1. Rheumatologoly, Mackenzie Evangelical Hospital of Medicine, Curitiba, PR. Brazil
tional and metrology indexes, showing that patients with severe cumulative damage are more affected. Keywords: Spondyloarthritis; Balance; Falls.
INTRODUCTION
Spondyloarthritis (SpA) patients, mainly those with ad-vanced disease, may have postural difficulties1. In these
patients the spine may became stiff due to the chronic inflammatory process of fibroconnective tissues and bones, leading to hip flexion, increase in dorsal kypho-sis and loss of lumbar and cervical lordokypho-sis. Knee flex-ion occurs as a compensatory mechanism promoting the appearance of the classic skier posture. Such malalignment causes dislocation of the center of mass of the trunk, disturbing static and dynamic balance2. It
also causes difficulties in looking up and creating visu-al inputs that are important to compensate the negative effects of postural instability3. Balance in SpA may be
further conditioned by impairment of sensory path-ways, vestibular dysfunction and by inflammation of tendons4-6. According to Demontis et al.4, stimulation of
muscle and tendons by the inflammatory process may alter the sensitivity of muscle spindles leading to decrease in proprioceptive perceptiveness and contribu -ting to the problem.
Balance impairment is a frequent and underdiag-nosed manifestation in SpA that may contribute to the loss of life’s quality4. These patients may also have
co-morbidities such as osteoporosis7. The combination of
postural instability increasing the chance of falls8and
osteoporosis7, heightens the risk of fractures further
ag-gravating the deterioration of life’s quality. In terms of morbidity and mortality, injurious falls have serious consequences of which the hip fracture is the most feared one9. SpA patients, when falling, may harm
themselves more easily than normal individuals be-cause their spine is inflexible, disturbing the capacity
Balance and falls in axial spondyloarthritis:
a cross-sectional study
Mewes KB1, Longo B1, Campos APB1, Simioni J1, Skare TL1
ACTA REUMATOL PORT. 2019;44:248-253
ABSTRACT
Background: Spondyloarthritis (SpA) patients may suf-fer from balance loss predisposing them to falls. We aim to study balance impairment and falls in axial SpA patients and its association with clinical and epi-demiological variables, disease activity, functional and metrology indexes.
Methods: Cross-sectional study of 55 SpA patients with axial disease. Clinical and epidemiological data were collected from the charts. Balance was accessed by Berg Balance Scale (BBS). The following instruments were applied: ASDAS (Ankylosing Spondylitis Disease Activity Score)-ESR, ASDAS-CRP, BASDAI (Bath Anky-losing Spondylitis Disease Activity Index), BASFI (Bath Ankylosing Spondylitis Functional Index), BASMI (Bath Ankylosing Spondylitis Metrology Index) and ASQoL (Ankylosing spondylitis quality of life ques-tionnaire). The number of falls in the last year was ob-tained through direct questioning.
Results: In this sample, 30.9% had high risk of falls by the BBS and 25.4% recalled having at least one fall in the last years. The BBS values were lower in those with white ethnic background (p=0.01), smokers (p=0.03) and with HLA-B27 (p=0.03) and correlated inversely with BASDAI (rho=-0.28), ASDAS-ESR (rho=-0.32) and ASDAS-CRP (rho=-0.33), BASFI (rho=-0.71,p<0.0001), BASMI (rho=-0.80; p<0.0001), ASQoL (rho=-0.57; p<0.001) and age (rho=-0.50;p<0.001). Linear multi-variable analysis showed that BASFI and BASMI were in-dependently associated with BBS (p=0.01 and <0.0001 respectively). Patients with falls had lower BBS (p=0.03) and loss of balance correlated with impairment of the quality of life (rho=-0.56; p<0.001).
Conclusions: Balance is impaired in 1/3 of axial SpA patients and the BBS is associated mainly with
func-to protect themselves after sudden changes of posi-tion10. However, Aydog et al10studying 75 patients
with ankylosing spondylitis failed to prove that these patients have more balance disorders when compared to controls10.
In this study we aimed to analyze the presence of balance impairment in axial SpA patients and to veri-fy the influence of epidemiological and clinical factors that are associated with its appearance.
METHODS
This was a cross-sectional study approved by the local Committee of Ethics in Research. All participants signed consent. It included a convenience sample of 55 axial SpA patients that came for regular consulta-tions in a single center, for the period of one year and that agreed to participate in the study. To be included patients had to fulfill the classification criteria for axi-al SpA according to Assessment of Spondyloarthritis International Society (ASAS)11.
