www.jped.com.br
REVIEW
ARTICLE
Sialorrhea
in
children
with
cerebral
palsy
夽
,
夽夽
Bruno
Leonardo
Scofano
Dias
a,∗,
Alexandre
Ribeiro
Fernandes
b,
Heber
de
Souza
Maia
Filho
caRedeSARAHdeHospitaisdeReabilitac¸ão,SetordeReabilitac¸ãoInfantil,RiodeJaneiro,RJ,Brazil
bUniversidadeFederalFluminense(UFF),Niterói,RJ,Brazil
cUniversidadeFederalFluminense(UFF),ProgramadeMestradoProfissionalemSaúdeMaterno-Infantil,Niterói,RJ,Brazil
Received28February2016;accepted9March2016 Availableonline6June2016
KEYWORDS
Sialorrhea;
Cerebralpalsy;
Child
Abstract
Objective: Toreviewtheliteratureonsialorrheainchildrenwithcerebralpalsy.
Sourceofdata: Non-systematicreviewusingthekeywords‘‘sialorrhea’’and‘‘child’’carried
outinthePubMed®,LILACS®,andSciELO®databasesduringJuly2015.Atotalof458articles
wereobtained,ofwhich158wereanalyzedastheywereassociatedwithsialorrheainchildren;
70 had contentrelated to sialorrhea incerebralpalsy orthe assessmentandtreatment of
sialorrheainotherneurologicaldisorders,whichwerealsoassessed.
Datasynthesis: Theprevalenceofsialorrheaisbetween10%and58%incerebralpalsyandhas
clinicalandsocialconsequences.Itiscausedbyoralmotordysfunction,dysphagia,and
intra-oralsensitivitydisorder.Theseverityandimpactofsialorrheaareassessedthroughobjective
orsubjectivemethods. Severaltypes oftherapeuticmanagementaredescribed:trainingof
sensoryawarenessandoralmotorskills,drugtherapy,botulinumtoxininjection,andsurgical
treatment.
Conclusions: Themosteffectivetreatmentthataddressesthecauseofsialorrheainchildren
withcerebralpalsyistrainingofsensoryawarenessandoralmotorskills,performedbyaspeech
therapist.Botulinumtoxininjectionandtheuseofanticholinergicshaveatransienteffectand
areadjuvanttospeechtherapy;theyshouldbeconsideredincasesofmoderatetosevere
sial-orrheaorrespiratorycomplications.Atropinesulfateisinexpensiveandappearstohavegood
clinicalresponsecombinedwithgoodsafetyprofile.Theuseoftrihexyphenidylforthe
treat-mentofsialorrheacanbeconsideredindyskineticformsofcerebralpalsyorinselectedcases.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
夽
Pleasecitethisarticleas:ScofanoDiasBL,FernandesAR,MaiaFilhoHS.Sialorrheainchildrenwithcerebralpalsy.JPediatr(RioJ). 2016;92:549---58.
夽夽
StudycarriedoutatRedeSARAHdeHospitaisdeReabilitac¸ão,RiodeJaneiro,RJ,Brazil.
∗Correspondingauthor.
E-mail:[email protected](B.L.ScofanoDias). http://dx.doi.org/10.1016/j.jped.2016.03.006
PALAVRAS-CHAVE
Sialorreia;
Paralisiacerebral;
Crianc¸a
Sialorreiaemcrianc¸ascomparalisiacerebral
Resumo
Objetivo: Revisaraliteraturareferenteasialorreiaemcrianc¸ascomparalisiacerebral. Fontededados: Revisãonãosistemáticautilizandoaspalavras-chave‘‘sialorreia’’e‘‘crianc¸a’’
realizadanasbasesdedadosPubmed®,Lilacs®eScielo®emjulhode2015.Foram
recuper-ados458artigos,158foramanalisadosporteremrelac¸ãocomsialorreiaemcrianc¸as,70com
conteúdorelativoàsialorreianaparalisiacerebralouaavaliac¸ãoetratamentodasialorreia
emoutrosdistúrbiosneurológicosforamaproveitados.
Síntesedosdados: Asialorreiatemprevalênciaentre10%e58%naparalisiacerebraleimplica
emconsequênciasclínicasesociais.Écausadapordisfunc¸ãomotoraoral,disfagiaedistúrbioda
sensibilidadeintraoral.Agravidadeeoimpactodasialorreiasãoavaliadosatravésdemétodos
objetivosousubjetivos. Estãodescritasdiversasformasdemanejoterapêutico:treino para
consciênciasensorial ehabilidadesmotoras orais,terapia farmacológica,injec¸ão de toxina
botulínicaetratamentocirúrgico.
Conclusões: Otratamentomais eficaze queaborda acausadasialorreia nascrianc¸ascom
paralisiacerebraléotreinoparaconsciênciasensorialehabilidadesmotorasorais,realizadopor
umfonoaudiólogo.Injec¸ãodetoxinabotulínicaeousodeanticolinérgicostêmefeitotransitório
esãoauxiliaresaotratamentofonoaudiológicooudevemserconsideradasnoscasosdesialorreia
moderadaagraveoucomcomplicac¸õesrespiratórias.Osulfatodeatropinatem baixocusto
epareceterboarespostaclínicacombomperfildeseguranc¸a.Ousodetriexifenidilparao
tratamentodasialorreiapodeserconsideradonasformasdiscinéticasdeparalisiacerebralou
emcasosselecionados.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo
OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Sialorrheaistheinvoluntarylossofsalivaandoralcontent1,2
that usually occurs in infants; however, at 24 months of age children with typical development should have the ability to perform most activities without loss of saliva.3
Aftertheageof4years,sialorrheaisabnormalandoften persistsin children withneurological disorders, including neuromuscular incoordination of swallowing and intellec-tual disabilities.1 The term cerebral palsy (CP) describes
agroupofmovement andposture developmentdisorders, withactivityrestrictionsormotordisabilitiescausedby mal-formationsorinjuriesthatoccurinthedevelopingfetalor child’sbrain.4,5Worldwide,theprevalenceofCPis1---5per
1000 livebirths, representing the most commoncause of motordisabilityinchildren.6 The prevalenceof sialorrhea
inCPisseldomstudied,andtheresultscannotbecompared duetovariationinthestudydesignsandpatientselection.1
Someauthorsreportedaprevalenceof10---58%,7---10 thusit
isreasonabletoacceptthatoneinthreepatientswithCP hasdroolingatsomedegree.1
Althoughunderestimated,sialorrheaimpliesclinicaland socialconsequencesandhasseveralimpactsrelatedtothe overallhealthofchildrenwithCP,regardingdysphagiaand respiratoryhealth,theirsocio-emotionaldevelopment,and emotionalandworkoverloadforfamiliesandcaregivers.
