w w w . r b o . o r g . b r
Original
Article
Result
from
surgical
treatment
on
the
terrible
triad
of
the
elbow
夽
Anderson
de
Aquino
Santos
∗,
Thomaz
Antônio
Tonelli,
Fabio
Teruo
Matsunaga,
Marcelo
Hide
Matsumoto,
Nicola
Archetti
Netto,
Marcel
Jun
Sugawara
Tamaoki
EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30July2014 Accepted7August2014 Availableonline3July2015
Keywords:
Elbow Fracture Dislocation Orthopedicsurgery
a
b
s
t
r
a
c
t
Objective:Toevaluatetheresultsfromsurgicaltreatmentoftheterribletriadoftheelbow, withaminimumofsixmonthsoffollow-up,takingelbowfunctionintoconsideration.
Methods:Theanalyzedaspectsof20patients,whounderwentsurgicaltreatmentofthe terri-bletriadoftheelbow,weregivenasfollows:Dashscore(DisabilitiesoftheArm,Shoulderand Hand),Meps(MayoElbowPerformanceScore),painaccordingtoVAS(visualanalogscale), ROM(rangeofmotion),patientsatisfaction,degreeofenergyofthetrauma,complications andradiographs.
Results:Themeanlengthoffollow-upamongthepatientswas38months.Therewere statis-ticallysignificantrelationshipsbetweenthefollowingsetofparameters:traumamechanism andpatientsatisfaction;radiologicaloutcomeof“heterotopicossification”andsatisfaction; functionalflexion–extensionROMandsatisfaction;andbetweentypeofradialheadfracture andpresenceofaradiologicaloutcome.
Conclusion: Thesurgicaltreatmentfortheterribletriadoftheelbowgenerallyprovided sat-isfactoryresults,whenthefunctioningofthisjointuponthereturntoactivitieswastaken intoconsideration.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Resultado
do
tratamento
cirúrgico
da
tríade
terrível
do
cotovelo
Palavras-chave:
Cotovelo Fratura Luxac¸ão
Cirurgiaortopédica
r
e
s
u
m
o
Objetivo:Avaliarosresultadosdotratamentocirúrgicodatríadeterríveldocotovelo,com nomínimoseismesesdeseguimento,considerandoafunc¸ãodocotovelo.
Métodos:Foramanalisadososseguintesaspectosde20pacientessubmetidosatratamento cirúrgicoportríadeterríveldocotovelo:escoresDash(DisabilitiesoftheArm,Shoulderand Hand),Meps(MayoElbowPerformanceScore),dorpelaEVA(EscalaVisualAnalógica),ADM (arcodemovimento),satisfac¸ãodopaciente,graudeenergiadotrauma,complicac¸õese radiografias.
夽
WorkdevelopedintheDisciplineofHandandUpper-limbSurgery,DepartmentofOrthopedicsandTraumatology,EscolaPaulistade Medicina,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.d.A.Santos). http://dx.doi.org/10.1016/j.rboe.2015.06.010
Conclusão: Otratamentocirúrgicodatríadeterríveldocotoveloproporcionou,deforma geral,resultadossatisfatórios,quandoseconsideraafunc¸ãodessaarticulac¸ãonoretorno àsatividades.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Traumatic lesions in adult elbows can be very challeng-ing to treat due to their complex anatomy and potential complications.1
Hotchkiss1describedanassociationpatternoflesionsin
thisjoint,the terribletriadoftheelbow, whichconsistsof posteriordislocationoftheelbowassociatedwithacoronoid fractureandwitharadialheadfracture,whichpresentsgreat potentialforjointinstability.Itisthusnamedduetoits unfa-vorableprognosis.
Theterribletriadisrareandgenerallyoccursinyoungmale patients,relatedtohigh-energytrauma.Themostcommon mechanismconsists offallingonto the outstretchedhand, withtheelbowunderhyperextension,supinationandvalgus stress.2
The treatment for these lesions is eminently surgical becauseconservativetreatmentisriskyandrelatedto vari-ouscomplications.3Thelattertreatmentisconsideredtobe
theexception,indicatedinwell-selectedcasesinwhichthere isgoodalignmentoftheelbow,withoutarticularblock,and inwhichthecoronoidandradialheadfracturesarerelatively smallandonlyslightlydeviated.4
Surgical treatment has the objectives of restoring joint stabilityandachievinganatomicalreductionandearly mobil-ityduringthe postoperativeperiod.Thisallowsrestoration of functional capacity and, therefore, reduces the risk of complications.5
Duetotheseriousnessandrarityofthelesion,few stud-ieshaveevaluatedtheresultsfromsurgicaltreatmentofthe terribletriadoftheelbow.6,7Itsprognosisremainsuncertain,
especiallyoverthelongterm.6
Theobjective ofthe present study was to evaluatethe resultsfrom surgical treatment ofthe terrible triad ofthe elbow, with at least six months of follow-up, considering thefunctionoftheelbow.