Epidemiological (gender, age, disease duration, eth-nic background, smoking habits, work status), clieth-nical (peripheral arthritis, dactilitis, enthesitis, ocular in-volvement, presence of HLA-B27), and treatment data was obtained through chart review. Clinical data were considered in a cumulative way. Information on im-age [presence of sacroiliitis unilateral or bilateral judged by magnetic resonance imaging (MRI)] was provided by the attending rheumatologist and fol-lowed the definition of ASAS/Omeract MRI group12.
The number of falls in the last year was obtained through the question: “How many falls did you have in last year?”
Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)13, Ankylosing Spondylitis Disease Activity
Score) -ESR (erythrocyte sedimentation rate)14and
AS-DAS-CRP (C reactive protein)14, Bath Ankylosing
Spondylitis Functional Index (BASFI)15, and Bath
Anky-losing Spondylitis Metrology Index (BASMI)16;
Anky-losing spondylitis quality of life questionnaire (ASQoL)16
were obtained. Simultaneously the Berg Balance scale (BBS)17was applied. The BBS has 14 tasks that assesses
the patient’s ability to either keep balance statically, or while performing movements for a specified duration of time. Each item scores from 0 to 4, with a maximum global score of 56 points. Values ≤ 45 indicate that in-dividuals may be at greater risk of falling and score of < 40 are associated with almost 100% fall risk18.
Data was collected in frequency and contingency tables. The Shapiro-Wilk test was used to study data distribution. BBS values were studied as a continuous variable. To compare BBS values according to clinical, epidemiological, image and treatment variables, the Mann Whitney test was applied. Correlation studies were done by Spearman test. The adopted significance was of 5%. A linear multiple regression was performed in a backward stepwise using BBS values as a contin-uous dependent variable to investigate the best subset of variables in which the best fit in the model. The soft-ware Medcalc 10.0 was used to perform calculations.
RESULTS
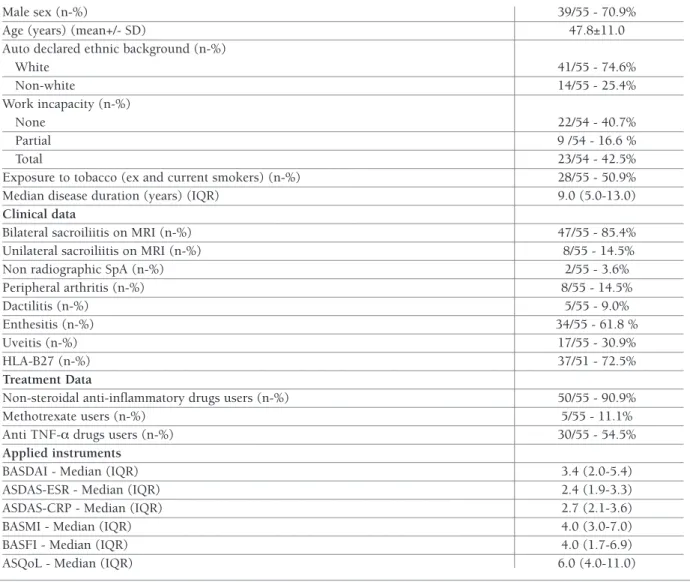
The main characteristics of the studied sample is on Table I.
In this sample, the BBS ranged from 35.0 to 56.0 (median of 51.0 with IQR= 44.0-55.0). In 38/55 (69.0%) the BBS values were >45 and in 17/55 (30.9%) were ≤ 45. About 25.4% (14/55) patients re-membered having at least one fall in the last year.
