w w w . r b o . o r g . b r
Review
article
Pseudoaneurysm
after
arthroscopic
procedure
in
the
knee
夽
Edmar
Stieven
Filho
a,∗,
Guilherme
Rufini
Isolani
b,
Filipe
Ribas
Baracho
b,
Ana
Paula
Gebert
de
Oliveira
Franco
c,
Luiz
Antônio
Ridder
Bauer
a,
Mario
Namba
a aSportsTraumatologyandArthroscopyCenter,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,BrazilbHospitaldeClínicas,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil cPontifíciaUniversidadeCatólicadoParaná(PUCPR),Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20March2014 Accepted28April2014 Availableonline16March2015
Keywords:
Anteriorcruciateligament Arteries
Falseaneurysm Arthroscopy Knee
a
b
s
t
r
a
c
t
Theaimofthisstudywastoreviewallcasesofpseudoaneurysmintheliterature,in predom-inantlyarthroscopicproceduresontheknee,andtoreportonacaseofpseudoaneurysm thatwetreated.Abibliographicsearchwasconductedforscientificarticlespublishedin Brazilianandforeignperiodicalsoverthelast23years.Forty-sevencaseswerefound,in40 articles.Inadditiontothese47cases,therewasthecasethatwetreated,whichwasalso includedinthedata.Amongtheoperationsthatprogressedwithformationofa pseudoa-neurysm,60%werecasesofmeniscalinjuriesand23%,anteriorcruciateligamentinjuries. In46%ofthecases,thearteryaffectedwiththepopliteal,andin21%,theinferomedial genicularartery.Thecommonestclinicalsymptomwaspain(37%),followedbypulsating tumor(31%),edemaofthecalf(12%)andhemarthrosis(11%).Themediantimetakento makethediagnosiswas11days,butitrangedfromonedayto10weeksafterthe proce-dure.Althoughrare,pseudoaneurysmsareariskthatisinherenttoarthroscopicsurgery. Allpatientsshouldbemadeawareofthevascularrisks,eveninsmall-scaleprocedures.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Pseudoaneurisma
após
procedimento
artroscópico
no
joelho
Palavras-chave:
Ligamentocruzadoanterior Artérias
Falsoaneurisma Artroscopia Joelho
r
e
s
u
m
o
Oobjetivodeste estudoé revisarnaliteratura todosos casosdepseudoaneurismaem procedimentospredominantementeartroscópicosdojoelhoerelatarumcasode pseudoa-neurismatratadopelosautores.Foifeitaumapesquisabibliográficapormeiodeartigos científicospublicadosemperiódicosnacionaiseinternacionaisnosúltimos23anos.Foram levantados47casos,em40artigos.Somou-seaos47umcasodosautoresdesteestudoque foiincluídonosdados.Dascirurgiasquecursaramcompseudoaneurisma,60%setratavam
夽
WorkdevelopedattheUniversidadeFederaldoParaná,Curitiba,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](E.S.Filho). http://dx.doi.org/10.1016/j.rboe.2015.03.001
delesõesmeniscaise23%delesõesdoligamentocruzadoanterior.Em46%doscasosa artériaacometidafoipoplíteaeem21%aartériagenicularinferomedial.Osintomaclínico maiscomumfoidor(37%),seguidodetumorpulsátil(31%),edemadepanturrilha(12%)e hemartrose(11%).Amedianadotempoparadiagnósticofoide11dias,masvarioudeum diaaté10semanasapósoprocedimento.Apesarderaro,opseudoaneurismaéumrisco inerenteàcirurgiaartroscópica.Todopacientedevesernotificadodosriscosvasculares, mesmoemprocedimentosdepequenoporte.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Kneearthroscopyisamongthemostcommonlyperformed surgicalproceduresfortreatingsportsinjuries.1Arthroscopic reconstructionoftheanteriorcruciateligament(ACL)alone accountsfor75,000casesperyearintheUnitedStates.2
Useofarthroscopyhasgrownbecauseitentailslessinjury tosofttissuesinordertoperformtheprocedure.With pre-ciseguidesanduseofcameras,itispossibletoincreasethe surgeon’sefficacy and diminishthedamagetothepatient. However,directviewingofthesurrounding structuresisno longerdoneroutinely,whichmayleadtounexpectedinjuries. Oneexampleofthisisthereportsofpseudoaneurysmsafter arthroscopicprocedureshavebeenperformedontheknee.3,4 Pseudoaneurysmsarecausedbyincompleteinjurytothe arterialwall,withextravasationofbloodthatiscontainedby thesurroundingtissues.Thisbloodaccumulationisorganized inafibrouscapsulewiththepresenceofturbulentflowinside it5(Fig.1).