Material
and
methods
Patientswithterribletriadoftheelbowwhoweretreated sur-gicallybetween 1999and 2012, atthe Shoulderand Elbow SectoroftheDisciplineofHandand Upper-limbSurgeryof ourservice,wereretrospectivelyevaluated.
All patients older than 18 years who agreed to partici-pateinthestudyandsignedthefreeandinformedconsent statementwereincluded.Thestatementhadpreviouslybeen
acceptedbytheResearchEthicsCommitteeunderthenumber CEP0032/11.
Theexclusioncriteriacomprisedassociatedlesionsor dis-easesthatcouldinterfereintheevaluationoftheoutcomes, lack ofinformationin the medicalrecords dueto absence or non-comprehension and failure to return for reevalua-tion.
Thefollowingepidemiologicalinformationwasobtained: age, ageonthe dateofthe trauma,sex,dominance,elbow affected,traumamechanism,associatedlesions,surgery per-formed, duration of immobilization, complications during treatment,patient’sdegreeofsatisfactionanddatafromthe lastconsultation.
TheprimaryoutcomeusedwastheDASHscore,8as
vali-datedforthePortugueselanguage.
ThesecondaryclinicalfunctionaloutcomewastheMayo ElbowPerformanceScore(MEPS).9Inaddition,painwas
eval-uated using avisualanalog scale(VAS)10 and the patients’
rangeofmotion(ROM)wasanalyzeddichotomously, consid-ering the functional ROM according to Morrey (30–130◦ of flexion–extensionoftheelbowand50–50◦ ofpronationand supination).9
Complications were recorded accordingtotheir severity andthedateofoccurrence;forinstance:infection,renewed dislocationandreoperation.
Lesionswereevaluatedradiographicallyandclassifiedas follows:
- Radialheadfracture,withdescriptionofthetypeof frac-tureaccordingtoMason.Classified11,12 accordingtotheir
severityanddividedintotypeI:fractureswithoutdeviation,
typeII:fractureswithdeviation,andtypeIII:comminuted
fractures.
- Coronoidprocessfracture.Classifiedaccordingtothe sys-temdescribedbyReganandMorrey13anddividedintotype
I:apexavulsion,typeII:impairmentofupto50%ofitsheight
andtypeIII:involvingover50%ofitsheight.
Inaddition, postoperativeradiographswere producedin frontal and lateral views and the following characteristics were evaluated: presenceofosteoarthritis,presence of lig-ament calcification, pseudarthrosis, skewed consolidation (malunion)andheterotopicossification.Theresponseswere dichotomous.
Fig.1–Frontandlateral-viewradiographsoftheelbowdemonstratingtheresultsfromthesurgicaltreatment,withlateral ligamentrepairusingananchor,radialheadprosthesisandosteosynthesisofthecoronoidusingascrew.
For the statistical analysis, the test of equality of two proportions was used in order to characterize the relative frequencies of sex, trauma mechanism, dominance, MEPS classificationandcomplications.
Thechi-squaretestwasusedforcomparingthequalitative variableswiththeMEPSclassification.
TheMann–Whitneytestwasusedforcomparingvariables relatingtothetypeoffracture,suchastraumamechanism, classificationoftheradialheadfractureandclassificationof thecoronoidfracture,andvariablesrelatingtoradiographic complicationssuchasosteoarthrosis,ligamentcalcification, heterotopic ossification and malunion, with the factors of functionalrangeofmotion,elbowfunction,painand satis-faction.
Lastly,theSpearmancorrelationwasusedformeasuring thedegreeofrelationshipbetweenthedurationof immobi-lizationandthefindingsfromthephysicalexaminationand questionnaires.
Thefollowingsoftwarewasusedforperformingthe statis-ticalanalysis:SPSSV17,Minitab16andExcelOffice2010.