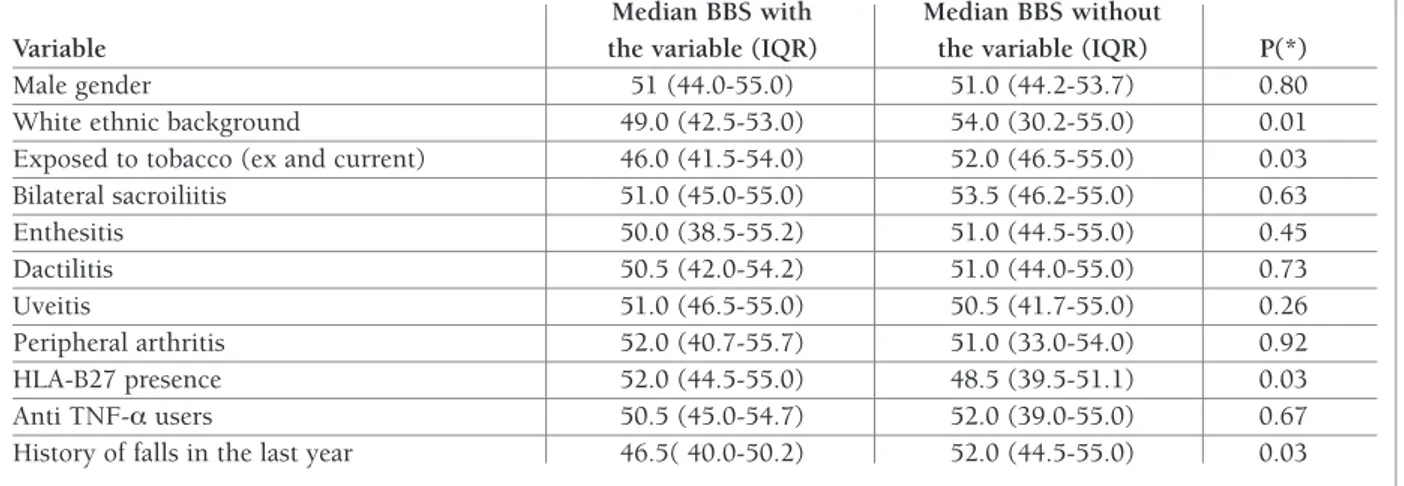
The comparison of BBS according to clinical, image findings and treatment data is shown on Table II. There it is possible to see that, patients with white ethnic background, exposure to tobacco and history of falls in the last year, had lower values of BBS.
Table III shows the correlation studies of BBS with age, disease duration and result of applied instruments. This table shows that all studied variables but disease duration had a negative correlation with BBS values.
Linear multivariable analysis showed that BASFI (with p=0.01; Beta coefficient=-0.05) and BASMI (p<0.0001; Beta coefficient= -1.35) were indepen-dently associated with BBS values.
DISCUSSION
The present results show that almost 1/3 of the stu -died axial SpA patients may be at greater risk of falling as they have a BBS under 45. Indeed, almost 1/4 of them did fall in the year prior to the study. The mul-tivariable analysis showed that the functional and the metrology indexes are the variables related indepen-dently with balance loss; both of them reflect SpA structural damage.
Exposure to tobacco, the presence of HLA-B27 and white ethnic background were associated with lower BBS in univariate analysis. A systematic literature
re-white patients. Caucasians are known to have higher prevalence of HLA-B27 in their SpA population than non-Caucasians21and this gene, although associated
with the development of SpA, cannot be linked to in-creased structural damage22that is supposed to be the
subjacent reason for the balance impairment. In fact, a study by Jamalyaria et al.23found that the non-white
population with ankylosing spondylitis have more dis-ease activity, greater functional loss and worse disdis-ease prognosis when compared to whites or Latinos.
Another finding of the present study was the asso-view by Villaverde-García et al.19showed that smoking
has a dose-dependent impact in progression of struc-tural damage in axial SpA that could lead to worse balan ce and explain our findings. The negative impact of smoking may be caused by increased systemic in-flammation; accelerated radiographic progression has also been observed in this context20. In addition,
smok-ers have poorer treatment adherence and worse re-sponse to anti TNF drugs when compared with never smokers20.
Worse balance was found in HLA-B27 positive and
N: number; IQR: interquartile range; SD: Standard deviation; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; ASDAS: Ankylosing Spondylitis Disease Activity Score; ESR: erythrocyte sedimentation rate; CRP: C reactive protein; BASMI: Bath Ankylosing Spondylitis Metrology Index; BASFI: Bath Ankylosing Spondylitis Functional Index; ASQol: Ankylosing Spondylitis Quality of Life questionnaire.
