Validation of Missouri Aneroid Sphygmomanometer to Measure
Blood Pressure in Patients with Cancer
Karine Azevedo São Leão Ferreira
1,2, Ana Claúdia dos Santos
1, Thais Cardoso Arthur
1, Daniela Aparecida A. dos
Santos
1, Daniela Pereira
1, Elizângela Oliveira Freitas
1, Fernanda Medeiros Fukuda
1, Wânia Regina Mollo Baia
1 Instituto do Câncer do Estado de São Paulo (ICESP) da Faculdade de Medicina da Universidade de São Paulo1, São Paulo, SP; UniversidadeGuarulhos (UnG)2, Guarulhos, SP - Brazil
Mailing address: Karine Azevedo São Leão Ferreira •
Rua Aníbal Borbola, 105, Parque dos Príncipes - 05396-265 - São Paulo, SP - Brazil
E-mail: [email protected], [email protected] Manuscript received June 12, 2009; revised manuscript received December 28, 2009; accepted March 18, 2010.
Abstract
Background: Auscultatory mercury sphygmomanometers to measure blood pressure (BP) have been banned from health services because of risk of pollution and environmental accidents with mercury. Aneroid appliances could be an alternative.
Objective: To validate the Missouri™ aneroid device for blood pressure measurement in cancer patients according to the protocol of the European Society of Hypertension (ESH).
Methods: 33 patients hospitalized or under outpatient care at the Cancer Institute of the State of São Paulo, FMUSP, were
evaluated. Three trained and blinded observers performed nine sequential blood pressure measurements interspersed with the mercury sphygmomanometers. The differences between the values of systolic blood pressure (SBP) and diastolic blood pressure (DBP) of the test device with the mercury sphygmomanometer were classified according to the ESH protocol.
Results: The Missouri™ equipment underwent all three phases required by the ESH Protocol for SBP and DBP, and it was approved in all of the phases. The average difference between the test device and the mercury sphygmomanometer was 0.62 (SD = 4.53) and 0.06 (SD = 6.57) mmHg for SBP and DBP, respectively. No association was found between the differences in BP measurements with sex, age, body mass index and arm circumference and length.
Conclusion: The results revealed that the aneroid Missouri™ device meets ESH accuracy recommendations for the measurement of SBP and DBP, and it can be used to replace the mercury sphygmomanometer. (Arq Bras Cardiol 2010;
95(2): 244-250)
Key words: Sphygmomanometers; hypertension; blood pressure; neoplasms; patients.
women with breast cancer8-10.
BP can be measured by a direct method (invasive) and by inserting a catheter into the artery connected to a transducer or by an indirect method using auscultatory and oscillometric techniques. The consistency and accuracy of various indirect measurement devices against invasive measurement may vary11.
Before being marketed, BP measurement devices should be tested according to the protocols proposed by the British Hypertension Society (BHS)12,13, or by the Association for the
Advancement of Medical Instrumentation (AAIM)14 or by the
European Society of Hypertension (ESH)15. This procedure
is called validation, and ensures greater reliability to the equipment. Although the models are manufactured in series and tested by the manufacturer, yet it is recommended that the validation is also performed14.
The accuracy and consistency of the various devices are controversial. Among sphygmomanometers, the mercury sphygmomanometer is considered the most accurate one and it is adopted as the gold standard for an indirect BP measurement1. However, due to the risk of environmental
Introduction
The blood pressure measurement (BP) is still important in clinical practice. It is a fundamental tool for early identification of cardiovascular and renal disease1.
The use of several chemotherapeutic and biological agents such as antiangiogenic antibodies, tyrosine kinase inhibitors and others, is associated with chronic and acute adverse cardiovascular events such as hypotension and hypertension in patients with breast, renal and colorectal cancer2-7. These
events are especially identified by measurement of BP. It is critical for early diagnosis and treatment.
accidents and mercury toxicity in case of equipment breakdown, its use has been banned in health services, making it necessary to identify reliable and validated instruments to replace them in these applications16. Hence, the purpose
of this study is to validate the Missouri™ aneroid device for measuring blood pressure in patients with cancer, according to the ESH protocol.