This non-systematic review aimstoupdate the profes-sionalsinvolvedinthecareofchildrenwithCPinrelation totheliteratureonsialorrheainthesepatients;itwas car-riedoutusingthekeywords‘‘sialorrhea’’and‘‘child’’inthe
PubMed®,LILACS®,andSciELO®databasesduringJuly2015. A totalof 458articles wereretrieved,of which158 were analyzed, astheywere associatedwithsialorrheain chil-dren;70wererelatedtosialorrheaincerebralpalsyorthe assessmentandtreatmentofsialorrheainotherneurological disorders,whichwerealsoassessed.
Physiologyofsalivation
The parotidglands producemoreserous, waterysalivaas
a result of stimulation during meals. The sublingual and
submandibular glands produce more viscous saliva, more
constantly, throughout the day.11,12 On average, a person
swallows approximately 600mL of saliva every day; how-ever, in some individuals, this volume can reach up to 1000mL/day.11 Afferents of thefifth, seventh,ninth, and
regulatory mechanism as part of encephalopathy in CP.11
Sialorrheamayvaryfromminutetominute, dependingon factors suchashunger, thirst, fatigue,anxiety,emotional state,andthecircadianrhythmofsalivaryproduction.1
Predisposingfactors,physiopathology,andetiology
Reid et al. analyzed the predisposing factors of
sialor-rhea in children with CP (385 individuals) aged
7---14 years of age, which include thefollowing: non-spastic
types, thequadriplegic topographical pattern,absenceof
cervical control, severe difficulties in gross motor
coor-dination/function, epilepsy, intellectual disability, lack of
speech,openanteriorbite,anddysphagia.13
Currently, itis widely accepted that sialorrheain chil-drenwithCPis notcausedbyhypersalivation,butbyoral motor dysfunction,dysphagia, and/or intraoral sensitivity disorder.1,3,9,11,12 Senneretal.publishedastudythat
com-paredgroups of children withCP withsialorrhea (n=14); children with CPwithout sialorrhea (n=14), and children withnormalneurodevelopment(n=14)through quantifica-tionofsalivausingtheSaxontestdescribedbyKohleretal. in1985;14theresultsshowedlowerscoresinoralmotor
func-tionwithout excesssalivaproductionintheCPgroupwith sialorrhea,suggestingthatthehypersalivationisnotoneof thefactorsresponsibleforsialorrheainCP.3Erasmusetal.
studiedgroupsofchildrenwithCP(n=100)andhealthy chil-dren(n=61)throughcollectionofsalivausingthemethod describedbyRotteveletal.15andconcludedthattherewere
nodifferencesbetweensalivaryflowratesinbothgroupsof patients.11
A proper swallowing reflex is essential for the swal-lowing of saliva. This complex, fundamental function is mediatedbyorofacialneuromuscularsystems,andinvolves aseriesofsequentialreflexes andcoordinatedmovements of the muscles of the mandible, lips, tongue, pharynx, larynx,andesophagus.12Severalstudieshaveshowna
pos-itive correlation between sialorrhea in children with CP and the following factors: difficulties in the formation of the food bolus,3,7 inefficient labial sealing, suction
disor-der,increasedfoodresidue,3,16difficultycontrollingthelips,
tongue, and mandible,3,8 reduced intraoral sensitivity,3,17
reducedfrequencyofspontaneousswallowing,18esophageal
phasedysphagia,3,7anddentalmalocclusion.3,19Significant
negativecorrelationshavebeen found betweensialorrhea and chewing capacity, as well as other swallowing skills in general.3 Other factors, all common in CP, influence
thepresenceandseverityof sialorrhea:openmouth posi-tion, inadequate body posture, particularly of the head, intellectual disabilities, emotional state, and degree of concentration.1,12,20
Associationbetweensialorrheaand gastroesophagealrefluxdisease(GERD)
Salivaplaysanimportantroleinprotectingtheesophageal
mucosaagainstlesionscausedbyGERD.Inchildrenwith
sial-orrhea,theconstantlossofsalivacanimpairtheremovalof
gastricacidrefluxintotheesophagus,whichcan
perpetu-ateesophagealdysmotilityandesophagitis.3,21Heineetal.,
inastudycarriedoutin1996,showedthatapproximately
one-thirdofthe24childrenwithsialorrheahadevidenceof GERDinthe24-hourpHmonitoringoresophagoscopy.Inthis study,drugtreatmentwithcisaprideandranitidineforGERD didnotreduce theseverityandfrequencyofsialorrheain mostchildren,andintheauthors’opinion,salivasecretion stimulatedbyGERDshouldhaveclinicalsignificanceonlyin thosepatientswithsignificantesophagitis.21
ForErasmusetal.,chemicalirritation causedby GERD can lead to increased production of saliva through the mediationoftheparasympatheticnervoussystemand vago-vagal reflex, aiming to protect the oropharyngeal and esophageal mucosa. In children with oral motor dysfunc-tion, this increase in saliva production could accumulate in the pharynx and/or esophagus, increasing the risk of aspiration.In the authors’ opinion, it is still a matter of debatewhetherGERDalonecancauseseveresialorrheaand ifGERDtreatmentcanreduceitsintensityinchildrenwith CP.10
Classificationandclinical,social,andfamily implications
Fromaclinicalpointofview,sialorrheacanbeclassifiedas
