w w w . r b o . o r g . b r
Original
Article
Evaluation
of
patients
submitted
to
the
arthroscopic
treatment
of
the
lateral
epicondylitis
refractory
to
the
conservative
treatment
夽
Fábio
Alexandre
Martynetz
a,b,c,
Fernando
Ferraz
Faria
c,∗,
Mauro
José
Superti
c,
Salim
Mussi
Filho
c,
Larissa
Martins
Mourão
Oliveira
aaPontifíciaUniversidadeCatólicadoParaná,Curitiba,PR,Brazil
bInstituteofOrthopedicsandTraumatologyofToledo,Toledo,PR,Brazil
cOrthopedicsandTraumatologyService,CajuruUniversityHospital,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6November2012 Accepted9April2013
Keywords:
Tenniselbow/surgery Tenniselbow/complications Tenniselbow/therapy Arthroscopy
a
b
s
t
r
a
c
t
Objective:toevaluatetheresultsofthearthroscopictreatmentofthelateralepicondylitis. Methods:weevaluated14patients(15elbows)submittedtothearthroscopictreatmentof thelateralepicondylitisrefractorytotheconservativetreatment,whichwasrealizedfor aminimumperiodof18months.Beyondthedemographicdatacollection,patientswere evaluatedaccordingtothearthroscopicclassificationofBakeretal.,theDisabilitiesofthe Arm,Shoulder,andHand(DASH)questionnaireandtheMayoElbowPerformanceScore (MEPS).Thepatients’agesrangedbetween23and56years(average46years)(eightmales andsixfemales).Ofthe15elbows,12werethedominantandonepatienthadbilateral lesion.Thefollow-upaftersurgerywasminimum24monthsandmaximum72months (average41months).
Results:wefound,accordingtothearthroscopicclassificationofBakeretal.,twopatients withtypeIlesions,ninewithtypeIIlesionsandthreewithtypeIIIlesions.Wefoundthe followingcomplications:onepatientwithaltered sensitivityintheregionofthelateral portal,onewithadeficitoftendegreesinlength,onewithsynovialplicaandonewith synovitisinthelateralcompartment.OurscoreontheDASHquestionnairewasminimum of32pointsandmaximumof120points(average57points)andthescaleofMEPShada minimumscoreof60pointsandamaximumof100points(average90points).
Conclusion:thearthroscopictreatmentofthelateralepicondylitis,plusinsurance,provides satisfactoryresults.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedattheOrthopedicsandTraumatologyService,CajuruUniversityHospital,Curitiba,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.F.Faria).
2255-4971/$–seefrontmatter©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Avaliac¸ão
de
pacientes
submetidos
ao
tratamento
artroscópico
da
epicondilite
lateral
refratária
ao
tratamento
conservador
Palavras-chave:
Cotovelodetenista/cirurgia Cotovelode
tenista/complicac¸ões Cotovelodetenista/terapia Artroscopia
r
e
s
u
m
o
Objetivo: avaliarosresultadosdotratamentoartroscópicodaepicondilitelateral.
Métodos:foramavaliados14pacientes(15cotovelos)submetidosaotratamentoartroscópico daepicondilitelateralrefratáriaaotratamentoconservador,oqualfoifeitoporumperíodo mínimode18meses.Alémdacoletadedadosdemográficos,ospacientesforam avalia-dossegundoaclassificac¸ãoartroscópicadeBakeretal.,oquestionárioDisabilitiesofthe Arm,Shoulder,andHand(DASH)eoMayoElbowPerformanceScore(MEPS).Asidadesdos pacientesvariaramentre23e56anos(médiade46)eforamoitodosexomasculinoeseis dofeminino.Dos15cotovelos,12eramdomembrodominanteeumpacientetinhalesão bilateral.Oseguimentoapósacirurgiafoidenomínimo24mesesenomáximo72meses (médiade41).