Method
The research was conducted at the Cancer Institute of the State of São Paulo (ICESP) with outpatients and inpatients in clinical and surgical units, after approval by the of Research Ethics Committee. We evaluated 39 patients, resulting in the study with 33 patients, who signed an informed consent, respecting the following inclusion criteria: patients older than 30, who could walk and had no heart diseases. Among the patients assessed, five patients were excluded for presenting some of the exclusion criteria: auscultatory gap, atrial fibrillation or arrhythmia; and one patient agreed to participate in the study but was excluded for not being clinically able due to intense pain.
We used a mercury sphygmomanometer as the gold standard, previously calibrated by the Institute for Technological Research (IPT) and certified by INMETRO for comparison with the Missouri™ aneroid auscultatory device. The resting blood pressure was measured after measuring the arm circumference with the arm extended to choose the appropriate cuff as recommended by the American Heart Association17. Before the measurement, patients remained
at rest for at least 15 minutes.
The device was validated as recommended by the ESH15.
Each patient underwent 14 sequential measurements in the same arm, with a time interval of 3 to 5 minutes between each, by three trained observers blinded as to the values measured by the others.
Observers 1 and 2 performed blood pressure (BP) measurements with the mercury sphygmomanometer interspersed with measurements with the test device, which was performed by observer 3. The total evaluation time for each patient averaged 40 minutes.
Sequence of measurements15
The sequence of blood pressure measurements was as recommended by the ESH15 and called BP, which stands for
blood pressure, as described below:
BPA (Blood Pressure A) = observers 1 and 2 perform independent measurements with the mercury sphygmomanometer. The average value was used to categorize the patients into three groups (Table 1).
BPB (Blood Pressure B) = 3 observers measured the BP with the test device. Such measurement was not included in equipment validity analyses used to determine patient’s BP characteristics and the equipment operation.
BP1 (Blood Pressure 1) = observers 1 and 2 with the mercury sphygmomanometer.
BP2 = observer 3 with the test device.
B P 3 = o b s e r v e r s 1 a n d 2 w i t h t h e m e r c u r y sphygmomanometer.
BP4 = observer 3 with the test device.
B P 5 = o b s e r v e r s 1 a n d 2 w i t h t h e m e r c u r y sphygmomanometer.
BP6 = observer 3 with the test device.
B P 7 = o b s e r v e r s 1 a n d 2 w i t h t h e m e r c u r y sphygmomanometer.
Measurements were performed in three phases (Phase 1, Phase 2.1 and Phase 2.2). The first phase included 15 patients, 5 of whom were in each of the three groups (Table 1), with a minimum of 5 men and 5 women. The second phase included 18 patients, totaling 33, who were equally distributed among the three groups, with a minimum of 10 men and 10 women.
Measurement of accuracy
To evaluate the accuracy of the test device, only those measures between BP1 and BP7 were used. The average values measured by observers 1 and 2 were calculated, corresponding to measures BP1, BP3, BP5 and BP7. Each measurement with the test device was interspersed with two measurements with the mercury sphygmomanometer. Thus, as recommended by the BHS protocol, the following differences were calculated for the DAP and PAS: BP2-BP1, BP2-BP3, BP4-BP3, BP4-BP5, BP6-BP5 and BP6-BP7. Out of these differences, three relating to DBP and three relating to SBP were selected, totaling 99 measurements. All of the three were selected considering: 1) if the values of the pairs were different, the smallest difference would be selected; and 2) if the values of the pairs were identical, the first of the two differences would be selected.
The values of the 99 differences between the two devices were classified into three cumulative zones: <5 mmHg, <10 mmHg and <15 mmHg.
Statistical analysis
Data were stored and analyzed using the program SPSS version 13.0, conducting descriptive analyses and inferences.
The continuous variables were assessed for their adherence to the normal distribution curve with the Kolmogorov-Smirnov test. All mean blood pressures and the differences between the pressure values measured with the test device and the mercury sphygmomanometer had a normal distribution. Thus, their values were compared using Student’s t test.
Pearson’s correlation test was used to assess the correlation between the mean values of DBP and SBP with the average differences between the test device and the mercury Table 1 -Pressure value ranges for classiication of patients into
groups15
Group Systolic pressure (mmHg) Diastolic pressure (mmHg)
Low 90 to 129 40 to 79
Average 130 to 160 80 to 100
sphygmomanometer.