anteriorandposterior;bothcanoccurseparatelyor
simulta-neously.Anteriorsialorrheaistheunintentionallossofsaliva
fromthemouth.Posteriorsialorrheaistheflowingofsaliva
fromthetonguetothepharynx.1,10,22
Anterior sialorrhea can lead topsychosocial, physical, andeducational consequences.One of them is social iso-lation, which can have negative effects on self-esteem. Themostseverelyaffectedchildrenmayhavean unpleas-antodor,andmayberejectedbytheirpeersandevenby their caregivers. Individuals may be perceived negatively and their intellectual capacity may be underestimated. The extent of this impact varies according to sociocul-turalcharacteristics,dependingonageandcognitiveability. Severe anterior sialorrhea requires frequent changes of clothesandcandamagebooks,computers,andkeyboards, threateningessential educationandcommunication tools. There can also be perioral infections and damage to the dentition.1,3,10,23---28 These consequencesaffectthe livesof
patientsandalsohave an impactonthequalityof lifeof familiesand caregivers. A Dutch group demonstrated the considerabledemandsplacedoncaregiversintermsof work-load, such as having to frequently remind the individual toswallow saliva, clean the excess saliva on the mouth, chin, and other areas, and change and wash towels and clothes.27,28
Posteriorsialorrheaoccursinchildrenwithmoresevere pharyngealphasedysphagia.Thesechildrenareat riskfor saliva aspiration, which can cause recurrent pneumonia andmayevengoundiagnosedbeforesignificantlunginjury develops.10 Parketal.describedtwocasesinwhichsaliva
aspirationintothe tracheobronchial tree wassuccessfully documentedthrough a radionuclide assessment known as a salivagram. This same method was used and showed a total reduction in saliva aspiration after botulinum toxin was applied to patients’ salivary glands.29 Vijayasekaran
Spasticity GERD
GERD
GERD
Sleep disorder Sialorrhea
Scoliosis
Respiratory hypersecretion Infections
Malnutrition
CPD
Dysphagia
Dysphagia
Aspiration Upper
respiratory obstruction
Involuntary movements
Positioning during meals / Food consistency / Volume and velocity of feeding /
Utensils used during meals / Total meal time
Intestinal constipation
Hospitalizations
Risk of premature
death
Epilepsy and use of anticonvulsants
Neurodevelopment
Parent / child interaction
Quality of life
Family functionality
Figure1 Interactionbetween the clinicalaspects involvedinthehealth ofchildren withCP. GERD,gastroesophageal reflux
disease;CPD,chronicpulmonarydisease.
pneumonia.Thus,therapeuticinterventionscaneffectively
improverespiratoryhealthinthesepatients.30
Sialorrheaassessment
Clinicalassessment
The different clinical aspects involved in the health
sta-tusof children with CPcan influence the occurrenceand
severityofsialorrheaand,conversely,theirseveritycanbe
influencedbytheirpresence(Fig.1).Therefore,when
eval-uatingsialorrhea,theseseveralfactors(Table1)shouldbe activelyassessedbyhistory-takingandthroughobservation ofthechild.1
Methodsofsialorrheameasurement
Itisdifficulttomeasuresialorrhea.Thechildmustnot
real-izethat he/sheis being observed andshould beassessed
duringeverydaysituations.Nevertheless,itisnecessaryto
quantifythe frequencyand severityof sialorrhea,aswell
asits impact on the quality of life of children and their
caregivers. The severity and impactof sialorrhea can be
evaluatedthroughobjectiveorsubjectivemethods.31
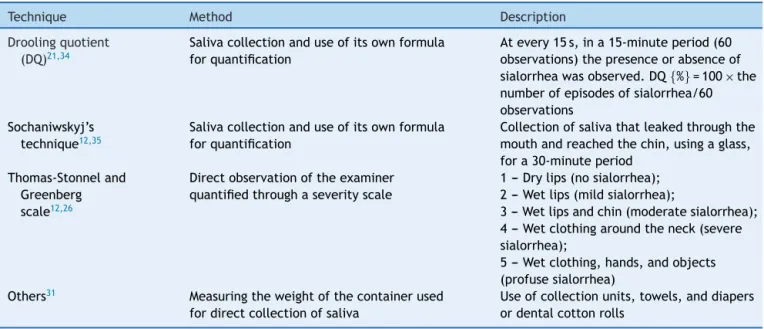
Objective methods include measurement of salivary flow and direct observation of saliva loss; some of these techniques are described in Table 2.12,21,25,26,31---35 The
development of direct (objective) measurement methods for anterior sialorrhea, which are validated and actually
feasible,arestillachallengebothintheresearchfieldand inclinicalpractice.31
Subjectivescalesareusefulandappropriatemethodsto measurechangesinsialorrhea,becausetheimpacton fam-ilies, caregivers,andthepatients themselvesis ofutmost importancewhenassessingsatisfactionwiththe effective-ness of any treatment. According to some researchers, the definitive method for evaluating the effectiveness of any treatment for sialorrhea is one that measures how much the life of the caregiver has been facilitated and that quantifies the improvement in the child’s quality of life.33,36SubjectivescalessuchastheDroolingRatingScale,
the Drooling Frequency and Severity Scale, visual analog scales,andtheDroolingImpactScale31,33,36arefilledoutby
patientsortheircaregivers,whichexpresstheirqualitative andquantitativeimpressionsoftheseverityandimpactof sialorrhea.31
Treatment
Objectives
The main objectives in the treatment of sialorrhea are:
reductioninsocial-affectiveandhealthimpactscausedby
anteriorsialorrhea;reductionin healthimpactscaused by
posterior sialorrhea;improved quality of life for patients
andcaregivers;andreductionintheburdenexperiencedby
Table1 Clinicalfactorstobeinvestigated.