Resultados: foramconstatadas,segundoaclassificac¸ãoartroscópicadeBakeretal.,dois pacientescomlesãodotipoI,novecomlesãodotipoIIetrêscomlesãodotipoIII. Encon-tramosasseguintescomplicac¸ões:umpacientecomalterac¸ãodasensibilidadenaregião doportallateral,umcomdéficitdedezgrausnaextensão,umcomplicasinovialeum comsinoviteemcompartimentolateral.Nossapontuac¸ãonoquestionárioDASHfoideno mínimo32pontosenomáximo120pontos(médiade57)eaescaladeMEPSapresentou pontuac¸ãomínimade60pontosemáximade100pontos(médiade90pontos).
Conclusão: otratamentoartroscópicodaepicondilitelateral,além deseguro,apresenta resultadossatisfatórios.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Lateralepicondylitis,alsoknownas“tenniselbow”,isa condi-tioncommonlyfoundinmedicalpractice.Itaffectsbetween 1%and 3%ofthe populationand is mostfrequentamong individualsbetween35and50yearsofage.Althoughitwas originallythoughtthatthispathologicalconditionwasmostly associatedwiththeactofplayingtennis,theetiologyofthis pain in the lateral region of the elbow ismore related to overuseorrepetitivedorsiflexionandpronosupination exer-tion ofthe wrist. Thediagnosis ismade clinicallythrough identifyingitoccupationallyandfromphysicalexamination. Imagingexaminationsarerarelyneeded.1,2
Lateralepicondylitiswas firstdescribedbyRungeinthe German literaturein 1873. The association with the game of tennis was suggested by Morris ten years later, which led to the term “tennis elbow”, although it also occurs in otherracquetsportsandingolf.Sincethen,therehasbeen discussionregardingthecauses,pathogenesisand possible treatments.1–3
Thepathogenesisoflateralepicondylitisisstilla contro-versialmatter,butitisknownthatnotonlythetendonofthe extensorcarpiradialisbrevis(ECRB)musclebutalsothe annu-larligament,lateralcapsule,radialnerveandsomebandsof thetendonoftheextensordigitorumcommunismuscleare involved.2
It was originally thought that the cause of lateral epi-condylitiswasaninflammatoryprocess,whichwouldthen resultinthesymptoms. However,histologicalstudies have demonstrated that, through repetitive injuries at the site, thereisadegenerativeprocessandafailureofrepairinthe
ECRB tendon. Thisismorepronouncedthan inflammation in other structures. The normal tissue of the ECRB ten-donisinvadedbyimmaturefibroblastsandnon-functioning vascular buds,thereby characterizing what todayis called “angiofibroblasticdegeneration”,whichconsistsof fibroblas-ticandvascularresponsesthataremorecommonlyreferred toastendinosis.2–4
Thereisstillnoconsensusregardingthebestapproachto takeincasesoflateralepicondylitis.Althoughitisa patholog-icalconditionwitheminentlyconservativetreatment,some patientspresentsymptomsthatarerefractorytothis treat-ment.Inthesecases,surgicalinterventionmaybeindicated, and this can be done by means of either an open or an arthroscopic technique. Arthroscopic treatment for lateral epicondylitiswasdescribedrecentlyandpresentsthe advan-tagesofenablingtendondebridement withoutdividingthe aponeurosisoftheextensordigitorumcommunis,evaluation ofintra-articularpathologicalconditionsand,possibly, reha-bilitationwithinashorterperiod.5
Manystudieshavedemonstratedtheimmediatesuccess ofsurgicaltreatmentforlateral epicondylitis.However,few have demonstrated the long-termresults.3 Theaimof the
presentstudywastoreportthelong-termresultsfrom arthro-scopicsurgicaltreatmentinpatientswithlateralepicondylitis that was refractoryto conservative treatment, focusing on theimprovementofthestateofpainandfunctionalityofthe elbow.
Materials
and
methods
Theresearch project was approvedbythe Research Ethics Committee of the Paraná Culture Association (Associac¸ão ParanaensedeCultura,PUC-PR),bymeansoftheBrazil Plat-form,onMay22,2012(CAAE:01542912.6.0000.0020).
Twentypatientswithlateralepicondylitisthatwas refrac-torytoconservativetreatment,whoweretreatedbymeansof arthroscopicsurgerybetweenAugust2000andOctober2012, wereidentified.Ofthesepatients,16werelocatedtoarrange interviewsinanoutpatientclinicand14cametothe inter-views,totaling15elbows.