Differences were considered statistically significant if p value was <0.05.
Results
Sociodemographic and clinical characteristics
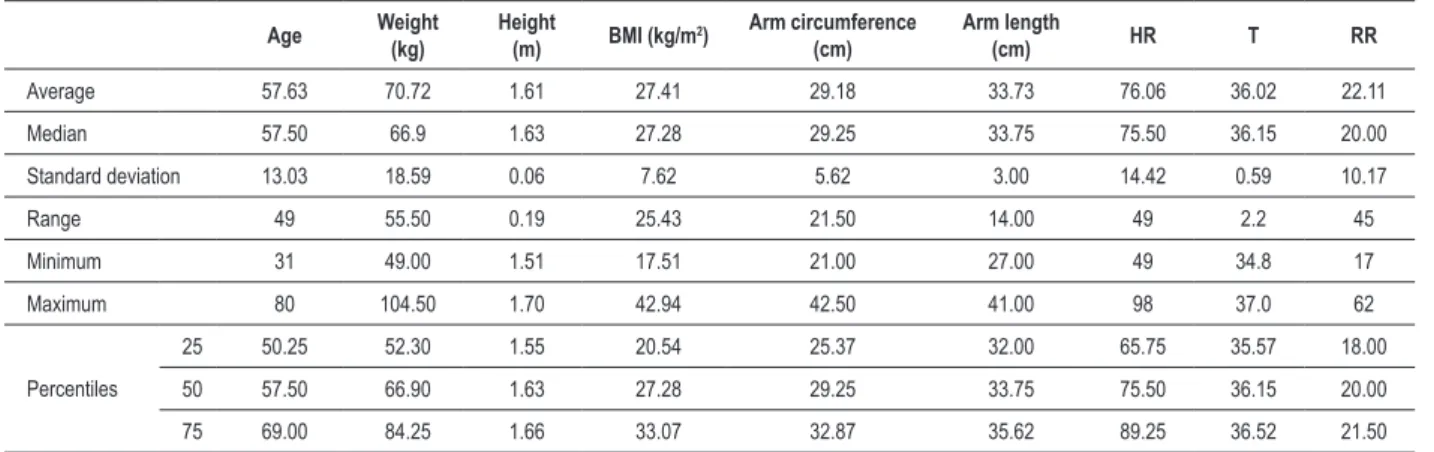
The final analysis included 33 patients, mostly female, married (45.5%), with predominance of white skin (54.5%) and average education level (60.6%) (Table 2). The mean age was 57.6 years old (Table 3).As for anthropometric measurements and vital signs, it was found that patients had breathing frequence, temperature and heart frequence values within normal limits, as shown in Table 3. Average BMI (Body Mass Index) was 27.41 kg/m2 and is compatible with
overweight. From the patients assessed, 21.2% were classified as normal (BMI ≤ 25), 15.2% as overweight (BMI = 26-30) and 15.2% were obese (BMI ≥ 31).
Measurements of arm circumference and length were also performed. Average values of 29.18 cm and 33.73 cm were also found, respectively (Table 3). From these data, we selected the appropriate cuff for the measurement.
By analysing the correlation between sociodemographic characteristics and average arterial pressure and the average differences for SBP and DBP, we found a statistically significant correlation only between age and average SBP of the mercury sphygmomanometer (r=0.35, p=0.05) and average SBP of the test device and mercury sphygmomanometer (r=- 0.38, p=0.033). Increased arm circumference were correlated with a significant increase in SBP measured by the test device (r=0.29, p=0.03) and the mercury sphygmomanometer (r=0.39, p=0.03) (Table 4).