Clinicalandsocial-emotionalhistory
Motivation,physical,andcognitiveabilitytotrytoreducesialorrhea
Useofmedications(anticonvulsants,benzodiazepines,neuroleptics)
Neurologicalexamination(includingstateofalertness,cranialnerves,overallmotorskills,posture,andtone)
Orofacialassessment(signsofupperairwayobstruction)
Oralhygiene,dentalocclusionandhealth,labialsealing
Language(dysarthria,dyspraxia)andcommunicationskillsingeneral
Cognition
Respiratoryhealth(hypersecretion,bronchospasm,andrecurrentinfections)/atopy
PresenceofGERD
Presenceandassessmentofdysphagia
Nutrition
GERD,gastroesophagealrefluxdisease.
Table2 Objectivemethodstomeasuresialorrhea.
Technique Method Description
Droolingquotient
(DQ)21,34
Salivacollectionanduseofitsownformula forquantification
Atevery15s,ina15-minuteperiod(60 observations)thepresenceorabsenceof sialorrheawasobserved.DQ{%}=100×the numberofepisodesofsialorrhea/60 observations
Sochaniwskyj’s technique12,35
Salivacollectionanduseofitsownformula forquantification
Collectionofsalivathatleakedthroughthe mouthandreachedthechin,usingaglass, fora30-minuteperiod
Thomas-Stonneland Greenberg scale12,26
Directobservationoftheexaminer quantifiedthroughaseverityscale
1--- Drylips(nosialorrhea); 2--- Wetlips(mildsialorrhea);
3---Wetlipsandchin(moderatesialorrhea); 4--- Wetclothingaroundtheneck(severe sialorrhea);
5--- Wetclothing,hands,andobjects (profusesialorrhea)
Others31 Measuringtheweightofthecontainerused
fordirectcollectionofsaliva
Useofcollectionunits,towels,anddiapers ordentalcottonrolls
Qualityoflifeandburdenonfamily/caregivers, self-esteem,andchild’shealth
Ingeneral,afterseveraltreatmentmodalities,thedemands
relatedtothecare ofthesechildren arereduced,
partic-ularly regarding the frequency of the need to clean the
mouth, lips, and chin; the number of changes of towels
and clothes; and damage tobooks, school supplies, toys,
and electronic equipment.36,37 Additionally, reduction in
sialorrhea improves social contact between children and theirpeers.Even in childrenwithintellectual disabilities, aGerman studyhasshown thattheperception ofparents concerningtheirchildren’ssatisfactionin relationtotheir physical appearanceandlife ingeneralcan improveafter therapeuticinterventions.36,38vanderBurgetal.published
astudy in whichtheyevaluatedchangesin qualityof life andnecessityofcareasaresultofsialorrheatreatment.The impactofsialorrheawasinvestigatedbeforeandafter treat-ment, using a questionnaire designed specifically for this study.Theresults demonstratedthatthedecreasein sali-varyflowhadasignificantlypositiveeffectontheneedfor dailycare.Theauthorsconcludethatreducedsalivaryflow shouldnotbetheonlygoalinthetreatmentofsialorrhea.It
isrecommendedthattheseveraltherapeuticmodalitiesbe assessedinrelationtotheimpacttheybringtothepatient’s dailylife.38
Therapeuticmodalities
Theliteraturedescribesseveralformsoftherapeutic
man-agement. The advantages and disadvantages of the main
treatmentmodalitiesaresummarizedinTable3.
Trainingofsensoryawarenessandoralmotorskills
Forchildren capableof obeying commandsand
cooperat-ingwiththetraining,thisisthefoundationofintervention
andshouldbetestedbeforeothertreatmentoptions.Initial
maneuversincludeimprovementsinthesittingposition,lip
movements,andclosingofthemandibleandtongue.Inits
simplestform,itconsistsofexercisesthatarecarriedout
ina playful manner, suchastheuse of differenttextures
aroundthemouth(icecubes,electrictoothbrush,etc.)to
stimulatesensory awareness and exercises toimprove lip
sealingandtonguemovement(usingastraw,lipstickkisses
Table3 Advantagesanddisadvantagesofthemaintherapeuticmodalities.
Therapeutic modalities
Advantages Disadvantages
Trainingofsensory
awarenessand
oralmotorskills
Treatstheunderlyingcause;
Long-lastingeffect
Dependsontheintellectualcapacity;
Requiresaccesstoregulartherapyandatrained
professional
Botulinumtoxin
use
Highefficacy;
Safe
Transienteffect;
Requiresequipmentandtrainedmultidisciplinary
staff;
Requiresgoodclinicalconditionforsedationor
anesthesia;
Doesnottreattheunderlyingcause
Surgicaltreatment Definitiveefficacy Definitivesideeffects;
Requiresgeneralanesthesia;
Demandsequipmentandtrainedsurgicalteam;
Doesnottreattheunderlyingcause.
Pharmacological
treatmentwith
anticholinergics
Proveneffectiveness;
Self-administered(bythepatientor
caregiver);
Doesnotrequiresedationoranesthesia;
Transientsideeffects
Frequentlyanticholinergiceffects(vomiting,
diarrhea,irritability,changesinmoodandinsomnia);
Doesnottreattheunderlyingcause.