TABLE I. MAIN EPIDEMIOLOGICAL, CLINICAL AND TREATMENT DATA OF 55 PATIENTS WITH AXIAL SPONDYLOARTHRITIS
Male sex (n-%) 39/55 - 70.9%
Age (years) (mean+/- SD) 47.8±11.0
Auto declared ethnic background (n-%)
White 41/55 - 74.6% Non-white 14/55 - 25.4% Work incapacity (n-%) None 22/54 - 40.7% Partial 9 /54 - 16.6 % Total 23/54 - 42.5%
Exposure to tobacco (ex and current smokers) (n-%) 28/55 - 50.9%
Median disease duration (years) (IQR) 9.0 (5.0-13.0)
Clinical data
Bilateral sacroiliitis on MRI (n-%) 47/55 - 85.4%
Unilateral sacroiliitis on MRI (n-%) 8/55 - 14.5%
Non radiographic SpA (n-%) 2/55 - 3.6%
Peripheral arthritis (n-%) 8/55 - 14.5% Dactilitis (n-%) 5/55 - 9.0% Enthesitis (n-%) 34/55 - 61.8 % Uveitis (n-%) 17/55 - 30.9% HLA-B27 (n-%) 37/51 - 72.5% Treatment Data
Non-steroidal anti-inflammatory drugs users (n-%) 50/55 - 90.9%
Methotrexate users (n-%) 5/55 - 11.1%
Anti TNF-a drugs users (n-%) 30/55 - 54.5%
Applied instruments
BASDAI - Median (IQR) 3.4 (2.0-5.4)
ASDAS-ESR - Median (IQR) 2.4 (1.9-3.3)
ASDAS-CRP - Median (IQR) 2.7 (2.1-3.6)
BASMI - Median (IQR) 4.0 (3.0-7.0)
BASFI - Median (IQR) 4.0 (1.7-6.9)
TABLE II. STUDY OF BBS (BALANCE BERG SCALE) VALUES ACCORDING TO EPIDEMIOLOGICAL, CLINICAL AND TREATMENT VARIABLES
Median BBS with Median BBS without
Variable the variable (IQR) the variable (IQR) P(*)
Male gender 51 (44.0-55.0) 51.0 (44.2-53.7) 0.80
White ethnic background 49.0 (42.5-53.0) 54.0 (30.2-55.0) 0.01 Exposed to tobacco (ex and current) 46.0 (41.5-54.0) 52.0 (46.5-55.0) 0.03 Bilateral sacroiliitis 51.0 (45.0-55.0) 53.5 (46.2-55.0) 0.63 Enthesitis 50.0 (38.5-55.2) 51.0 (44.5-55.0) 0.45 Dactilitis 50.5 (42.0-54.2) 51.0 (44.0-55.0) 0.73 Uveitis 51.0 (46.5-55.0) 50.5 (41.7-55.0) 0.26 Peripheral arthritis 52.0 (40.7-55.7) 51.0 (33.0-54.0) 0.92 HLA-B27 presence 52.0 (44.5-55.0) 48.5 (39.5-51.1) 0.03
Anti TNF-a users 50.5 (45.0-54.7) 52.0 (39.0-55.0) 0.67
History of falls in the last year 46.5( 40.0-50.2) 52.0 (44.5-55.0) 0.03 IQR: interquartile range.
(*) P refers to the comparison of BBS values in patients with and without the variable described in the first column.
TABLE III. CORRELATION STUDIES OF BBS (BERG BALANCE SCALE) VALUES WITH AGE, DISEASE DURATION, DISEASE ACTIVITY INDEXES, FUNCTIONAL AND METROLOGY INDEXES AND QUALITY OF LIFE
Rho 95% confidence interval P
BASDAI -0.28 -0,51 to -0,008 0.03 ASDAS ESR -0.32 -0,54 to -0,05 0.01 ASDAS CRP -0.33 -0.55 to -0.06 0.01 BASFI -0.71 -0.82 to -0.55 <0.0001 BASMI -0.80 -0.88 to -0.67 <0.0001 ASQoL -0.56 -0.72 to -0.35 <0.0001 Age (years) -0.50 -0.68 to -0.25 <0.0001
Disease duration (years) -0.10 -0.36 to 0.17 0.44
BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; ASDAS: Ankylosing Spondylitis Disease Activity Score; ESR: erythrocyte sedimentation rate; CRP: C reactive protein; BASMI: Bath Ankylosing Spondylitis Metrology Index; BASFI: Bath Ankylosing Spondylitis Functional Index; ASQol: Ankylosing Spondylitis Quality of Life questionnaire.
ciation of disease activity with loss of balance. The link between disease activity with structural damage has been highlighted by a 12-year longitudinal study by Ramiro et al.24that showed that sustained increased
dis-ease activity may lead to new bone formation and ra-diographic progression mainly in the early phases of the disease. In the present, the three instruments used to measure disease activity correlated with balance loss although only in the univariate analysis, suggesting that the structural damage they originate are causing the problem. So, treating inflammation vigorously may be a strategy to avoid future loss of balance.