The inclusion criteria were that there needed to be a clinicaldiagnosisoflateralepicondylitis,positivesemiology and receipt of conservative treatment for a minimum of 18 months. Patients with neurovascular deficits, cognitive deficits or polyarthralgia, or who had undergone previous surgeryonthisjoint,wereexcluded.
The following data were gathered: sex, age, dominant limb, operated limb, profession, symptoms before surgery, dateofstartofsymptoms,previoustreatmentthathadbeen instituted, duration ofphysiotherapy, number of glucocor-ticoidinfiltrations, date ofthe surgery, complicationsfrom theprocedure,postoperativecomplaintsandrange-of-motion measurementsbeforeandafterthesurgery.
Thepatientswereclassifiedsurgicallyinaccordancewith thescale ofBakeret al.6 into lesionsoftypeI(intactjoint
capsule), typeII (linear/partialcapsule lesion) and typeIII (completecapsulelesion).Duringtheinterviews,thepatients wereaskedtoanswertheDASHquestionnaireandtheywere also assessed functionally bymeans of MEPS.7 They were
alsoaskedabouttheirdegreeofsatisfactionwiththe surgi-calresult,throughtheirresponsetobeingaskedwhetherthey wouldundergotheprocedureagain.
Theresults were analyzeddescriptively using the Excel softwaretoconstructtablesandgraphs.
Surgical
technique
Arthroscopywasperformedwiththepatientinventral decu-bitus, under intravenous and plexus anesthesia, with a tourniquetattherootofthelimb.Cefazolin(1g)was adminis-teredintravenouslytoinduceanesthesia.Firstly,theboneand nervestructuresoftheelbowwereidentifiedanddemarcated. Insufflationofthejointwasperformedbymeansofinjection of15mLofphysiologicalserum,andthen ananteromedial portalwasconstructedinorder toclosely inspectthejoint bymeansof30◦arthroscopy.Followingthis,theECRBtendon waslocated,whichmadeitpossibletoclassifythelesionin accordancewithBakeretal.6(Fig.1).Ananterolateralportal
wasconstructedunderdirectviewing,inordertoinsertthe arthroscopy instruments,while the proximal anteromedial portalwasusedtoinsertthecapsuleretractor.
Withthe aid ofa5mmshaver blade,the compromised tissue and the entire origin of the tendon were debrided. Theinsertionbedwasthenscarified(Fig.2).Afterafurther inspection of the joint, the portals were sutured using 3-0monofilament thread.The operatedlimb waspositioned flexedat80◦usingabag-typesling.
Afterthepatienthad recoveredfrom anesthesia, mobil-ity of the fingers and wrist were stimulated and the limb
Fig.1–Identificationoftheoriginoftheextensorcarpi radialisbrevis(ECRB).
remained immobilizedfor oneweek.Afterthis period, the stitches were removed and the specialized physiotherapy workwasstarted.
Results
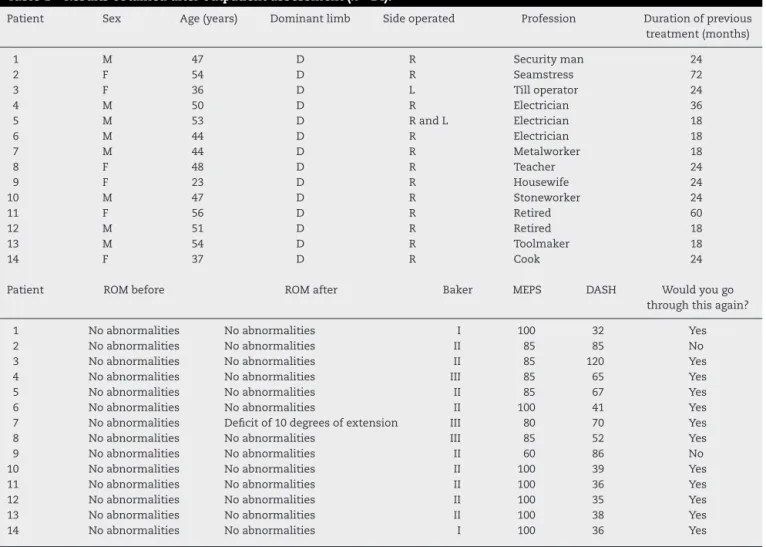
SomeofthedatagatheredarepresentedinTable1.