No association was found between sex and the difference found between the systolic and diastolic pressure values of the test device and mercury sphygmomanometer. An association was found only between the average diastolic pressure values of the test device and the mercury sphygmomanometer. Men had mean diastolic blood pressures greater than those of women both with the test device (87.26 ± 16.07 vs 77.99 ± 9.41
Table 2 - Sociodemographic characteristics of patients
Classiication Frequence Percentage
Sex Female 18 54.5
Male 15 45.5
Skin color
White 18 54.5
Mestizo where white is
predominant 4 12.1 Mestizo where black is
predominant 7 21.2
Black 2 6.1
Eastern 1 3.0
Missing 1 3.0
Education level
Illiterate 4 12.1
Elementary/middle
education 4 12.1
High school 20 60.6
Higher education 4 12.1
Missing 1 3.0
Marital status
Single 4 12.1
Married 15 45.5
Cohabitation 1 3.0
Divorced 3 9.1
Widower 7 21.2
Missing 3 9.1
Table 3 - Anthropometric measurements and vital signs
Age Weight
(kg)
Height
(m) BMI (kg/m
2) Arm circumference
(cm)
Arm length
(cm) HR T RR
Average 57.63 70.72 1.61 27.41 29.18 33.73 76.06 36.02 22.11
Median 57.50 66.9 1.63 27.28 29.25 33.75 75.50 36.15 20.00
Standard deviation 13.03 18.59 0.06 7.62 5.62 3.00 14.42 0.59 10.17
Range 49 55.50 0.19 25.43 21.50 14.00 49 2.2 45
Minimum 31 49.00 1.51 17.51 21.00 27.00 49 34.8 17
Maximum 80 104.50 1.70 42.94 42.50 41.00 98 37.0 62
Percentiles
25 50.25 52.30 1.55 20.54 25.37 32.00 65.75 35.57 18.00
50 57.50 66.90 1.63 27.28 29.25 33.75 75.50 36.15 20.00
75 69.00 84.25 1.66 33.07 32.87 35.62 89.25 36.52 21.50
HR - heart rate; RR - respiratory rate and T - temperature in centigrade degrees.
mmHg, p=0.047) and with the mercury sphymomanometer (86.93 ± 14.84 vs 78.47 ± 8.65 mmHg, p=0.045).
Concerning the clinical characteristics, patients were almost equally distributed among breast (6.1%), prostate (3.0%), head and neck (9.1%), colorectal (6.1%), stomach (9.1%), hematologic (3.0%), lung (12.0%), ovary (3.0%) and testis (3.0%) tumors.
Table 4 - Correlation between blood pressure values and physical and demographic characteristics
Blood pressure Age Arm circumference (cm) Arm length (cm) BMI (kg/m
2)
r p value r p value r p value r p value
SBP test 0.26 0.14 0.39 0.03* -0.08 0.68 0.45 0.07
DBP test -0.12 0.50 0.33 0.08 -0.05 0.80 0.39 0.12
SBP mercury
sphygmomanometer 0.35 0.05* 0.39 0.03* -0.08 0.67 0.50 0.04* DBP mercury
sphygmomanometer 0.03 0.88 0.28 0.14 0.01 0.97 0.32 0.21
Average DBP test and mercury -0.32 0.08 0.27 0.15 -0.34 0.07 0.26 0.32
Average SBP test and mercury -0.38 0.03* 0.14 0.47 -0.11 0.56 -0.25 0.33
*statistically signiicant correlation.
9.1% (n = 3), circulatory diseases, 6.1% (n = 2) had diabetes mellitus, and 21.2% (n = 7) had some other comorbidity, such as bronchial asthma, coagulopathy, hypothyroidism, hypercholesterolemia, and glaucoma.
As for drugs used, it was found that opioid analgesic drugs were used by 36.4% (n=12); 39.4% (n=13) used non-opioid analgesic drugs; 33.3% (n=11), anti-inflammatory drugs; 15.2% (n=5), antibiotics; 9.1% (n=3) chemotherapy; 48.5% (n=16). gastroprotective drugs; 9.1% (n=3), diuretics; 3.0% (n=1), alpha blockers; 12.1% (n=4), beta blockers; 6.1% (n=2), calcium channel blockers; 12.1% (n=4), angiotensin-converting enzyme inhibitors; 6.1% (n=2), insulin; 27.3% (n=9), anticoagulants; and 27.3% (n=9) used antiemetics.
Validation of the device
We performed 462 pressure measurements. From these measurements, seven measurements of systolic and diastolic
pressure (BP1 to BP7) performed in 33 patients we included in the validation analysis. From these measurements, we obtained three differences totaling a set of 99 measurements for systolic (SBP) and diastolic (DBP) pressure.