Over the course of the natural evolution of pseudoa-neurysms, they may increase insize untilthey rupture or causeulcerationintheneighboringstructures.3,5,6
Becausepseudoaneurysmsareararecomplication,ahigh degreeof suspicion isneeded foran early diagnosis to be made.7 The literature of pseudoaneurysms subsequent to arthroscopicproceduresonthekneeissparseandonlyafew reportsexist.
Theobjective ofthis study was toreview all the cases ofpseudoaneurysmintheliteratureresultingfrom predom-inantly arthroscopic procedures on the knee (treatments relatingto ACL,meniscalinjuries,synovectomyand osteo-chondritis)andreportonacaseofpseudoaneurysmthatwe treated.
Method
Abibliographicsurveywasconductedamongscientificarticles publishedinBrazilianandforeignperiodicalsoverthelast23 years,usingthePubMedandBireme databases.Thesurvey wasconductedintwostagesonthePubMedwebsite:firstly, usingthetermspseudoaneurysmORfalseaneurysmandkneeOR
cruciateORarthroscopy; and secondly,usingpseudoaneurisma
OR falso aneurisma and joelho OR cruzado OR artroscopia. In the Bireme database, the terms were used separately. Ten combinations would be needed in order to have a simi-larsearch, asfollows:pseudoaneurysm knee, pseudoaneurysm
cruciate,pseudoaneurysmarthroscopy,falseaneurysmknee,false aneurysmcruciate,falseaneurysmarthroscopy,pseudoaneurisma joelho,pseudoaneurismacruzado,pseudoaneurismaartroscopia.
Reports on cases of pseudoaneurysm of the knee sub-sequent to predominantly arthroscopic procedures were selected (cases relating toACL,meniscalinjuries, synovec-tomy and osteochondritis).Someother articleswere found throughexaminingthereferencelistsofthearticlesselected. Noprospectiveorretrospectivestudiesonthissubjectwere found,andnotevenanycaseseries.Themaximumnumberof casesreportedperarticlewasthree.8Thereviewwaschecked uptoJune24,2011.
Articlesinfivelanguageswerefound:English(31),French (3),Portuguese(1),German(1)andSerbian(1).Thepointsof interestinthearticleinSerbianwerekindlytranslatedinto Englishforussothattheycouldbeincludedinthisstudy.9
Forthepurposesofthepresentstudy,itwasnotof inter-esttoreviewtheopinionsofspecialistsbut,rather,thecase reports,giventhattherewasnostrongerevidencethanthis, onthissubject,uptothetimeofthisstudy.
Case
report
Ourpatientwasa17-year-oldmalewhopresentedacomplete tearoftheACLsubsequenttotwistinghisrightkneewhile playinghandball.ArthroscopicreconstructionoftheACLwas performedusingagraftfromtheflexortendonsoftheknee.
Two and a half years later, he twisted his right knee again,andthisledtoacomplaintofinstabilityandrecurrent episodesofjointeffusion.Hesoughtassistanceatthe ortho-pedicsserviceofthe SportsTraumatology andArthroscopy Center,whereadiagnosisofanewACLinjurywasmade. Sur-gicalrevisionofthereconstructionwasthereforescheduled. Thegraftusedwasfromthetendonofthequadricepsmuscle. Extensive repairtothefemoralintercondylarareawasalso performed.