Thepatients’ agesrangedfrom 23 to56years (meanof 46).Therewereeightmalesandsixfemales.Amongthe15 elbows,12wereonthedominantlimb,onewasonthe non-dominant limband onepatient had bilateral injuries.The lengthoffollow-up afterthesurgerywasaminimumof24 monthsandamaximumof72months(mean:41).Themain symptomsreportedbythepatientsbeforethesurgerywere pain,edema,paresisandparesthesia.
Theassociatedcomorbiditiesincludedonecaseof tendini-tisinthewristflexors,onecaseofrotatorcuffinjuryandone caseofuseofantidepressants.
In our sample, all the patients had previously been treated conservatively for a minimum of 18 months and a maximum of 72 months (mean: 30). The treatments instituted had included: relativerest, modification todaily activities,acupuncture,administrationofnon-steroidal anti-inflammatorydrugs(NSAIDs),corticoidinjectionsand phys-iotherapy.Sixpatientshadundergonelocalinfiltration,with anaverageoftwoapplicationsperpatient.
Complicationswere observedin28.5%ofthe cases(one patientwithlocalalterationsofsensitivityintheregionofthe lateral portal,onewithadeficitof10degreesofextension, onewithasynovialplicaandonewithsynovitisinthelateral
Table1–Resultsobtainedafteroutpatientassessment(n=14).
Patient Sex Age(years) Dominantlimb Sideoperated Profession Durationofprevious treatment(months)
1 M 47 D R Securityman 24
2 F 54 D R Seamstress 72
3 F 36 D L Tilloperator 24
4 M 50 D R Electrician 36
5 M 53 D RandL Electrician 18
6 M 44 D R Electrician 18
7 M 44 D R Metalworker 18
8 F 48 D R Teacher 24
9 F 23 D R Housewife 24
10 M 47 D R Stoneworker 24
11 F 56 D R Retired 60
12 M 51 D R Retired 18
13 M 54 D R Toolmaker 18
14 F 37 D R Cook 24
Patient ROMbefore ROMafter Baker MEPS DASH Wouldyougo
throughthisagain?
1 Noabnormalities Noabnormalities I 100 32 Yes
2 Noabnormalities Noabnormalities II 85 85 No
3 Noabnormalities Noabnormalities II 85 120 Yes
4 Noabnormalities Noabnormalities III 85 65 Yes
5 Noabnormalities Noabnormalities II 85 67 Yes
6 Noabnormalities Noabnormalities II 100 41 Yes
7 Noabnormalities Deficitof10degreesofextension III 80 70 Yes
8 Noabnormalities Noabnormalities III 85 52 Yes
9 Noabnormalities Noabnormalities II 60 86 No
10 Noabnormalities Noabnormalities II 100 39 Yes
11 Noabnormalities Noabnormalities II 100 36 Yes
12 Noabnormalities Noabnormalities II 100 35 Yes
13 Noabnormalities Noabnormalities II 100 38 Yes
14 Noabnormalities Noabnormalities I 100 36 Yes
M,male;F,female;R,right;L,left;ROMbefore,rangeofmotionbeforeoperation;ROMafter,rangeofmotionafteroperation;MEPS,MayoElbow PerformanceScore;DASH,DisabilitiesoftheArm,ShoulderandHand.
compartment).Nocasesofinfectionorpersistentdrainageat theaccessportalswereobserved.
Regarding the postoperative complaints, only three patientsreportedhavinglocalpain.
AccordingtotheclassificationofBakeretal.,6therewere
twopatientswithtypeIlesions,ninewithtypeIIandthree withtypeIII.OurscoringfromtheDASHquestionnairewasa minimumof32pointsandamaximumof120points(mean: 57),andtheMEPSscoresrangedfromaminimumof60points toamaximumof100points(mean:90).