In phase 1, we evaluated 15 patients with averaging 58,80 years old (SD=10,34, min.=41 and max.= 76), of which 60% (n=9) were men and 40% (n=6) were women. This sample included 45 measures of SBP and DBP. The number of SBP and DBP measurements in zones <5, <10 and <15 mmHg was above the minimum values required by the ESH (Table 5).
The analyses of Phase 2 included 33 patients and found that the mean differences between the test device and the mercury sphygmomanometer were 0.62 (SD = 4.53) and 0.06 (SD = 6.57) mmHg for SBP and DBP, respectively (Table 5). The average values of the 99 measurements of SBP and DBP were 134.64 (SD = 20.27) and 82.20 (SD = 13.49) mmHg, respectively (Table 6).
Table 5 - Cumulative frequence of differences between the pressure values generated by the test device (Missouri™) and the mercury sphygmomanometer and mean and standard deviation of pressure values and the difference between the devices
Blood pressure Degree of recommendation
Number of differences between the test device and the mercury device (mmHg)
Difference between the averages generated by the test device and the mercury device (mmHg)
< 5 < 10 <15 Average SD Median Min Max
Phase 1
ESH * - 25 35 40 - - - -
-SBP Approved 41 45 45 -0.38 3.09 0.00 -6.17 4.67
DBP Approved 43 43 44 -0.30 3.62 -0.33 -8.83 7.83
Phase 2.1
ESH* - 60 75 90 - - - -
-SBP Approved 84 93 93 0.62 4.53 0.0 -6.17 21.67
DBP Approved 91 91 92 0.06 6.57 -0.5 -8.83 32.67
Phase 2.2 2/3 < 5mmHg 0/3< 5mmHg
ESH* - 22 3
SBP Approved 30 1
DBP Approved 32 1
Table 6 - Comparison of blood pressure values (mmHg) generated by the test device (Missouri™) and the mercury sphygmomanometer
Blood pressure Test device
Mercury
sphygmomanometer p value Blood pressure BPA
Average SD Average SD Average SD Amplitude (range)
SBP 134.64 20.27 134.11 19.98 0.525 137.83 19.47 85
DBP 82.20 13.49 82.58 12.34 0.734 85.04 11.39 50
The number of measurements taken with the test device that differed from the mercury sphygmomanometer for 5, 10 and 15 mmHg or smaller is apresented in Table 5. Most of the differences were smaller than 5 mmHg (n = 84 and 91 for SBP and DBP, respectively).
As required by the ESH protocol in Phase 2.2, out of the 33 patients, at least 22 of them should have at least two of the three differences smaller than 5 mmHg. In this study, from the total sample, 30 met these criteria in SBP and 32 in DBP (Table 5).The second criterion required was that no more than three patients could have all three differences greater than 5 mmHg. In this study, only one patient in SBP and two in DBP obtained these measurements. Two patients in the SBP and DBP had one of the differences <5 mmHg (data not shown in tables). Figure 1 shows the correlation between the differences of values measured with the mercury device and the test device with the average values of systolic and diastolic blood pressures measured with both devices. Figure 1 shows that the points were concentrated between the difference interval of +5 to -5 mmHg, indicated on axis y, demonstrating the accuracy of the test device. The difference between the BP measurements of the mercury and test device were within the expected range, as well as the average values of systolic and diastolic pressure measurements.
By analysing the correlation between the average values of pressure measurements with the test device Missouri™ and the mercury sphygmomanometer, we found a strong correlation for SBP (r=0.972, p=0.00) and a moderate correlation for DBP (r=0.887, p=0.000).
The results described above and shown in TablE 5 are consistent with the requirements of ESH, indicating that the Missouri™ aneroid device fulfills the international validation criteria.
Discussion
The results found attest to the validity of the Missouri™ aneroid device for measuring blood pressure in patients with cancer, since it was approved in all evaluation criteria required by the ESH validation protocol.
The validation was performed according to the recommendations to validate automated instruments. This approach was adopted because it is a reliable criterion and no specific criteria were identified for validation of aneroid equipment. Some other aneroid equipment, such as the G7 Heine Gamma and XXL-LF18, Welch Allyn Tycos 76719 and
Maxi Stabil 320 were also validated as recommended by the
protocols for digital equipment.