Partial injury of the artery Organization of the pseudoaneurysm
A
B
Fig.1–Schematicdrawingoftheformationofapseudoaneurysm.
Table1–Diagnosesfoundintheliteraturesurveyed.
Diagnosis Numberofpatients Percentage(%)
Meniscus 29 60.41
Synovitis 3 6.25
Arthrosis 2 4.16
ACL 11 22.91
Osteochondritis 1 2.08
Synovectomy 1 2.08
Baker’scyst 1 2.08
Review
of
the
literature
Forty-sevencasesinfortyarticlesweresurveyed.4,6–43In addi-tion,oursinglecasedescribedabovewasincludedinthedata. Thefirstcaseofpseudoaneurysmsubsequenttoan arthro-scopicprocedureonthekneedatesbackto1979.13Wedonot believethatanyoldercasesexist,becausearthroscopyonly becamepopularinthe1990s.
Fromthepresentinvestigation,75%ofthepatientswere maleand25%werefemale,andtheiragesrangedfrom13to 69years.Themeanageofthemalepatientswas32.30years (14.92)and themedianwas31 years.Themean ageofthe femalepatientswas33.87years(21.19)andthemedianwas 32.50.
Thediagnosesfoundinthestudiesinvestigatedincluded thefollowing:meniscaldisorders(60.41%),ACL(22.91%), syn-ovitis(6.25%),arthrosis(4.16%)andalsoosteochondritisand Baker’scyst(Table1).
Thetimetakentoreachthediagnosisrangedfromoneto 180days,withameanof11.90days(35.25)andmedianof11 days.
Resection was the treatment most frequently seen in theliterature,accountingfor75% ofthecases,followed by embolization,with20.83%.Amongthecasesstudied,onewas resolvedusingapercutaneousprosthesisandthetreatment usedwasnotspecifiedinoneothercase.
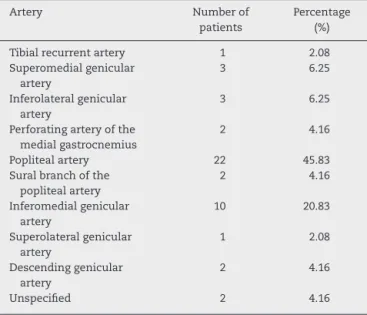
The arteries most affected were the popliteal artery (45.83%) and the inferomedial genicular artery (20.83%) (Table2).
To detect the pseudoaneurysm, complementary exam-inations were used, such as: echo Doppler, arteriography, computed axial tomography, angiotomy with contrast,
Table2–Arteriesaffectedinthecasesthatwerefound intheliterature.
Artery Numberof
patients
Percentage (%)
Tibialrecurrentartery 1 2.08
Superomedialgenicular artery
3 6.25
Inferolateralgenicular artery
3 6.25
Perforatingarteryofthe medialgastrocnemius
2 4.16
Poplitealartery 22 45.83
Suralbranchofthe poplitealartery
2 4.16
Inferomedialgenicular artery
10 20.83
Superolateralgenicular artery
1 2.08
Descendinggenicular artery
2 4.16
Unspecified 2 4.16
aspiration and even inspection by means of surgery. The complementaryexaminationsmostfrequentlyrequestedin the studies reviewed here were arteriography(41.66%) and echoDoppler(39.58%).
Amongthe48patientsevaluatedinthedifferentstudies,34 presentedpain,29hadapulsatiletumor,11hadedemaofthe calf,eighthadanon-pulsatiletumorandonehadparesthesia (Table3).
Table3–Signsandsymptomsreportedintheliterature surveyed.