Discussion
Despite the advances already achieved in relation to the etiopathogenesis of lateral epicondylitis, there is still no consensus regarding its management.3 In most cases, the
symptoms of lateral epicondylitis are effectively resolved throughrest,modificationofphysicalactivities,useofNSAIDs andphysiotherapy.Newtypesoftreatmentinclude extracor-porealshockwaves,laserapplication,filament lighttherapy andinjectionsofplatelet-richplasma.1,2,8
Onlyafewcases(around8%)presentpainthatisrefractory totheabovementionedmeasures.Aftersixmonthsof inef-fectiveconservativetreatment,surgicalinterventionisthen
indicated.Thismaybeundertakenthroughanopen, percu-taneousorarthroscopicapproach.1,8Althoughsixmonthsof
conservativetreatmentisrecommendedintheliterature,we choseinourstudytomaintainthistreatmentforaminimum of18monthsbecauseofdifficultyinstartingandfollowingup physiotherapyinthehealthcaresystem.
Themajorityofthesurgicalproceduresfollowthesame principle,consistingofdebridementorreleaseoftheoriginof theECRBtendon.1,5Opensurgicalinterventionpresentsgood
results,butfailstoidentifyassociatedintra-articularlesions, whicharepresentin11–69%ofthepatients.9Moreover,open
surgerycarriesrisksofligamentinjuries,whichmayleadto elbowinstability.10
Thearthroscopictechniqueenablesgood viewingofthe elbowjointandthepathological conditionsthatmayexist. However,this technique takes along time to performand surgeonsrequiretrainingandexperienceinordertoachieve goodresults.Theprocedurepresentsresultsthataresimilarto thosefromconventionaltechniquesbut,asreportedby stud-iesinthisregard,thefailurerateislowerandanearlyreturn toactivitiesisenabled.8
InaccordancewiththesurgicalclassificationofBakeretal., itwasfoundthattwopatientshadtypeIlesions,ninehad typeIIlesionsandthreehadtypeIIIlesions.Inthepatient withbilaterallesions,bothofthemweretypeII.Thisshows thatpartialcapsule-tendonlesionswere themostfrequent occurrenceinoursample,whichwasprobablybecauseofthe activitiesperformedbyourpatients.Studieshaveindicated thatthereisnorelationshipbetweenthetypeoflesionand thepostoperativeclinical-functionalevolution.5,6Thistypeof
relationshipwasalsonotfoundinourresults.
InotherstudiesthatmadeevaluationsusingMEPSscores, theresultsweresimilartoours.Kimetal.4divided38patients
who underwent the procedure according to the technique used:19patientswhounderwentdebridementandreleaseof theECRBandanother19whoonlyunderwentrelease.Both groupspresentedameanof40pointsonMEPS.Thestudyby Bakeretal.6includedapopulationof40patients(42elbows)
whounderwentoperationsusingthetechniqueinquestion. Outofthistotal,37patients(39elbows)werefollowedup.Of these,13patientswhoreturnedforasubjectiveclinical exam-inationpresentedamean of93.6points. Inananalysison eightpatientswhounderwentarthroscopy,ZoppiFilhoetal.10
foundscoresgreaterthan90points.Ourscoresrangedfroma minimumof60pointstoamaximumof100points(meanof 90),whichcorroboratesthedataintheliteratureinrelationto satisfactoryfunctionalresults.
TheresultsfromtheDASHquestionnairefoundinthe liter-aturearepromising.Othman8divided33patientswithlateral
epicondylitisintotwogroups:onewith14patientswho under-wentarthroscopyandonewith19patientswhounderwenta percutaneoustechnique.ThescoresfromtheDASH question-nairewereevaluatedbeforeandaftersurgeryandtheresults werefoundtobesignificant(p<0.05).Inthefirstgroup,the scoreimprovedfrom72to48points,andinthesecond,from 70to50 points. Comparingthe postoperativescoresinthe twogroups,therewasnosignificantdifference(p=0.5002).In astudy on18patients whounderwent arthroscopic opera-tions,Wadaetal.12usedtheJapaneseHandSurgerySociety’s
version ofthe DASHquestionnaire.From analysis ontheir results,theseauthorsobservedthatthereweretwofactors relatingtoworseresultsfromthequestionnaire.Thefirstwas lowT2signalattheoriginoftheECRBonpreoperative mag-neticresonanceimaging,andthesecondwasreceiptofpublic assistance.Our patients presentedaminimum scoreof32 pointsandamaximumof120points(mean:57),whichwas alsosimilartotheresultsfromotherstudies.