Balance is defined as postural adaptation to changes in the gravity center at rest and activity keeping it with-in the base of support with mwith-inimal postural sway25. It
requires a precise coordination of visual, auditory, pro-prioceptive, neuromuscular and central nervous sys-tem and it is necessary to accomplish daily activities that are important to keep ones’ independence25. Stu
-dies by Bot et al.26revealed that the thoracic kyphosis,
seen in advanced disease, causes a forward and down-ward displacement of the spine weight center. In order to maintain balance, compensatory movements in the lower extremities occur such as hip extension, knee
flexion and ankle plantar flexion. Arthritis and enthe-sitis in the lower extremity joints may affect this adap-tation25. Others noted that increased pelvic tilt (the
angle formed by the line passing from the head of the femur and the line connecting the middle of the sacral plateau) and decreased pelvic incidence (the angle be-tween the perpendicular line drawn to the sacral end-plate and the line connecting the midpoint of the sacral plateau and hip axis) affect balance27. All the
above-mentioned alterations are seen in patients with ad-vanced disease and offer an explanation for our results that showed association of loss of balance in those with worse BASFI and BASMI.
This study has limitations: it includes a small sam-ple of patients and it has a transversal design. The num-ber of falls were determinate by patients’ recollection and may suffer recall bias. Nevertheless, it does high-light the problem of loss of balance in SpA patients and the need to prevent functional loss in order to avoid this problem. Rehabilitation treatment, including pos-tural and proprioceptive exercises, seems effective on helping balance control4and should be included in the
treatment of these patients.
Summarizing, the present study shows that SpA pa-tients may have important loss of balance that is asso-ciated independently with loss of function and mobi lity. CORRESPONDENCE TO
Betania Longo
Rua Luis Leitner, 50 - Bigorrilho CEP: 80.710-390 - Curitiba (PR) - Brazil. E-mail: [email protected]
REFERENCES
1. Pompeu JE, Romano RS, Pompeu SM, Lima SM. Static and dy-namic balance in subjects with ankylosing spondylitis: literature review. Rev Bras Reumatol. 2012; 52:409-416.
2. Sawacha Z, Carraro E, Del Din S, Guiotto A, Bonaldo L, Punzi L et al. Biomechanical assessment of balance and posture in sub-jects with ankylosing spondylitis. J. Neuroeng Rehabil. 2012; 9:63.
3. De Nunzio AM, Iervolino S, Zincarelli C, Di Gioia L, Rengo G, Multari V, et al. Ankylosing spondylitis and posture control: the role of visual input. Biomed Res Int. 2015; 2015:948674 4. Favorable effect of rehabilitation on balance in ankylosing
spondylitis: a quasi-randomized controlled clinical trial. De-montis A, Trainito S, Del Felice A, Masiero S.Rheumatol Int. 2016; 36:333-339.
5. Adam M, Erkan AN, Arslan D, Leblebici B, Ozluoglu L, Nafiz Akman M. High-frequency sensorineural hearing loss in pa-tients with ankylosing spondylitis: Is it an extraarticular feature of disease? Rheumatol Int.2008; 28: 413–417
6. Amor-Dorado JC, Barreira-Fernandez MP, Vazquez-Rodriguez TR, Gomez-Acebo I, Miranda-Filloy JA, Diaz de Teran T et al. Audiovestibular manifestations in patients with ankylosing
spondylitis. Medicine (Baltimore). 2011; 90:99–109 7. van der Weijden MA, Claushuis TA, Nazari T, Lems WF,
Dijk-mans BA, van der Horst-Bruinsma IE. High prevalence of low bone mineral density in patients within 10 years of onset of ankylosing spondylitis: a systematic review. Clin Rheumatol. 2012; 31:1529-1535.
8. Batur EB, Karataş GK. Do postural changes affect balance in pa-tients with ankylosing spondylitis? J Rehabil Med. 2017; 49: 437-440.
9. Lee AY, Tan J, Koh J, Fook-Chong SM, Lo NN, Howe TS. Five-year outcome of individuals with hip fracture admitted to a Singapore hospital: quality of life and survival rates after treat-ment. J Am Geriatr Soc 2012, 60: 994–996.
10. Aydog E, Depedibi R, Bal A, Eksioglu E, Unlu E, Cakci A. Dy-namic postural balance in ankylosing spondylitis patients. Rheumatology (Oxford). 2006; 45:445–448.