of thespeech therapist is necessary.Unlike children with
more severe neurological symptoms and less capacity for
cooperationandunderstanding,thosewithmild sialorrhea
canachievesignificantbenefitsthroughsuchaprogram.39
Bodymodificationthroughbiofeedback
Bodymodificationthroughbiofeedbackisbasedonthe
mon-itoringof the target muscle group for electromyographic
stimulation.Whenthemusclecontracts,electromyography
informsof the change inmuscle activity throughacoustic
orlightsignals.Thus,thepatientcanconsciouslycorrector
improvecertaincomponentsofswallowing.Thetechnique
canhaveapositiveimpactonpatienttrainingandimproving
oromotorfunction.12,20
Orthodontictherapy
Itshouldbeusedascomplementarytoanyothertreatment,
andaimstopreventor correct an anterioropen biteand
otherverticalocclusionabnormalities.12
Pharmacologicalandsurgicaltherapies
Despite indications that hypersalivation is not one of the
factorsresponsibleforsialorrheainchildrenwithCP,most
availabletreatments---includingtheuseoforal(OR),
trans-dermal (TD), and sublingual (SL) medications, botulinum
toxin, or surgical management --- aim at the reduction in
salivaproduction.3
There areadvantages and disadvantages tothe use of thesetechniques(Table3)whencomparedwith nonpharma-cologicalandnonsurgicaltreatments.Ingeneral,theoptions aimed at reducing salivary production quickly lead to an effectivereductioninsialorrhea,butwithaprofileofside effectsinherenttoeachtreatmentmodality.Another impor-tantaspectisrelatedtothepossibleexacerbationofGERD andesophagitis.3Therefore,inthosepatientsundergoinga
treatmentwhosemechanismofactionistoreducesalivary production, early and effective GERD treatment becomes
essential. In this group of treatments, each type has its peculiarities,asdescribedbelow.
Botulinumtoxin
Theintraglandularinjectionofbotulinumtoxininhibitsthe
releaseof acetylcholinefromcholinergicnerveterminals,
thereby reducing salivary secretion and sialorrhea. Some
prospective,controlledstudieshaveinvestigatedtheuseof
botulinumtoxintypeA(BoNTA)forthetreatmentof
sialor-rhea.Asignificant reductioninsialorrheawasobserved in
thesestudiesusingobjective(ClassI)andsubjectivecontrol
scales.Theinjectionsitesaretheparotidandsubmandibular
glands.Olderchildren(cooperative)andadultsmayundergo
localanesthesia.1,40,41Somedisadvantages(Table3)hinder
patients’accesstotheprocedure:theinjectionsitesshould beaccessed,ideally,byultrasound;thetechniquerequires thepresenceofmedicalandnursingstaffwithexperience; and it should beassessed whether the patientmeets the clinicalrequirementstoundergosedationoranesthesia.
Surgicaltreatment
Thefirstsurgicaltreatmentforsialorrheawasparotidductal
relocation,42followedbyfurtherremovalofsubmandibular
glands.43,44 Radicalproceduressuchasbilateraldivisionof
theparotidductswithremovalofthesubmandibularglands and neurectomies have been proposed, but with unpre-dictable results.43---48 Surgeries were carriedout mostly in
adults, and their efficacy wasquestionable, as symptoms recurredaftersometime.43,44In1974,Ekedahldescribedthe
rearrangementofductsfromthesubmandibularglandsinto the tonsilar fossa.49 The glands maintained their function
in
children
with
cerebral
palsy
555
Table4 Pharmacologicaltreatment.
Authorand
year
Drug Associated
pathology
Ages n Studydesign Results Sideeffects
Mieretal.56 Glycopyrrolate CPand
other neurological conditions
4---19years 39 DB,PC Glycopyrrolate
0.10mg/kg/doseis effectiveforthecontrol ofsialorrhea
Incidenceof20%ofSE, enoughtowithdrawthe drug
Zelleretal.55 Glycopyrrolate CPand
other neurological conditions
3---18years 137 Uncontrolled clinicaltrial
Satisfactoryresponsein 40.3%ofpatientsinthe 4thweekand52.3%in the24thweek,witha peakof56.7%inthe 16thweek
Intestinalconstipation (20.4%),vomiting (17.5%),diarrhea (17.5%),pyrexia(14.6%), xerostomia(10.9%), flushing(10.9%),nasal congestion(10.9%) Matoetal.50 Scopolamine
TD
CPand other neurological conditions
12---58years 30 Prospective, randomized, DB,PC
Significantimprovement (p<0.005)inthe scopolaminegroup
Incidenceof23%ofSE (fourpatientswithmore severeSEandthreewith milderSE)
Camp-Bruno etal.51
Benztropine CP 4---44years
(14children/ adolescents and6adults)
20 DB,PC Significantreductionin sialorrheawhen comparedtoplacebo
Incidenceof11%ofmore severeSEresolvedin 24---48hafterdrug withdrawal Carranza-del
Rioetal.57
Trihexyphenidyl CP 1---18years 70 Retrospective Mostpatients(96%) reportedsome improvementin sialorrhea
SEwerefoundin69.3% ofpatients:intestinal constipation(43), urinaryretention(19), xerostomia(seven), blurredvision(five), increaseininvoluntary movements(four) reductioninseizure control(four), hallucinations(two) DeSimone
etal.70
Atropine sulfateSL
Upper digestive tractcancer
48---87years 22 Prospective, randomized, DB,PC
Thestudyfailedto demonstrate
effectivenessofatropine sulfatecomparedto placebo
Onlyonepatient (xerostomia)
has become the surgical technique of choice for severe
sialorrhea.44,49 Duetotheriskofpermanentconsequences
(especiallyxerostomia),itisindicatedonlyinseverecases, thosenon-responsivetonon-surgicaltherapiesandinwhich sialorrheahasgreatimpactonthehealthandqualityoflife ofthechildrenandfamilymembers/caregivers.1
Oral,transdermal,orsublingualdrugtreatment
Thesalivaryglands arecontrolledby theparasympathetic
autonomic nervous system and, therefore,
anticholin-ergic drugs induce a significant reduction in salivary
flow, being the most often used drugs. The
advan-tages and disadvantages of the oral (OR), transdermal
(TD), or sublingual (SL) use of anticholinergic drugs are
summarized in Table 3.12,50---57 The most widely used
sys-temicanticholinergicdrugsareglycopyrrolate,benztropine, scopolamine,atropine,andtrihexyphenidyl;however,only trihexyphenidylandatropinesulfateareavailableinBrazil; theresultsofsomestudieswiththesedrugsaresummarized inTable4.