According to the studies reviewed, most patients who underwent theprocedure declared thatthey were satisfied withtheresultsfromthesurgery.BakerandBakerfoundthat 28(93%)oftheir30patientssaidthattheywouldundergothe surgeryagain.3Inapostoperativeanalysison20patientswith
ameanfollow-upof20months,Miyazakietal.9foundthat
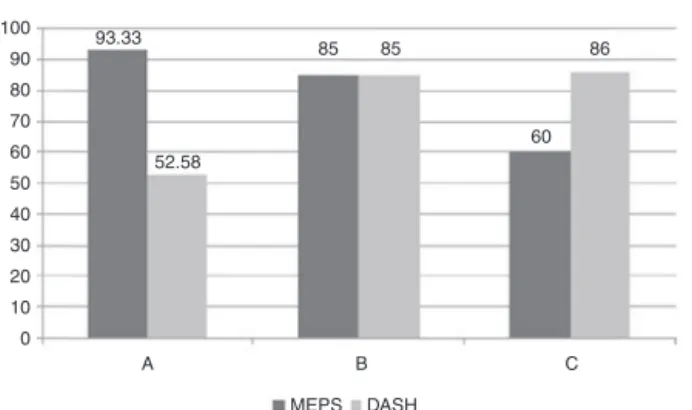
100 52.58 85 93.33 6 8 5 8 60 90 80 70 60 50 40 30 20 10 0
A B C
MEPS DASH
Fig.3–ScoringforpatientsontheMEPSandDASHscales accordingtotheirresponsesrelatingtowhethertheywould gothroughthisoperationagain.(A)Meannumberof patientswhoanswered“yes”;(B)and(C),scoresofthetwo patientswhoanswered“no”.MEPS,MayoElbow
PerformanceScore;DASH,DisabilitiesoftheArm,Shoulder andHand.
onlyonepatientwasdissatisfied withtheresults,and this wasbecausethepatientpresentedreflexsympathetic dystro-phyasasurgicalcomplication.Withameanfollow-upof14 months,ZoppiFilhoet al.10 foundthattheireightpatients
weresatisfiedwiththeresults.Lattermanetal.5reportedthat,
outof32patientswithameanfollow-upof3.5years,20(63%) wouldundergothesurgeryagain.Thesedatashowthatthe technique usedpresentedsatisfactory clinicresultsforthe patients,particularlyregardingpaincontrol.
Ourstudy,inagreementwiththosereviewed,alsofound thatthemajorityoftheresponseswerepositivewithregard to satisfaction.Twelve patients (85%)said that they would undergotheprocedureagainandonlytwo(15%)responded negatively.However,thefunctionalevaluationscoresofthese patientsafterthesurgerydidnotjustifytheirdissatisfaction and,thus,noexplanationcouldbefoundfortheirresponses onthebasisoftheresultsfromtheprocedure(Fig.3).
The possiblecomplicationsafter the procedure are rare andconsistofneurovascularlesions,posterolateralligament lesions, hematomas and infection of the surgical wound.8
Moststudies havenotreported anycomplications.6,9,10,12,13
Inananalysison18patientsoperatedusingthistechnique, Cumins14 also did not report any complications, but this
author’shistologicalanalysisshowedmicroscopicfindingsof residualtendinopathyintenpatients.Lattermanetal.5had
onepatientwhopresentedparesthesiaintheforearmfortwo weeksafterthesurgery,withspontaneousresolution.Inour sample,wefoundacomplicationrateof28.5%(onepatient withlocalalterationsofsensitivityintheregionofthe lat-eralportal,onewithadeficitof10degreesofextension,one withasynovialplicaandonewithsynovitisinthelateral com-partment).Nonetheless,theprocedurewasshowntohavelow morbidityratesifperformedbyatrainedprofessional.
