverstudy.Arthroscopy.1999;15(7):750–6.
16.ShahAA,BrienA,LoweWR.Radiographicresultsoffemoral tunneldrillingthroughtheanteromedialportalinanterior cruciateligamentreconstruction.Arthroscopy.
2010;26(12):1586–92.
17.BernardM,HertelP,HornungH,CierpinskiT.Femoral insertionoftheACL.Radiographicquadrantmethod.AmJ KneeSurg.1997;10(Winter(1)):14–21.