All the patients included underwent the same surgical procedure protocol.Afteradministrationofbrachial plexus block in association with general anesthesia, the patients wereplacedinthehorizontaldorsaldecubituspositionand asepsiswasperformedusingchlorhexideneandalcohol.The procedure always began through the lateral access route describedbyKocher,betweentheextensorcarpiulnarisand the anconeus muscles. The radial head fracture was first dealt.In cases ofan indication ofarthroplasty, the condi-tionofthe coronoidprocesswasverifiedthroughthesame accessrouteandthefracturewasdealtwithwhenever possi-ble.Inallcases,thelateralulnarcollateralligamentwasalso repaired.Inpatientstreatedwithosteosynthesisoftheradial headandincasesofpersistenceofelbowinstability,an addi-tionalmedialaccessroutewascreated inorder toperform osteosynthesisofthecoronoidorrepairoftheanteriorcapsule and,whennecessary,repairorreconstructionofthemedial
collateralligament.Afterrepairingallthesestructures,ifthere wasanyremaininginstability,adynamicexternalfixatorwas used(Fig.1).
Duringthepostoperativeperiod,thepatientsunderwent thesamerehabilitationprotocolandwereencouragedtodo earlyassistedexercisesinaccordancewiththeirtoleranceof pain,inordertoavoidelbowstiffnessduetojoint immobiliza-tion.
Results
Thisstudypresentedaninitialsampleof20cases,fromwhich three were excluded due to lack ofessential data in their recordsandtwoabandonedthefollow-upbeforethe conclu-sion ofthe study.Thus,15 patients remained forthe final analysis.Theepidemiologicalcharacteristics,theclinicaldata ofthesample,the radiologicaloutcome andthefunctional outcome were reported through the observed DASH score, MEPS,VASandpatient’ssatisfaction,asdescribedinTable1.
The cases evaluated presented a mean time interval betweentraumaandsurgeryof7±2.6daysandmeanlength offollow-upof38.6±23.3months.Themeanofdurationof immobilizationwas2.8±0.8weeks.
The analysis on the range of motion of elbow flexion–extension during the postoperative period revealed that10 cases(66.7%)presentedaROMthatwasconsidered functional, while the remaining five (33.3%) presented a non-functionalelbowfromthisperspective.Theanalysison pronosupination of the forearm revealed that 12 patients (80%)presentedacceptablefunction.
Female(%) 10(66.7)
Meanage(SD) 43.8(13.4)
Dominance–leftupperlimb(%) 1(6.7)
Dominance–rightupperlimb(%) 14(93.3)
Characteristicsofthefracture
Sideaffected–left(%) 9(60)
Sideaffected–right(%) 6(40)
High-energytrauma(%) 7(46.7)
Low-energytrauma(%) 8(53.3)
Radialheadfracturen(%)
Type1 0(0)
Type2 5(33.3)
Type3 10(66.7)
Coronoidfracturen(%)
Type1 10(66.7)
Type2 2(13.3)
Type3 3(20)
Functionaloutcomes Mean(SD)
DASH 28.7(13.7)
MEPS 84.7(16.7)
VAS 2.0(2.3)
MEPS n(%)
Excellent 8(53.3%)
Good 3(20%)
Fair 3(20%)
Poor 1(6.7%)
Satisfaction n(%)
Yes 12(80)
No 3(20)
Radiologicaloutcomes n(%)
Ligamentcalcification 7(46.7)
Malunion 2(13.3)
Heterotopicossification 3(20)
Osteoarthritis 5(33.3)
Pseudarthrosis 1(6.7)
SD,standarddeviation;n,number;DASH,DisabilitiesoftheArm, ShoulderandHand;MEPS,MayoElbowPerformanceScore;VAS, visualanalogscale.
experiencedhigh-energytrauma.Therewerealsocorrelations betweentheradiologicaloutcomeof“heterotopicossification” and satisfaction and between functional flexion–extension ROMand satisfaction (Table 2).In addition, therewas also atendency towardanassociation betweenthe radiological outcomeof“heterotopicossification” andthevisualanalog scale(Table3).
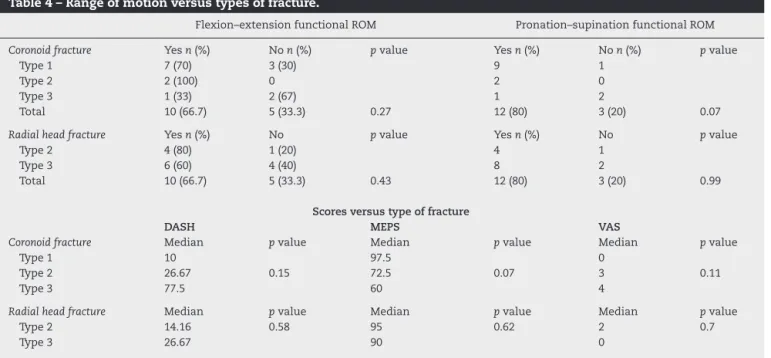
Fromcorrelatingthetypesoffracturewiththefunctional outcomesdeterminedbyscoresandwiththefunctionalrange ofmovement,tendenciestowardanassociationbetweenthe typeofcoronoidfractureandfunctionalROMof pronosupina-tionandbetweenthetypeofcoronoidfractureandtheMEPS scorewereobserved(Table4).