Lattermanetal.5consideredthatthetechniquepresented
etal.6demonstratedthatonly10%oftheirpatientspresented
painduringtheirdailyactivities.Cummins14madea
compari-sonbetweenpreandpostoperativepainamongtheirpatients, bymeansofsomepaincategories.Amongtheir18patients, onlytwodidnotpresentapostoperativeimprovementofpain, andthiswasrelatedonlytothecategoryof“worstpainlevel”. Thisauthorconcludedthatthis resultoccurredinpatients who presented residual microscopic disease. All the eight patientsinthestudybyZoppiFilhoetal.10evolvedwithout
painandwithout anylimitationofrangeofmotion.Inour sample,onlythreepatientsreportedhavinglocalpain.
Conclusion
Weconcludethatarthroscopictreatmentoflateral epicondyli-tis presents low morbidity, whichmakes it safe, and good resolutioncapacity,whichenablesimprovementofthestate ofpainandfunctionalityoftheelbow.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. JohnsonGW,CadwalladerK,ScheffelSB,EpperlyTD. Treatmentoflateralepicondylitis.AmFamPhysician. 2007;76(6):843–8.
2. SavoieFH,VanSiceW,O’BrienMJ.Arthroscopictenniselbow release.JShoulderElbowSurg.2010;19(2):31–6.
3. BakerCL,Baker3rdCL.Long-termfollow-upofarthroscopic treatmentoflateralepicondylitis.AmJSportsMed. 2008;36(2):254–60.
4.KimJW,ChunCH,ShimDM,KimTK,KweonSH,KangHJ, etal.Arthroscopictreatmentoflateralepiconsylitis: comparisonoftheoutcomeofECRBreleasewithanwithout decortication.KneeSurgSportsTraumatolArthrosc. 2011;19(7):1178–83.
5.LattermannC,RomeoAA,AnbariA,MeiningerK,McCartyLP, ColeBJ,etal.Arthroscopicdebridementoftheextensorcarpi radialisbrevisforrecalcitrantlateralepicondylitis.JShoulder ElbowSurg.2010;19(5):651–6.
6.BakerJrCL,MurphyKP,GattlobCA,CurdDT.Arthroscopic classificationandtreatmentoflateralepicondylitis:two-year clinicalresults.JShoulderElbowSurg.2000;9(6):
475–82.
7.MorreyBF,AnKN,ChaoEYS.Functionalevaluationofthe elbow.In:MorreyBF,editor.Theelbowanditsdisorders.2nd ed.Philadelphia:Saunders;1993.p.86–9.
8.OthmanAM.Arthroscopicversuspercutaneousreleaseof commonextensororiginfortreatmentofchronictennis elbow.ArchOrthopTraumaSurg.2011;131(3):383–8.
9.MiyazakiAN,FregonezeM,SantosPD,daSilvaLA,PiresDC, MotaNetoJ,etal.Avaliac¸ãodosresultadosdotratamento artroscópicodaepicondilitelateral.RevBrasOrtop. 2010;45(2):136–40.
10.ZoppiFilhoA,VieiraLAG,FerreiraNetoAA,BenegasE. Tratamentoartroscópicodaepicondilitelateraldocotovelo. RevBrasOrtop.2004;39(3):93–101.
11.YeohKM,KingGJW,FaberKJ,GlazebrookMA,AthwalGS. Evidence-basedindicationsforelbowarthroscopy. Arthroscopy.2012;28(2):272–82.
12.WadaT,MoriyaT,IbaK,OzasaY,SonodaT,AokiM,etal. Functionaloutcomesafterarthroscopictreatmentoflateral epicondylitis.JOrthopSci.2009;14(2):167–74.
13.OwensBD,MurphyKP,KukloTR.Arthroscopicreleasefor lateralepicondylitis.Arthroscopy.2001;17(6):
582–7.