Original Article
A STUDY TO DETERM INE THE ASSOCIATION OF BODY M ASS
INDEX W ITH PERFORM ANCE-BASED M EASURES OF BALANCE
AND M OBILITY IN YOUNG ADULTS
M adhuri Gaur* , Kunjal Parekh.
Jr. Lect urer, BITS Inst it ute of Physiot herapy, Varnama, Vadodara, Gujarat , India.
Background:The incidence of obesit y is increasing in younger adult s, w it h associat ed w orsening of disabilit y. Lit t le is know n about t he im pact of body m ass index (BM I) on perform ance-based balance and m obilit y m easures in younger adult s.
Objective:The purpose of t his st udy w as t o exam ine t he associat ion of BM I w it h m easur es of balance and m obilit y.
M et hods:Young adult s w ho part icipat ed in t he st udy (N=50) w ere classified as norm al w eight , overw eight , m oderat ely obese, or severely obese. M obilit y and balance w er e assessed by perform ance-based m easur es. Pearson correlat ion t est w as used t o exam ine t he associat ion am ong BM I, m obilit y, and balance aft er cont rolling for pot ent ial conf ounding variables.
Results:There is a significant corr elat ion bet w een m obilit y and BM I at 0.01 levels. There is also a significant cor relat ion bet w een balance and BM I, t hough t here w as no corr elat ion found bet w een st anding w it h nar row base balance and BM I.
Conclusions:Higher BM I levels are associat ed w it h poorer m obilit y and balance. Furt her m ore, individuals classified as being of nor m al w eight and t hose classified as overw eight w ere sim ilar in m obilit y and balance, w hereas individuals w it h obesit y had great er im pairm ent s in m obilit y and balance.
KEY W ORDS: Balance, M obi lit y, Body M ass Index (BM I), Weight , Obesit y, Im pairm ent .
ABSTRACT
INTRODUCTION
Address for correspondence: Dr. M adhuri Gaur, Jr. Lect urer, BITS Inst it ute of Physiot herapy, Varnama, Vadodara, Gujarat , India. E-M ail: [email protected]
DOI: ht t p:/ / dx.doi.org/10.16965/ ijpr.2015.163
Quick Response code
Access this Article online
International Journal of Physiotherapy and Research
ISSN 2321- 1822
w w w.ijm hr.org/ ijpr.htm l
DOI: 10.16965/ ijpr.2015.163
Received: 25-06-2015 Peer Review : 25-06-2015 Revised: None
Accept ed : 20-07-2015 Published (O): 11-08-2015 Published (P): 11-08-2015
Obesity is a major public healt h problem around t he w orld. There has been a subst antial increase in t he prevalence of obesit y globally, even in developing count ries [ 1]. The prevalence of obesit y is increasing rapidly in young adult s (18-22 yrs) and adult s (23-64 yrs). This increasing prevalence is of gr eat concern because t he health and economic burdens of obesity are vast. Numerous chronic diseases, including hypert e-nsion, cardiovascular disease, t ype 2 diabet es,
osteoart hrit is, and certain forms of cancer, are st rongly associat ed w it h excess body w eight [2,3].
i nst r um ent al act i vi t i es of d ail y li v in g an d mobilit y tasks. Impairments in physical funct ion, such as the component s of mobilit y and balance, have been linked to the development of disability. The 6-M inut e Walk Test has been used as a measure of mobilit y and aerobic endurance in older adult s w it h and w it hout disease and has show n t o be a reliable measure. The 6M WT is a pract ical sim ple t est t hat r equir es a 100-f t hallw ay but no exercise equipment or advanced t raining for t echnicians. Walking is an act ivit y perform ed daily by all but t he m ost severely im pair ed pat ient s. This t est m easur es t he dist ance t hat a pat ient can quickly w alk on a flat , hard surface in a period of 6 minut es. Single leg st ance m easur es st at ic st anding abilit y (balance w it h feet fixed). This t est helps t o assess st anding balance. Tandem st ance assesses st at ic balance w it h narrow base of support . For client s w ho cannot perform t he single leg st ance, use the TS t est for an out come measure.