Signsandsymptoms Numberofcases Percentage(%)
Pain 34 36.55
Pulsatiletumor 29 31.18
Edemaofthecalf 11 11.82
Hemarthrosis 10 10.75
Non-pulsatiletumor 8 8.6
Paresthesia 1 1.07
Discussion
Kneearthroscopyisasafeandcommonlyperformed proce-dure,withfewcomplications.Theincidencerateofnerveand vascularinjuriesdescribedsubsequenttoarthroscopyranges from 0.56% to0.80% in large series. This low incidence is perhapsoneofthereasonswhyvascularcomplicationsare difficulttodiagnoseandarediagnosedlate.7
Thegreaterincidenceofpseudoaneurysmsfoundamong men(75%)isduetothefactthatthesekneeinjuriesoccur inyoungpeoplepracticingsportsactivities,whoaremostly men.However,thenumberofwomenwhopracticesportsis growingandtheratioofinjuriesperhourofsportspracticeis loweramongwomen.44
Theriskofarterialinjuryduringkneesurgeryisrelatedto kneeanatomy,sincethevesselsareclosetothejointcapsule. Duringkneeflexion,thearteriesaremovedforwards,toward theposteriorcapsule,andthepoplitealarteryisthen sepa-ratedfromthecapsulebyathinlayeroffat,whichmaybe thereasonwhythepoplitealarteryissofrequentlyaffected. Sincetheposteriorpartofthekneeisdifficulttoview dur-ingarthroscopyanduseofatourniquetmakesitimpossible toviewbleedingimmediately,thesevascularinjuriesarenot easilydiagnosed.Forthisreason,thelimbcirculationshould becarefullycheckedafterthesurgery.7
Rupture of the artery wall is necessary for a pseudoa-neurysmtodevelop.However,apseudoaneurysmmayform afterarthroscopywithoutany historyofpenetrationofthe knee capsuleorvesselwall. Onehypothesisfor explaining thisrelates tothe highlevels ofstress appliedtotheknee structuresandarteriesduringthearthroscopicprocedure.For example,this can be seen inarthroscopic surgeryto treat injuriestothemedialmeniscus,inwhich insomecasesit isnecessarytouseahighdegreeofvarusforceinorderto achievegoodviewing.Anotherhypothesisthatismore plau-sibleisthatpartialinjurytothearterymayoccuratthetimeof constructingtheaccessroutesforthearthroscopy.Theaccess portalisopenedontheanteromedialandanterolateralface oftheknee,closetothesuperiorgeniculararteries.Thereis alsotheaccessrouteforgraftharvesting,whichinthecaseof patellargraftsandgraftsfromthekneeflexortendonsisclose totheinferiorgeniculararteries.7
Knowledgeofthevascularanatomyofthekneeis essen-tialinordertoavoidthistypeofcomplication.Thefollowing arteriessupplythekneejoint:thegenicularbranchesofthe femoral,poplitealandanteriortibialrecurrentarteriesandthe descendingbranchofthe lateral circumflexfemoralartery. Themajorityofthe bloodsupplyforboththeACL andthe posteriorcruciateligamentcomesthroughligamentbranches ofthemedialgenicularartery(whichalsosuppliesthe syno-vialmembrane and thelateral margin ofthe menisci)and alsothroughsometerminalbranchesoftheinferomedialand inferolateralgeniculararteries.Thesevesselsbranchout to formarichsynovialplexusthatcontributestoanetworkof intracapsularvesselsthatsurroundtheACL.45
Arthroscopic surgery that requires bone tunnels also requirestheuseofguidesthatensurethattheholesaredrilled throughthebonesisthecorrectplaces.Tunnelconstruction isusuallystartedbymeansofasteelwireofdiameter2mm
(guidewire).Afterthesurgeonhasdecidedthatthepositioning iscorrect,acannulateddrillbitispassedalongthisguidewire inorder todrillthe bone.Here,twoimportantpointsarise withregardtodiscussingpseudoaneurysms.Thefirstrelates tosoft-tissuepenetration,inthatthesewiresarepassedinto thesofttissuesblindly,whichmayleadtopartialinjuriesto arteries.Thesecondrelatestoprecision,inthatifpoorquality materialsareused,thismayleadtoguidewireintounplanned locations,evenifthetechniqueisappliedcorrectly.
