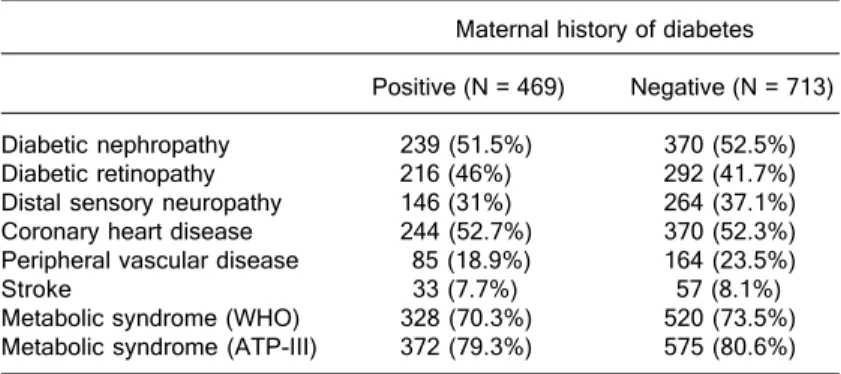
The prevalence of chronic diabetic complications and metabolic syndrome is not associated with maternal type 2 diabetes
Texto
Imagem
Documentos relacionados
Figure 1.8: Diagram of insulin resistance as a core feature for the development of type 2 diabetes and a risk factor for both cardiovascular and metabolic complications
Objective: To investigate the presence of maternal and paternal history of type 2 diabetes mellitus (DM) in relatives of 644 type 2 diabetic patients from Southern
Also, lipodystrophy and metabolic complications associated with insulin resistance have been reported in Mandibuloacral Dysplasia (18), and some affected patients were found to
To evaluate the prevalence of chronic vascular complications and associated factors in patients with type 1 diabetes mellitus (DM).. Cross-sectional study with type 1
pathways and processes providing a putative molecular basis for the association of diabetes with hypertension. Type-2 diabetic patients with a history of taking
Background: The presence of cardiac autonomic neuropathy (CAN) in patients with diabetes mellitus (DM) is associated with increased mortality and chronic microvascular complications
Summary of the findings: The metabolic syndrome is characterized by insulin resistance and the presence of risk factors for cardiovascular diseases and diabetes mellitus type
Objectives : To implement actions of evaluation and guidelines for patients with type 2 DM who attend a Family Health Strategy (FHS), regarding diabetic foot and the practice