The BM I is t he most common met hod t o quantify w eight across a range of body sizes in adult s. Using t he BM I, individuals can be classified as: Normal Weight : BM I 18.5 – 24.9
Overweight : BM I 25 – 29.9 Obese: BM I 30 – 34.9 M oderat e Obese: BM I 35 – 39.9 Severe Obese: BM I >40
The BM I is an inexpensive and easy-t o-use clinical measure t hat can be administ ered w it h minimal t raining [6]. Healt h care professionals, such as physical t herapist s, m ay ut ilize t his sim p l e m easu r e t o scr een pat i en t s an d det erm ine risks for diseases associat ed w it h obesit y.
St udies invest igat ing t he relat ionship bet w een BM I and mobilit y have focused on individuals w it h severe obesit y [7,8] and few st udies have exam ined t he relat ionship bet w een BM I and balance [9].
The purposes of this st udy w ere t o describe how mobilit y and balance measures are affect ed by BM I and t o examine ot her fact ors t hat might explain t he associ at i on bet w een BM I and mobilit y and balance.
M ATERIALS AND M ETHODS
having age betw een 18-24 years from t he Rajkot Cit y, India, and excluded t he subject s w it h Neuromuscular disorders, Cancer, M ajor surgery in t he previous 6 mont hs, Severe pulm onary disease, chest pain w it h act ivit y, A cardiac event such as a heart at t ack in t he previous 6 mont hs.
Present st udy conduct ed w it h 50 young adult s
Procedure:
BM I: Height and w eight w ere measured w hile w earing indoor clot hing and w it hout shoes. The BM I classificat ions used in t his st udy w ere based on t he Wor ld Healt h Organi zat io n’s definit ions of
Normal weight (BM I 18.5 t o <25 kg/ m2)
Overw eight (BM Ie” 25 t o <30 kg/ m2)
Class I obesit y (BM Ie” 30 t o<35 kg/ m2)
M obility measure: Six-M inute Walk Test , Each part icipant was asked t o walk as far as possible in 6 m inut es, t aking st anding rest periods as needed. A st raight pat h of 12.18 m w as used. The t otal distance walked back and fort h in 6 minut es w as recorded.
Balance measures: Timed balance measures, Par t i cip ant s w ere asked t o m ai nt ain t heir balance for up t o 30 seconds under each of t he follow ing condit ions: w it h eyes closed:
St anding w hile t he feet w ere positioned as close t oget her as possible
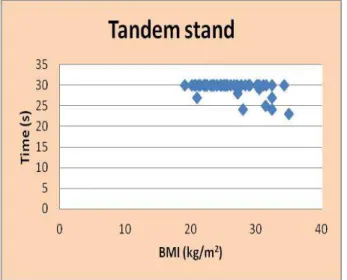
Tandem stand Single-leg st ance
Statistical Analysis: Dat a w as analyzed by using Pearson Correlat ion Test and interpreted w it h t he available lit erat ure.
RESULTS
Fig. 2: Show ing correlation betw een BM I and t he Balance (Tandem stand).
Fig.3: Showing correlat ion bet w een BM I and t he Balance (one leg st and).
DISCUSSION
BM I levels. Differences in st at ic balance among w eight groups m ay be clinical m eaningful. A great er number of individuals w it h moderat e o b esi t y w er e u nab l e t o co m p let e t h e p er f o r m an ce-b ased m easu r es o f b al an ce compared with t hose who were of normal weight and t h ose w ho w er e o ver w eigh t . Lack o f complet ion of balance measures in part icipant s w it h higher BM I w as relat ed t o inabilit y t o assume t he t est posit ions (eg, t andem st ance & single leg st ance). Thus, had all part icipant s w it h obesit y been able t o complet e t he balance measures, our result s may have differed. M any of t he impairment s t o w alking relat ed t o obesit y can be at t r ibut ed t o dif fer ences in t em po r o spat ial gai t p ar am et er s o bser v ed bet w een obese and normal w eight populations. When w alking at a self select ed pace, obese individuals w alk at a slow er velocity w it h shorter st ride length and spend more time wit h their feet cont act ing t he ground via longer double support t imes and st ance t imes [11]. Obese adult s also w alk at a slow er cadence wit h w ider step w idt hs and short er sw ing t imes [12].