Pain was the commonest symptom among the cases reported, but its nonspecific nature sometimes may not havehelped inmakingthe diagnosis.Pulsatiletumorsand hemarthrosiswitharterialbloodwerepresentinmanyofthe casesand theirpresenceledtoahighdegreeofsuspicion. Insomecases,thetumorwasdescribedasnon-pulsatile,but noneoftheauthorsofthesecasestudiesdiscussedthis.
Thediagnosiscanbemadeclinicallythroughthepresence ofapainfulpulsatilemassofgrowingsize,inassociationwith palpablefremitusandasystolicheartmurmur.The diagno-sis can beconfirmed bymeans ofechoDoppler, magnetic resonanceimagingandarteriography.37Thefollowing com-plicationsofpseudoaneurysmsmayoccur:hemorrhage,pain andspaceoccupationeffectssuchasneurological compres-sion,neuralgia,venouscompressionandthrombosis.46
Ahighdegreeofsuspicionneedstobemaintainedinorder toavoiddelayeddiagnosis.Themedianlengthoftimetaken tomakethediagnosiswasfoundtobe11days,butitranged fromonedayto10weeksaftertheinitialprocedure.37
Althoughrare,pseudoaneurysmisariskthatisinherentto arthroscopicsurgery.Allpatientsneedtobenotifiedregarding thevascularrisks,evenincasesofsmall-sizedprocedures.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MiyasakaKC,DanielDM,LsmPH.Theincidenceofknee ligamentinjuriesinthegeneralpopulation.AmJKneeSurg. 1991;4(1):3–8.
2.GrossmanMG,ElAttracheNS,ShieldsCL,GlousmanRE. Revisionanteriorcruciateligamentreconstruction:three-to nine-yearfollow-up.Arthroscopy.2005;21(4):418–23. 3.ShawA,StephenAB,LundJN,BungayP,DeNunzioM.
Geniculatearterialpseudoaneurysmformationfollowing traumaandelectiveorthopaedicsurgerytotheknee:2case reportsandareviewoftheliterature.JRadiolCaseRep. 2009;3(3):12–6.
4.MelloW,deBritoWE,MigonEZ,BorgesA.Pseudoaneurysmof themedialinferiorgeniculararteryafteranteriorcruciate ligamentreconstruction.Arthroscopy.2011;27(3):442–5. 5.MiyamottoM,CésarR,MoreiraR,ErzingerFL,Franc¸aGJ,
GinesteA.Pseudo-aneurismaidiopáticodaartériapoplítea.J VascBras.2004;3(2):169–71.
7. AudenaertE,VuylstekeM,LissensP,VerhelstM,VerdonkR. Pseudoaneurysmcomplicatingkneearthroscopy.Acase report.ActaOrthopBelg.2003;69(4):382–4.
8. DinhA,BrunetAP,MaatoukM,DieboldS,FavoliP.Arterial complicationsofarthroscopicmeniscectomies.Aproposof threecases.AnnChir.1993;47(6):547–52.
9. MilankovM,Ninkovi´cS,Stankovi´cM.Falseaneurysm followingarthroscopicmeniscectomyoftheknee.MedPregl. 2004;57(5–6):289–91.
10.ArmatoDP,CzameckiD.Geniculatearterypseudoaneurysm: ararecomplicationofarthroscopicsurgery.AJRAmJ Roentgenol.1990;155(3):659.
11.AldrichD,AnschuetzR,LoPrestiC,FumichM,PitlukH, O’BrienW.Pseudoaneurysmcomplicatingkneearthroscopy. Arthroscopy.1995;11(2):229–30.