When the data regarding the classification of fractures werecorrelatedwiththepresenceofaradiologicaloutcome,a significantassociationwasobservedforthetypeofradialhead
fracture(Table5). Table
Table3–Radiologicaloutcomesversusscores.
DASH MEPS VAS
Osteoarthritis Median pvalue Median pvalue Median pvalue
Yes 26.67 85 2
No 15 0.4 95 0.45 1 0.6
Ligamentcalcification Median pvalue Median pvalue Median pvalue
Yes 26.67 85 2
No 15 0.64 97 0.4 1 0.62
Malunion Median pvalue Median pvalue Median pvalue
Yes 47.1 77.5 3
No 20 0.31 95 0.43 0 0.27
Heterotopiccalcification Median pvalue Median pvalue Median pvalue
Yes 35.22 60 4
No 21.97 0.11 95 0.14 0 0.07
ROM,rangeofmotion;n,number;DASH,DisabilitiesoftheArm,ShoulderandHand;MEPS,MayoElbowPerformanceScore;VAS,visualanalog scale.
Table4–Rangeofmotionversustypesoffracture.
Flexion–extensionfunctionalROM Pronation–supinationfunctionalROM
Coronoidfracture Yesn(%) Non(%) pvalue Yesn(%) Non(%) pvalue
Type1 7(70) 3(30) 9 1
Type2 2(100) 0 2 0
Type3 1(33) 2(67) 1 2
Total 10(66.7) 5(33.3) 0.27 12(80) 3(20) 0.07
Radialheadfracture Yesn(%) No pvalue Yesn(%) No pvalue
Type2 4(80) 1(20) 4 1
Type3 6(60) 4(40) 8 2
Total 10(66.7) 5(33.3) 0.43 12(80) 3(20) 0.99
Scoresversustypeoffracture
DASH MEPS VAS
Coronoidfracture Median pvalue Median pvalue Median pvalue
Type1 10 97.5 0
Type2 26.67 0.15 72.5 0.07 3 0.11
Type3 77.5 60 4
Radialheadfracture Median pvalue Median pvalue Median pvalue
Type2 14.16 0.58 95 0.62 2 0.7
Type3 26.67 90 0
ROM,rangeofmotion;n,number;DASH,DisabilitiesoftheArm,ShoulderandHand;MEPS,MayoElbowPerformanceScore;VAS,visualanalog scale.
Discussion
The terrible triad of the elbow is characterized by great potentialforjointinstabilityandanunfavorableprognosis.1,5
Surgicaltreatmentisthetherapyofchoiceinthevastmajority ofcases,withtheaimsofrestorationoftheanatomyandearly mobility.Thisobjectiveremainsachallengeforsurgeonsdue tothecomplexityofthelesion.5
Inmost casesin the present study, the lesion wasdue tolow-energytrauma.Consideringtheradialheadfractures, type3oftheMasonclassificationwasthemostcommonone. Consideringthecoronoidfractures,thedistributionwas
het-erogeneous.Type1oftheRegan-Morreyclassificationwasthe onemostobserved.Thesedatacorroboratedtheepidemiology describedintheliterature.6,14
Unlikesomestudies,14,15thesampleofthepresentstudy
presented greater prevalence of the female sex (66.7%), which can be explained by population aging and by the predominanceofwomeninthisagegroup.Therewasalso pre-dominanceofthenon-dominantsideasthesidemostaffected (53.3%),i.e.theleftlimb.
Type1 4 6
Type2 2 0 0.08
Type3 0 3
Radialheadfracture No Yes pvalue
Type2 4 1 0.02
Type3 2 8
ofmotionofpronosupination.Thus,themajorityofthe sam-plepresentedafunctionalelbowjointfordailyactivitiesafter surgery,whichwas concordantwiththe resultsfrom other studiesthatevaluatedrangeofmotion.7,15,16
Althoughonestudy16didnotobtaingoodfunctionalresults
through the Bruce score,16 the results from the present
studyshowedgoodfunctionalresults.Thisdifferencecanbe explainedbythescoreused,sinceothervalidatedscoreswere usedinthepresentstudy.
Asexpected,relationshipsbetweensatisfactionandrange ofmotionofflexion–extensionandbetweensatisfactionand thetraumamechanismwereobserved.Thiswasbecauseall thepatientswhostatedthattheywerenotsatisfiedpresented anon-functionalrangeofmotionandhadbeeninvolvedin eventswithahigh-energytraumamechanism.