Glycopyrrolate
Theoralsolutionofglycopyrrolateiscurrentlytheonly
for-mulationofananticholinergicdrugapprovedbytheUnited
States Food and Drug Administration (FDA) to treat
sial-orrhea in children aged3---16 years.Glycopyrrolate is not
availableinBrazil.
Scopolamine
Severalstudieshave shownareductioninsaliva secretion
withuseofscopolamine.Thetransdermalrouteeffectively
reducessalivarysecretioninapproximately67%ofpatients
anditsactioncanbedemonstrated15minafterthe
trans-dermal patch is applied.The main side effects are pupil
dilationandurinaryretention.53Lewisetal.observedthat
66%ofthepatientshadpupildilation,whichoccurredafew daysafterthestartofthetreatment.52
Benztropine
Therehasbeen onlyone studywithbenztropine involving
children.Thedrugwasconsideredeffectiveinacontrolled,
randomizedclinicaltrialpublishedbyCamp-Brunoetal.51
Trihexyphenidyl
In the largest study in children with trihexyphenidyl, a
drug commonly used in the treatment of extrapyramidal
syndromessuchasdystonia,theindicationsforusewere
dys-tonia(28.7%),sialorrhea(5.9%),anddystoniaandsialorrhea
(65.4%). The initial mean dose was 0.095mg/kg/day and
themaximummeandosewas0.55mg/kg/day,twotothree
timesaday. Sideeffectswerefoundin 69.3%ofpatients.
Mostpatientsreportedsomeimprovementindystonia,
sial-orrhea,andspecificlanguage.The authorsconcludedthat
trihexyphenidylwasbettertolerated in thispopulation of
childrenandadolescents(withCPandextrapyramidal
syn-drome)when comparedtotheadult population, andthat
improvementin sialorrhea may have occurred due tothe
anticholinergic effect of the drug, but also through
cen-tralaction, resultingin greater control motor of muscles
involved inswallowing.57 Otherstudies have reportedthe
successfuluseoftrihexyphenidylinadultstotreatsialorrhea inducedbyclozapine.58---60
Atropinesulfate
Althoughatropinehasbeenformanyyearsacknowledgedas
effective,ithasneverbeenwidelyacceptedforthe
treat-ment of chronic sialorrhea.54 The first mentionof its use
for treatment of sialorrhea was made in an article pub-lished inOctober1970bySmithetal.intheNewEngland JournalofMedicine.61 Subsequently,somestudiesreported
its use to treat drug-induced sialorrhea62---68 and patients
withParkinson’sdisease.69 DeSimone etal.publishedthe
only prospective, randomized, placebo-controlled, double blind studywithatropineSL,which failedtodemonstrate effectiveness ofatropinewhen comparedtoplacebo.70 In
2010, Rapoportreportedthecase of14-year oldboywith metachromatic leukodystrophy and excess oral secretions whoneeded frequent aspirations, which caused recurrent dropsinoxygensaturationcausedbysalivaaspiration, suc-cessfullytreatedwithatropinesulfateSL,representingthe onlyreportedcaseintheliteratureonatropinesulfateSLin childrenoradolescents.54
Therearenospecificstudies publishedinchildrenwith CP,butthereisongoingresearchusingatropineSL(0.5%eye drops)inchildrenwithCP,whichsuggestsgoodefficacywith lowincidenceofsideeffects.Suchdatawillbeavailablefor publicationsoon.
Final
considerations
In practice, to indicate any type of treatment for
sialor-rheainchildrenwithCP,oneshouldtake intoaccountthe
patient’saccesstotheproposedtreatment,aswellasthe
socioeconomicand culturalcharacteristics ofeach family,
in order for the individual choice of methods to be
effi-cient, more specific, and tobe lessof a burden for each
patient/family.The mosteffectivetreatment andtheone
that effectively addresses the causeof sialorrhea in
chil-drenwithCPistrainingofsensoryawarenessandoralmotor
skills, performed or supervisedby a trainedandqualified
speechtherapist.
Drugtherapies, suchastheuse ofbotulinumtoxin and
anticholinergics,haveatransienteffectandshouldideally
beadjuvanttospeechtherapy,orshouldbeconsidered in
specificcasesofpatientswithmoderatetoseveresialorrhea
or respiratory complications. Among the available drugs,
atropinesulfateisalow-cost,easy-accessdrugandappears
tohavegoodclinicalresponsewithgoodsafetyprofile.The
useoftrihexyphenidylforthetreatmentofsialorrheain
chil-drenmaybeconsideredfordyskineticformsofCPorinsome
selectedcases.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
2.BlascoPA.Surgicalmanagementofdrooling.DevMedChild Neu-rol.1992;34:368---9.
3.SennerJE,Logemann J,ZeckerS,Gaebler-SpiraD.Drooling, salivaproduction,and swallowingincerebralpalsy.DevMed ChildNeurol.2004;46:801---6.
4.Colver A, Fairhurst C, Pharoah PO. Cerebral palsy. Lancet. 2014;383:1240---9.
5.RosenbaumP,PanethN,LevitonA,GoldsteinM,BaxM,Damiano D,etal.Areport:thedefinitionandclassificationofcerebral palsy.DevMedChildNeurol.2007;109:8---14.
6.LeeRW,PorettiA,CohenJS,LeveyE,GwynnH,JohnstonMV, etal.Adiagnosticapproachforcerebralpalsyinthegenomic era.NeuromolecularMed.2014;6:821---44.
7.EkedahlC,ManssonI,SandbergN.Swallowingdysfunctioninthe braindamagedwithdrooling.ActaOtolaryngol.1974;78:141---9. 8.VanDeHeyningP,MarquetJ,CretenW.Droolinginchildrenwith cerebralpalsy.ActaOtorhinolaryngolBelg.1980;34:691---705. 9.TahmassebiJF,CurzonME. Thecause ofdroolinginchildren
withcerebralpalsy---hypersalivationorswallowingdefect?Int JPediatrDent.2003;13:106---11.