11. Rudwaleit M, van der Heijde D, Landewé R, Listing J, Akkoc N, Brandt J et al. The development of assessment of Spondy-loarthritis International Society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann Rheum Dis 2009; 68:777-783.
12. Hermann KG, Baraliakos X, van der Heijde DM, Jurik AG, Lan-dewé R, Marzo-Ortega H, et al. Descriptions of spinal MRI le-sions and definition of a positive MRI of the spine in axial spondyloarthritis: a consensual approach by the ASAS/OMER-ACT MRI study group. Ann Rheum Dis. 2012 ;71:1278-1288. 13. Garrett S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P, Calin A. A new approach to defining disease status in ankylos-ing spondylitis: the Bath Ankylosankylos-ing Spondylitis Disease Activ-ity Index. J Rheumatol 1994; 21:2286-2291.
14. Van der Heijde D, Lie E, Kvien TK, Sieper J, van den Bosch F, Listing J et al. ASDAS, a highly discriminatory ASAS-endorsed disease activity score in patients with ankylosing spondylitis. Ann Rheum Dis 2009; 68:1811-1818.
15. Calin A, Garrett S, Whitelock H, Kennedy LG, O´Hea J, Malo-rie P, et al. A new approach to defining functional ability in anky-losing spondylitis: the development of the Bath Ankyanky-losing Functional Index. J Rheumatol. 1994; 21:2281-2285. 16. Sieper J, Rudwaleit M, Baraliakos X, Brandt J, Braun J,
Burgos-Vargas R, et al. The Assessment of SpondyloArthritis interna-tional Society (ASAS) handbook: a guide to assess spondy-loarthritis. Ann Rheum Dis. 2009;68 Suppl 2:ii1-44
17. Berg K, Wood-Dauphinee S, Williams JI, Maki, B. Measuring balance in the elderly: validation of an instrument. Can. J. Pub. Health; 1992; S2: S7-S11
18. Shumway-Cook A, Baldwin M, Polissar NL, Gruber W. Pre-dicting the probability for falls in community-dwelling older adults. Phys Ther. 1997; 77: 812-819.
19. Villaverde-García V, Cobo-Ibáñez T, Candelas-Rodríguez G, Seoane-Mato D, Campo-Fontecha PDD, Guerra M, et al. The ef-fect of smoking on clinical and structural damage in patients with axial spondyloarthritis: A systematic literature review. Semin Arthritis Rheum. 2017; 46:569-583.
20. Glintborg B, Højgaard P, Lund Hetland M, Steen Krogh N, Kollerup G, Jensen J, et al. Impact of tobacco smoking on re-sponse to tumour necrosis factor-alpha inhibitor treatment in patients with ankylosing spondylitis: results from the Danish nationwide DANBIO registry. Rheumatology (Oxford). 2016; 55:659-668.
21. Stolwijk C, Boonen A, van Tubergen A, Reveille JD. Epidemiol-ogy of spondyloarthritis. Rheum Dis Clin North Am. 2012;
38:441-476.
22. Reveille JD. Biomarkers for diagnosis, monitoring of progres-sion, and treatment responses in ankylosing spondylitis and ax-ial spondyloarthritis. Clin Rheumatol. 2015; 34:1009-1018. 23. Jamalyaria F, Ward MM, Assassi S, Learch TJ, Lee M, Gensler LS,
et al. Ethnicity and disease severity in ankylosing spondylitis a cross-sectional analysis of three ethnic groups. Clin Rheumatol. 2017;36: 2359-2364.
24. Ramiro S, van der Heijde D, van Tubergen A, Stolwijk C, Douga-dos M, van den Bosch F, et al. Higher disease activity leads to more structural damage in the spine in ankylosing spondylitis: 12-year longitudinal data from the OASIS cohort. Ann Rheum
Dis. 2014; 73:1455-1461.
25. Uckun A, Sezer I. Ankylosing Spondylitis and Balance. Eurasian J Med. 2017; 49:207-210.
26. Bot SD, Caspers M, Van Royen BJ, Toussaint HM, Kingma I. Biomechanical analysis of posture in patients with spinal kypho-sis due to ankylosing spondylitis: a pilot study. Rheumatology 1999; 38: 441-443.
27. Lee JS, Suh KT, Kim JI, Goh TS. Analysis of sagittal balance of ankylosing spondylitis using spinopelvic parameters. J Spinal Disord Tech. 2014; 27: 94-98.