Obesit y may also affect adapt at ion and mobilit y by limit ing an individual’s abilit y t o mot or plan, t he abilit y t o pre-plan a movement before t he movement is executed. Poor motor leads to poor perform ance on t asks [13]. This could be a det rim ent t o adapt at ion because adapt ive behavior involves t ailoring act ions t o variat ions in one’s environment . Therefore m ot or plans need t o be changed during mot or act ions [14]. In t he obese populat ion, poor mot or planning and an inabilit y t o adapt mot or plans during t he course of act ion could lead t o more frequent losses of balance or t he inabilit y t o recover from unavoidable losses of balance.
Obesit y is associat ed w it h increased burden of chronic disease and decreased physical act ivit y level, b ot h o f w h ich h av e been sh ow n t o negat ively affect mobilit y [10]. In t he current st udy, individuals w it h obesit y w ere less likely t o engage in physical act ivit y compared w it h t hose w ho were overweight and t hose of normal w eight . The associat ion bet w een BM I and m o bi li t y w as p ar t i all y expl ai ned by t hese fact ors. Using m ean speed of foot cent re of pressure (COP) t o approximate balance stabilit y, Hue et al. [15] estimated the contribution of body Ther e is a si gnif ican t cor r el at ion bet w een
mobilit y and BM I at 0.01 levels.
There is also a significant correlat ion bet w een b alan ce an d BM I t h o ugh t h er e w as n o significant correlat ion found bet w een st anding w it h narrow base balance and BM I.
When examining balance and mobilit y across w eight groups in younger adult s, t here w ere more
d if f er en ces i n m o bi l i t y t han in b al an ce. Individuals w ho w er e classif ied as being of n or m al w eigh t an d t h o se classif i ed as overweight w ere similar in mobilit y and balance, b ut i nd i v id u als w it h m o d er at e o b esi t y demonst rat ed consist ent ly low er performance t han t he ot her groups.
w eight to post ural st abilit y in condit ions of vision an d n o v i sio n . Th e st u d y n o t ed a st r o n g correlat ion bet w een increased body w eight and decreased post ural st abilit y, as evidenced by increased COP speed t o m aint ain st abi lit y, decr eased m ean p eak st ab il it y t i m es an d i ncr eased m ean di st an ce b et w een st abl e posit ions. These m easurement s suggest t hat o bese p er so n s ar e l ess r esp o n si v e t o pert urbat ion t han normal w eight subject s. One p ot en t i al exp lan at i o n f o r t h i s d ecr eased sensit ivit y is t he increase in mean pressure t hat t he mechanorecept ors – t he body ’s sensory recept ors for pressure – are under due t o an elevat ion in body w eight .
Exist ing evidence show s t hat pat ient s w it h obesit y adapt their gait in order t o accommodate excess w eight and t emporarily prot ect bones and joint s how ever by doing so put t hemselves at great er risk for damage t o t heir joint s and associat ed pain. In addit ion t o impairment s of t he musculoskeletal system t hose pat ient s w it h obesit y may also have cognit ive impairment s t hat could int erfere w it h m ot or planning and t herefore also cont ribute t o mobilit y disabilit y. The age of t he pat ient , dist ribut ion of body fat , and fact ors in t he environm ent in w hich t he person plans t o be physically act ive must also be considered.
W ei gh t l oss pr o gr am s sho u ld i ncl ud e t h e adopt ion of resist ance exercise and regular physical act ivit y. Individuals w it h obesit y w ere l ess l i kel y t o en gage in p hy si cal act i vi t y compared w it h those who w ere overw eight and t hose of norm al w eight . Young adult s w it h obesit y should be rout inely advised by t heir healt h care provider t o become more physically act ive for t he purpose of losing w eight and r educing car diovascular and m et abolic r isk profiles. Alt hough such advice is w ell int ended t o prom ot e healt h and w ellness, changes t o physical act ivit y levels and t he associat ed benefit s are illusive unless issues relat ed t o funct ional mobilit y are addressed.