10.ErasmusCE,vanHulstK,RotteveelJJ,WillemsenMA,Jongerius PH.Clinicalpractice:swallowingproblemsincerebralpalsy.Eur JPediatr.2012;171:409---14.
11.ErasmusCE,VanHulstK,RotteveelLJ,JongeruisPH,VanDen HoogenFJ,RoeleveldN,etal.Droolingincerebralpalsy: hyper-salivationordysfunctionaloralmotorcontrol?DevMedChild Neurol.2009;51:454---9.
12.Silvestre-RangilJ, SilvestreFJ, Puente-SandovalA, Requeni-Bernal J, Simó-Ruiz JM.Clinical-therapeutic management of drooling:reviewand update. MedOralPatolOralCir Bucal. 2011;16:e763---6.
13.Reid SM, McCutcheon J, Reddihough DS, Johnson H. Preva-lenceand predictorsofdroolingin7-to14-year-oldchildren withcerebralpalsy:apopulationstudy.DevMedChildNeurol. 2012;54:1032---6.
14.KohlerPF,WinterME.Aquantitativetestforxerostomia. Arthri-tisRheum.1985;28:1128---32.
15.RotteveelLJ,JongeriusPH,vanLimbeek J,VanDen Hoogen FJ.Salivationinhealthyschoolchildren.IntJPediatr Otorhino-laryngol.2004;68:767---74.
16.LespargotA,LangevinM,MullerS,GuillemontS.Swallowing dis-turbancesassociatedwithdroolingincerebralpalsiedchildren. DevMedChildNeurol.1993;35:298---304.
17.Weiss-Lambrou R, Tetreault S, Dudley J. The relationship betweenoralsensationanddroolinginpersons withcerebral palsy.AmJOccupTher.1988;43:155---61.
18.SochaniwskyjA,KoheilR,BablichK,MilnerM,KennyDJ.Oral motorfunctioning,frequencyofswallowinganddroolingin nor-malchildrenandinchildrenwithcerebralpalsy.ArchPhysMed Rehabil.1986;67:866---74.
19.Franklin DL, Luther F, Curzon MEJ. The prevalence of mal-occlusion in children with cerebral palsy. Eur J Orthod. 1996;18:637---43.
20.MoralesChávezMC,NualartGrollmusZC,SilvestreDonatFJ. Clinicalprevalenceofdroolingininfantcerebralpalsy.MedOral PatolOralCirBucal.2008;13:e22---6.
21.HeineRG,Catto-SmithAG,ReddihoughDS.Effectofantireflux medicationonsalivarydroolinginchildrenwithcerebralpalsy. DevMedChildNeurol.1996;38:1030---6.
22.JongeriusPH,JoostenF,HoogenFJ,GabreelsFJ,RotteveelJJ. Thetreatmentofdroolingbyultrasound-guidedintraglandular injectionsofbotulinumtoxintypeAintothesalivaryglands. Laryngoscope.2003;113:107---11.
23.CottonRT,RichardsonMA.Theeffectofsubmandibular duct reroutinginthetreatmentofsialorrheainchildren.Otolaryngol HeadNeckSurg.1981;89:535---41.
24.HarrisS, Purdy A. Drooling and its management in cerebral palsy.DevMedChildNeurol.1987;29:805---14.
25.LewKM,YounisRT,LazarRH.Thecurrentmanagementof sial-orrhea.EarNoseThroat.1991;70:99---105.
26.Thomas-StonellN,Greenberg J.Threetreatmentapproaches and clinical factors inthe reduction of drooling. Dysphagia. 1988;3:73---8.
27.vanderBurgJ,JongeriusP,vanLimbeekJ,VanHukstA, Rot-tevelJ.Droolinginchildrenwithcerebralpalsy:aqualitative methodtoevaluateparentalperceptionsofitsimpactondaily life, social interaction, and self-esteem. Int J Rehabil Res. 2006;29:179---82.
28.ReidSM,JohnstoneBR,WestburyC,RawickiB,ReddihoughDS. Randomized trialofbotulinumtoxin injectionsinto the sali-vary glandsto reduce droolingin childrenwithneurological disorders.DevMedChildNeurol.2008;50:123---8.
29.ParkHW,LeeWY,ParkGY,KwonDR,LeeZI,ChoYW,etal. Saliva-gramafterglandinjectionofbotulinumneurotoxinAinpatients withcerebralinfarctionandcerebralpalsy.PMR.2012;4:312---6. 30.VijayasekaranS,UnalF,SchaffSA,JohnsonRF,RutttlerRJ. Sali-varyglandsurgeryforchronicpulmonaryaspirationinchildren. IntJPediatrOtorhinolaryngol.2007;71:119---23.
31.vanHulstK,LindeboomR,vanderBurgJ,JongeriusP. Accu-rateassessmentofdroolingseveritywiththe5-minutedrooling quotientinchildrenwithdevelopmentaldisabilities.DevMed ChildNeurol.2012;54:1121---6.
32.SuskindDL,TiltonA.Clinicalstudyofbotulinum-Atoxininthe treatmentofsialorrheainchildrenwithcerebralpalsy. Laryn-goscope.2002;112:73---81.
33.Jongerius PH, van Limbeek J, Rotteveel JJ. Assessment of salivaryflowrate:biologicvariationandmeasureerror. Laryn-goscope.2004;114:1801---4.
34.RaapD.Droolcontrol:long-termfollow-up.DevMedChild Neu-rol.1980;22:448---53.
35.SochaniwskyjAE.Droolquantification:noninvasivetechnique. ArchPhysMedRehabil.1982;63:605---7.
36.Reid SM, Johnson HM, Reddihough DS. The Drooling Impact Scale: a measure of the impact of drooling in children with developmental disabilities. Dev Med Child Neurol. 2010;52:e23---8.
37.FlussR,FaraggiD,ReiserB.EstimationoftheYoudenIndexand itsassociatedcutoffpoint.BiomJ.2005;47:458---72.