In Brazil, the accuracy of aneroid devices are assessed only by Inmetro, which does require validation in individuals. Inmetro’s analysis includes the assessment of the following: proof of zero point indication, leak proof, determination of maximum error of measurement, determination of hysteresis and air leakage analysis. Besides these tests, fatigue and durability assessments are also performed21. Such assessment
neither covers the validation of such equipment in humans nor the measurement of the accuracy compared to the gold standard for noninvasive measurements, which is the mercury sphygmomanometer. Hence, it is not possible to ensure its accuracy for identifying too low or too high pressure values, requiring the validation of aneroid equipment in individuals.
The equipment is usually validated with the general population, the results of which cannot be extrapolated to special groups. Therefore, in the present study we chose to validate the MissouriϪ equipment specifically for adult patients with cancer, which is the population assisted at the Cancer Institute.
The BP measurements made with aneroid devices and with digital oscillometric devices are subject to errors that may result in differences greater that 5 and even 10 mmHg when compared to measurements with the mercury sphygmomanometer. These errors may be due to decalibrated equipment, which may occur due to falls even time of use, interference of environmental factors, such as outside noise, interference of factors related to the observer, the patient, the technique itself, and could be due to inappropriate selection of cuff width1,22.
Portable aneroid sphygmomanometers may be more easily damaged for being more prone to falls. Hence, wall sphygmomanometers would be preferable to the portable ones. Devices with more than six years of manufacturing and use tend to provide lower accuracy23. Thus, regular
dynamic testing of calibration and validation as well as measurements performed at sites with low noise, using the appropriate cuff size, considering the arm circumference, and training of professionals are essential to ensure an accurate measurement24.
In this study, all preventive measures were adopted to reduce the chance of errors.
Various techniques of pressure measurement are subject to greater or smaller interference. Hence, the appropriate selection of technique and equipment is essential. Aneroid sphygmomanometers, when properly calibrated, provide an acceptable accuracy and can be a reliable alternative to the mercury sphygmomanometers25.
Figure 1 -Blood pressure consistency measures [y - average arterial pressure (mmHg) and x - test-mercury difference (mmHg)].
pollution, should be banned and replaced with aneroid or oscillometric auscultatory devices. Therefore, it is essential that these devices be tested against mercury sphygmomanometers
in order to prove these are reliable alternatives18.
References
1. Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, et al. Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Circulation. 2005; 111 (5): 697-716.
2. Bono P, Elfving H, Utriainen T, Osterlund P, Saarto T, Alanko T, et al. Hypertension and clinical benefit of bevacizumab in the treatment of advanced renal cell carcinoma. Ann Oncol. 2009; 20 (2): 393-4.
3. Yusuf SW, Razeghi P, Yeh ET. The diagnosis and management of cardiovascular disease in cancer patients. Curr Probl Cardiol. 2008; 33 (4): 163-96.
4. Sparano JA, Gray R, Giantonio B, O’Dwyer P, Comis RL. Evaluating antiangiogenesis agents in the clinic: the Eastern Cooperative Oncology Group Portfolio of Clinical Trials. Clin Cancer Res. 2004; 10 (4): 1206-11.
5. Yeh ET, Tong AT, Lenihan DJ, Yusuf SW, Swafford J, Champion C, et al. Cardiovascular complications of cancer therapy: diagnosis, pathogenesis, and management. Circulation. 2004; 109 (25): 3122-31.
6. Scartozzi M, Galizia E, Chiorrini S, Giampieri R, Berardi R, Pierantoni C, et al. Arterial hypertension correlates with clinical outcome in colorectal cancer patients treated with first-line bevacizumab. Ann Oncol. 2009; 20 (2): 227-30.
7. Chen MH. Cardiac dysfunction induced by novel targeted anticancer therapy: an emerging issue. Curr Cardiol Rep. 2009; 11(3): 167-74.
8. Hager C, Hager K, Grubb S. Pheochromocytoma: an easily overlooked cause of secondary hypertension. W V Med J. 2009; 105 (2): 10-2.