12.BecherC,BurgerUL,AllenbergJR,KaufmannGW,Thermann H.Delayeddiagnosisofapseudoaneurysmwithrecurrent hemarthrosisofthekneejoint.KneeSurgSportsTraumatol Arthrosc.2008;16(6):561–4.
13.BellKA,SimonBK.Aneurysmofpoplitealarteryaftermedial meniscectomy:anunusualcomplication.SouthMedJ. 1979;72(9):1126–34.
14.BeckDE,RobisonJG,HallettJWJr.Poplitealartery pseudoaneurysmfollowingarthroscopy.JTrauma. 1986;26(1):87–9.
15.BrasseurP,SukkariehF.Iatrogenicpseudo-aneurysmofthe poplitealartery.Complicationofarthroscopicmeniscectomy. Aproposofacase.JRadiol.1990;71(4):301–4.
16.CarlinRE,PapenhausenM,FarberMA,RonningenE,Mauro MA,MarstonWA,etal.Suralarterypseudoaneurysmsafter kneearthroscopy:treatmentwithtranscatheter
embolization.JVascSurg.2001;33(1):170–3. 17.EvansJD,deBoerMT,MayorP,ReesD,GuyAJ.
Pseudoaneurysmofthemedialinferiorgenicularartery followinganteriorcruciateligamentreconstruction.AnnR CollSurgEngl.2000;82(3):182–4.
18.GuermaziA,ZagdanskiAM,deKervilerE,BourrierP,FrijaJ. Poplitealarterypseudoaneurysmrevealedbydeepvein thrombosisafterarthroscopicmeniscectomy.EurRadiol. 1996;6(2):217–9.
19.GuyRJ,SpaldingTJ,JarvisLJ.Pseudoaneurysmafter
arthroscopyoftheknee.Acasereport.ClinOrthopRelatRes. 1993;(295):214–7.
20.HilbornM,MunkPL,MiniaciA,MacDonaldSJ,RankinRN, FowlerPJ.Pseudoaneurysmaftertherapeuticknee arthroscopy:imagingfindings.AJRAmJRoentgenol. 1994;163(3):637–9.
21.HofmannW,ForstnerR,ForstnerK.Pseudoaneurysmofthe pediatricpoplitealarteryafterarthroscopicmeniscus resection.Chirurg.2000;71(4):469–71.
22.HusseinMK,LakkisSA.Pseudoaneurysmofthepopliteal arteryfollowingarthroscopicmeniscectomy.BullHospJtDis. 1998;57(3):162–4.
23.JanssenRP,ScheltingaMR,SalaHA.Pseudoaneurysmofthe poplitealarteryafteranteriorcruciateligament
reconstructionwithbicorticaltibialscrewfixation. Arthroscopy.2004;20(1):E4–6.
24.KankoM,BulucL,YavuzS,MuezzinogluS,BerkiT.Veryrare aetiologyofgiantpoplitealpseudoaneurysm:anterior cruciateligamentsurgery.PostgradMedJ.2008;84(989):158–9. 25.KissH,DrekonjaT,GrethenC,DornU.Postoperative
aneurysmofthepoplitealarteryafterarthroscopic meniscectomy.Arthroscopy.2001;17(2):203–5.
26.LafontaineM,KhouryA.Falseaneurysmofthekneeafter arthroscopy.ActaOrthopBelg.1997;63(3):215–7.
27.LeeB,ParkSW,NahJC,KimSW,KooBI,ChoWH,etal. Clinicalimage:poplitealarterypseudoaneurysmfollowing
arthroscopicsynovectomy.ArthritisRheum.2007;56(10): 3432.
28.LeeKB,SongSY,KwonDJ,ShinJ,PaikSH.Pseudoaneurysmof themedialsuperiorgeniculararteryafterarthroscopicpartial meniscectomy.ClinOrthopSurg.2009;1(3):173–5.