38.Vander BurgJJ,JongeriusPH,Van Hulst K,Van LimbeekJ, RottevelJJ.Droolinginchildrenwithcerebralpalsy:effectof salivaryflowreduction ondailylifeand care.DevMedChild Neurol.2006;48:103---7.
39.LittleSA,KubbaH,HussainSS.Anevidence-basedapproachto thechildwhodroolssaliva.ClinOtolaryngol.2009;34:236---9. 40.LakrajAA,MoghimiN,JabbariB.Sialorrhea:anatomy,
patho-physiology and treatment with emphasis on the role of botulinumtoxins.Toxins.2013;5:1010---31.
41.VashishtaR,NguyenSA,WhiteDR,GillespieMB.Botulinumtoxin for thetreatmentofsialorrhea:ameta-analysis.Otolaryngol HeadNeckSurg.2013;148:191---6.
42.WilkieTF.Theproblemofdroolingincerebralpalsy:asurgical approach.CanJSurg.1967;10:60---7.
43.WilkieTF,BrodyGS.Thesurgicaltreatmentofdrooling:aten yearreview.PlastReconstrSurg.1977;59:791---7.
44.Hornibrook J, Cochrane N. Contemporary surgical man-agement of severe sialorrhea in children. ISRN Pediatr. 2012;2012:364875.
45.Michel RG, Johnson KA, Patterson CN. Parasympathetic nerve section for control of sialorrhea. Arch Otolaryngol. 1977;103:94---7.
46.GlassLW,NobelGL,VecchioneTR.Treatmentofuncontrolled droolingbybilateralexcisionofsubmaxillaryglandsandparotid ductligations.PlasticReconstrSurg.1978;62:523---6.
48.DundasDF,PetersonRA.Surgicaltreatmentofdroolingby bilat-eralparotidductligationandsubmandibularglandresection. PlasticReconstrSurg.1979;64:47---51.
49.EkedahlC.Surgical treatmentofdrooling.Acta Otolaryngol. 1974;77:215---20.
50.MatoA,LimeresJ,TomasI,MunozM,AbuinC,FeijooJF,etal. Managementofdroolingindisabledpatientswithscopolamine patches.BrJClinPharmacol.2010;69:684---8.
51.Camp-Bruno JA, WinsbergBG,Green-Parsons AR, Abrams JP. Efficacy ofbenztropine therapy for drooling. DevMed Child Neurol.1989;31:309---19.
52.Lewis DW, Fontana C, Mehallick LK, Everett Y. Transder-malscopolamineforreductionofdroolingindevelopmentally delayedchildren.DevMedChildNeurol.1994;36:484---6. 53.MatoMonteroA,LimeresPosseJ,TomásCarmonaI,
Fernández-Feijoo J, Diz Dios P. Control of drooling using transdermal scopolamineskinpatches.Acasereport.MedOralPatolOral CirBucal.2008;13:e27---30.
54.RapoportA.Sublingualatropinedropsforthetreatmentof pedi-atricsialorrhea.JPainSymptomManag.2010;40:783---8. 55.ZellerRS,DavidsonJ,LeeHM,CavanaughPF.Safetyandefficacy
ofglycopyrrolateoralsolutionformanagement ofpathologic drooling in pediatric patients withcerebral palsy and other neurologicconditions.TherClinRiskManag.2012;8:25---32. 56.MierRJ,BachrachSJ,LajinRC,BarkerT, ChildsJ,MoranM.
Treatmentof sialorrhea withglycopyrrolate: a double-blind, dose-ranging study. Arch Pediatr Adolesc Med. 2000;154: 1214---8.
57.Carranza-delRioJ,CleggNJ,MooreA,DelgadoMR.Useof tri-hexyphenidylinchildrenwithcerebralpalsy.Pediatr Neurol. 2011;44:202---6.
58.SpivakB,AdlersbergS,RosenL,GonenN,MesterR,Weizman A.Trihexyphenidyltreatmentofclozapine-induced hypersaliva-tion.IntClinPsychopharmacol.1997;12:213---5.
59.AggarwalA,GargA,JilohaRC.Trihexyphenidyl(benzhexol)in clozapine-inducednocturnalenuresisandsialorrhea.IndianJ MedSci.2009;63:470---1.
60.Praharaj SK, Sarkhel S, Khanande RV, Sinha VK. Complete resolutionofclazapine-induced sialorrheawithlow dose tri-hexyphenidyl.PsychopharmacolBull.2010;43:73---5.
61.SmithRA,GoodeRL.Currentconcepts:sialorrhea.NEnglJMed. 1970;283:917---8.
62.AntonelloC,TessierP.Clozapineandsialorrhea:anew interven-tionforthisbothersomeandpotentiallydangeroussideeffect. JPsychiatryNeurosci.1999;24:250.
63.Comley C, Galletly C, Ash D. Use of atropine eye drops forclozapine inducedhypersalivation.AustNZJPsychiatry. 2000;34:1033---4.
64.TessierP,AntonelloC.Clozapineandsialorrhea:update.J Psy-chiatryNeurosci.2001;26:253.
65.FischerRB.Whattodoinneuroleptic-inducedsialorrhea. Psyc-hiatrPrax.2001;28:249---50.
66.FreudenreichO.Drug-inducedsialorrhea.Drugs Today(Barc). 2005;41:411---8.
67.Sockalingam S, Shammi C, Remington G. Clozapine-induced hypersalivation:areviewoftreatmentstrategies.CanJ Psy-chiatry.2007;52:377---84.
68.MustafaFA,KhanA,BurkeJ,CoxM,SherifS.Sublingualatropine forthetreatmentofsevereandhyoscine-resistant clozapine-induced sialorrhea. Afr J Psychiatry (Johannesbg). 2013;16: 242.
69.HysonHC,Johnson AM,Jog MS.Sublingualatropinefor sial-orrheasecondarytoparkinsonism: apilotstudy.MovDisord. 2002;17:1318---20.