Limitations of the study Includes:
CONCLUSION
Higher BM I levels are associat ed w it h poorer mobilit y and balance. Furt hermore, individuals classified as being of normal w eight and t hose classified as overw eight w ere similar in mobilit y and balance, w hereas individuals w it h obesit y had greater impairments in mobilit y and balance.
Conflicts of interest: None
REFERENCES
[1] . M endez M A, M ont eiro CA, Popkin BM . Overw eight exceed s u n der w ei gh t am o n g w om en i n m ost developing count ries. Am J Clin Nut r. 2005;81:714– 721.
[2]. Kopelm an PG. Obesity as a m edical problem . Nat ure. 2000;404:635–643.
[3]. Pi-Sunyer FX. M edical hazards of obesit y. Ann Intern M ed. 1993;119(7pt 2):655–660.
[4] . Han TS, Tijhuis M A, Lean M E, Seidell JC. Qualit y of l i f e i n r e l at i o n t o o v er w e i gh t an d b o d y f at dist ribut ion. Am J Public Healt h. 1998;88:1814– 1820.
[ 5] . Blaum CS, Xue QL, M ichelon E. The associat ion bet w een obesit y and t he frailt y syndr om e in older w om en: t he Wom en’s Healt h and Aging St udies. J Am Geriat r Soc. 2005;53:927–934.
[6]. Clinical guidelines on t he ident ification, evaluat ion, and t reat m ent of overw eight and obesit y in adult s: e xe cu t i v e su m m ar y; Exp e r t Pan e l o n t h e Id e n t i f i cat i o n , Eval u at i o n , an d Tr eat m en t o f Overw eight in Adult s. Am J Clin Nut r. 1998;68:899– 917.
[7]. Browning RC, Baker EA, Herron JA, Kram R. Effects of obesit y and sex on t he energetic cost and preferred speed of w alking. J Appl Physiol. 2006;100:390– 398.
[ 8]. De Souza SA, Faint uch J, Valezi AC, et al. Gait cinem at ic analysis in m or bidly obese pat ient s. Obes Sur g. 2005;15:1238–1242.
[9]. Corbeil P, Sim oneau M , Rancourt D, et al. Increased r i sk f o r f al l i n g asso ci at e d w i t h o b e si t y : m at hem at ical m odeling of post ural cont rol. IEEE Trans Neural Syst Rehabil Eng. 2001;9:126–136. [ 1 0] . LaCr o i x AZ, Gu r al n i k JM , Ber k m an LF, e t al .
M ai nt ain in g m o bi li t y in lat e li f e; II: sm o ki ng, alcohol consum pt ion, physical act ivit y, and body m ass index. Am J Epidem iol. 1993;137:858–869. [11]. Lai PP, Leung AK, Li AN et al. Three-dim ensional gait
analysis of obese adult s. Clinical Biom echanics 2008;23(Suppl.1):S2–S6.
[ 12] .Wear i ng SC, Hen ni g EM , Byr n e NM et al . Th e biom echanics of r est r ict ed m ovem ent in adult obesit y. Obesit y Review s 2006;7:13–24.
[ 13] . Wolp er t DM & M i all RC. For w ard m od el s f or ph ysi olo gical m o t or co nt r ol. Neur al Net w or ks 1996;9:1265–1279.
[14]. Adolph KE, Joh AS, Fr anchak JM et al. Flexibilit y in t he developm ent of act ion. In: The psychology of act i o n . N ew Yo r k : Oxf o r d Un i v e r si t y Pr ess, 2008;2:399–426.
[15]. Hue O, Sim oneau M , M arcott e J, Berrigan F, Doré J, M arceau P, Tremblay A, M arceau S, Teasdale N. Body w eight is a st rong predict or of post ural stabilit y. Gait Post ure 2007;26(1):32-38.