29.ManningMP,MarshallJH.Aneurysmafterarthroscopy.JBone JtSurgBr.1987;69(1):151.
30.MilankovM,MiljkovicN,StankovicM.Pseudoaneurysmof themedialinferiorgeniculararteryfollowinganterior cruciateligamentreconstructionwithhamstringtendon autograft.Knee.2006;13(2):170–1.
31.MuftySJr,SmitsP,FeyenJ.Pseudoaneurysmofthesuperior medialgeniculararteryfollowingkneearthroscopy.Knee SurgSportsTraumatolArthrosc.2011;19(8):1314–5. 32.MullenDJ,JabajiGJ.Poplitealpseudoaneurysmand
arteriovenousfistulaafterarthroscopicmeniscectomy. Arthroscopy.2001;17(1):E1.
33.OmaryR,StulbergSD,VogelzangRL.Therapeutic embolizationoffalseaneurysmsofthesuperiormedial geniculararteryafteroperationsontheknee.Areportoftwo cases.JBoneJtSurgAm.1991;73(8):1257–9.
34.PereiraJuniorED,MestrinerLA,PereiraED,DominguesRP, CardosoMP.Pseudoaneurismadeartériagenicularapós cirurgiaartroscópicadejoelho:relatodedoiscasos.Acta OrtopBras.2010;18(2):104–6.
35.RittMJ,TeSlaaRL,KoningJ,BruijnJD.Popliteal
pseudoaneurysmafterarthroscopicmeniscectomy.Areport oftwocases.ClinOrthopRelatRes.1993;(295):198–200. 36.PotterD,Morris-JonesW.Poplitealarteryinjurycomplicating
arthroscopicmeniscectomy.Arthroscopy.1995;11(6): 723–6.
37.SarrosaEA,Ogilvie-HarrisDJ.Pseudoaneurysmasa complicationofkneearthroscopy.Arthroscopy. 1997;13(5):644–5.
38.TaboadaMartínR,CapelAlemánA.Arteriovenousfistulaand poplitealpseudoaneurysmafterarthroscopicmeniscectomy: endovasculartreatmentwithaViabahn®stent.Radiologia.
2012;54(1):94–5.
39.TozziA,FerriE,SerraoE,ColonnaM,DeMarcoP,Mangialardi N.Pseudoaneurysmofthedescendinggeniculararteryafter arthroscopicmeniscectomy:reportofacase.JTrauma. 1996;41(2):340–1.
40.VassalloP,ReiserMF,StrobelM,PetersPE.Popliteal pseudoaneurysmandarteriovenousshuntfollowing arthroscopicmeniscectomy:casereport.CardiovascInterv Radiol.1989;12(3):142–4.
41.KpV,YoonJR,NhaKW,YangJH,LeeJH,JegalH.Popliteal arterypseudoaneurysmafterarthroscopiccystectomyofa poplitealcyst.Arthroscopy.2009;25(9):1054–7.
42.VincentGM,StanishWD.Falseaneurysmafterarthroscopic meniscectomy.Areportoftwocases.JBoneJtSurgAm. 1990;72(5):770–2.
43.ReginaG,FulloneM,TodiscoC,GrecoL,TestiniM,IuscoD, etal.Associationofdeepvenousthrombosisandpopliteal pseudoaneurysmafterarthroscopicmeniscectomy.Minerva Chir.2000;55(11):803–5.
44.BjordalJM,ArnłyF,HannestadB,StrandT.Epidemiologyof anteriorcruciateligamentinjuriesinsoccer.AmJSports Med.1997;25(3):341–5.
45.AldridgeJM,WeaverJP,MallonWJ.Avulsionofthemiddle genicularartery:apreviouslyunreportedcomplicationof anteriorcruciateligamentrepair.Acasereport.AmJSports Med.2002;30(5):748–50.