9. Cook LK. Pheochromocytoma. Am J Nurs. 2009; 109 (2): 50-3.
10. Braithwaite D, Tammemagi CM, Moore DH, Ozanne EM, Hiatt RA, Belkora J, et al. Hypertension is an independent predictor of survival disparity between African-American and white breast cancer patients. Int J Cancer. 2009; 124 (5): 1213-9.
11. O’Brien E, De Gaudemaris R, Bobrie G, Agabiti Rosei E, Vaisse B. Proceedings from a Consensus Conference on Self-Blood Pressure Measurement. Devices and validation. Blood Press Monit. 2000; 5 (2): 93-100.
12. O’Brien E, Petrie J, Littler W, de Swiet M, Padfield PL, O’Malley K, et al. The British Hypertension Society protocol for the evaluation of automated and semi-automated blood pressure measuring devices with special reference to ambulatory systems. J Hypertens. 1990; 8 (7): 607-19.
13. O’Brien E, Mee F, Atkins N, O’Malley K. Validation requirements for ambulatory blood pressure measuring systems. J Hypertens. 1991; 9 (8 Suppl): S13-5.
14. O’Brien E, Mee F, Atkins N, O’Malley K. The quest for better validation: a critical comparison of the AAMI and BHS validation protocols for ambulatory blood pressure measurement systems. Biomed Instrum Technol. 1992; 26 (5): 395-9.
15. O’Brien E, Pickering T, Asmar R, Myers M, Parati G, Staessen J, et al. Working Group on Blood Pressure Monitoring of the European Society of Hypertension International Protocol for validation of blood pressure measuring devices in adults. Blood Press Monit. 2002; 7 (1): 3-17.
16. O’Brien E. Replacing the mercury sphygmomanometer: requires clinicians to demand better automated devices. BMJ. 2000; 320 (7238): 815-6.
17. Perloff D, Grim C, Flack J, Frohlich ED, Hill M, McDonald M, et al. Human blood pressure determination by sphygmomanometry. Circulation. 1993; 88 (5 Pt 1): 2460-70.
18. Dorigatti F, Bonso E, Zanier A, Palatini P. Validation of Heine Gamma G7 (G5) and XXL-LF aneroid devices for blood pressure measurement. Blood Press Monit. 2007; 12 (1): 29-33.
19. Ma Y, Temprosa M, Fowler S, Prineas RJ, Montez MG, Brown-Friday J, et al. Evaluating the accuracy of an aneroid sphygmomanometer in a clinical trial setting. Am J Hypertens. 2009; 22 (3): 263-6.
20. Reinders A, Jones CR, Cuckson AC, Shennan AH. The Maxi Stabil 3: validation of an aneroid device according to a modified British Hypertension Society protocol. Blood Press Monit. 2003; 8 (2): 83-9.
21. Ministério do Desenvolvimento, Indústria e Comércio Exterior - MDIC. Instituto Nacional de Metrologia, Normalização e Qualidade Industrial - INMETRO. Portaria Inmetro nº 153, de 12 de agosto de 2005 [Acesso em 2009 dez 18]. Disponível em http://www.inmetro.gov.br/legislacao/rtac/pdf/ rtac000966.paf.
22. Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, et al. Recommendations for blood pressure measurement in humans and experimental animals: Part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension. 2005; 45 (1): 142-61.
23. Yarows SA, Qian K. Accuracy of aneroid sphygmomanometers in clinical usage: University of Michigan experience. Blood Press Monit. 2001; 6 (2): 101-6.
24. Waugh JJ, Gupta M, Rushbrook J, Halligan A, Shennan AH. Hidden errors of aneroid sphygmomanometers. Blood Press Monit. 2002; 7 (6): 309-12.
25. de Greeff A, Lorde I, Wilton A, Seed P, Coleman AJ, Shennan AH. Calibration accuracy of hospital-based non-invasive blood pressure measuring devices. J Hum Hypertens. 2010; 24 (1): 58-63.
sphygmomanometer, as it is accurate and valid for noninvasive measurements of blood pressure.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association


![Figure 1 - Blood pressure consistency measures [y - average arterial pressure (mmHg) and x - test-mercury difference (mmHg)].](https://thumb-eu.123doks.com/thumbv2/123dok_br/15562398.601338/6.892.130.824.122.983/figure-pressure-consistency-measures-average-arterial-pressure-difference.webp)