In addition, satisfaction presented a great association with the presence ofheterotopic ossification in the radio-graphicevaluation.Thosewhodidnotpresentsuchoutcomes reportedbeingsatisfied. Thesecorrelationsallowthe infer-encethatthesevariablesareprognosticfactorsforevaluation ofthesatisfactionofpatientswithsurgicaltreatment.
The severity of the coronoid fracture, as determined throughitsclassification,isanotherfactorthatcananticipate the prognosis in relationto the clinical result. In compar-ing this variable with the MEPS score, a tendency toward anassociation was observed, inwhich fractures ofgreater severity obtained scores that were considered worse. The samehappenedwhenthisvariable wascorrelated withthe functionof the elbow,measured through pronosupination. Thisimportanceofthetypeofcoronoidfracturewasobserved byGomideetal.15Ontheotherhand,theradialheadfracture
didnotpresentanysimilarassociation,fromthispointofview. However,themajorityoftheradialheadfracturesthatwere considered tobeofgreater severity presentedatleast one radiographicoutcome,whichdenotesthattheseverityofthis fractureisariskfactorforthepresenceofsometypeof radio-logicaloutcome.Incontrast,nosuchrelationshipwasfound whenthecoronoidfracturewasconsidered.
Duetotherarityofthelesion6,7andthedifficultyof
follow-ingupoursurgicallytreatedpatients,thesampleevaluated presentedasmallnumber ofcases, whichmayhave influ-encedthefinalresultsfoundinthepresentstudy.
Conclusion
Despite the limitation of the range of motion and a cer-tain degree ofresidual pain, the surgical treatment ofthe
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HotchkissRN.Fracturesanddislocationsoftheelbow.In: RockwoodCA,GreenDP,BucholzRW,HeckmanJD,editors. RockwoodandGreen’sfracturesinadults.4thed. Philadelphia:Lippincott-Raven;1996.p.929–1024. 2.Rodriguez-MartinJ,Pretell-MazziniJ,Andres-EstebanEM,
Larrainzar-GarijoR.Outcomesafterterribletriadsofthe elbowtreatedwiththecurrentsurgicalprotocols:areview. IntOrthop.2011;35(6):851–60.
3.ChanK,MacDermidJC,FaberKJ,KingGJ,AthwalGS.Canwe treatselectterribletriadinjuriesnonoperatively?ClinOrthop RelatRes.2014;472(7):2092–9.
4.GuittonTG,RingD.Nonsurgicallytreatedterribletriad injuriesoftheelbow:reportoffourcases.JHandSurgAm. 2010;35(3):464–7.
5.MathewPK,AthwalGS,KingGJ.Terribletriadinjuryofthe elbow:currentconcepts.JAmAcadOrthopSurg.
2009;17(3):137–51.
6.SeijasR,Ares-RodriguezO,OrellanaA,AlbaredaD,ColladoD, LlusaM.Terribletriadoftheelbow.JOrthopSurg(Hong Kong).2009;17(3):335–9.
7.WangYX,HuangLX,MaSH.Surgicaltreatmentof“terrible triadoftheelbow”:techniqueandoutcome.OrthopSurg. 2010;2(2):141–8.
8.OrfaleAG,AraújoPM,FerrazMB,NataourJ.Translationinto BrazilianPortuguese,culturaladaptation,andevaluationof thereliabilityoftheDisabilitiesoftheArm,Shoulderand HandQuestionnaire.BrazJMedBiolRes.2005;38(2): 293–302.
9.MorreyBF,AnKN,ChaoEYS.Functionalevaluationofthe elbow.In:MorreyBF,editor.Theelbowanditsdisorders.2nd ed.Philadelphia:Saunders;1993.p.86–9.
10.SummersS.Evidence-basedpracticepart2:reliabilityand validityofselectedacutepaininstruments.JPerianesthNurs. 2001;16(1):35–40.
11.MasonML.Someobservationsonfracturesostheheadofthe radiuswithareviewofonehundredcases.BrJSurg. 1954;42(172):123–32.
12.JohnstonGW.Afollow-upof100casesoffractureofthehead oftheradiuswithreviewoftheliterature.UlsterMedJ. 1962;31:51–6.
13.ReganW,MorreyB.Fracturesofthecoronoidprocessofthe ulna.JBoneJointSurgAm.1989;71(9):1348–54.
14.RingD,JupiterJB,ZilberfarbJ.Posteriordislocationofthe elbowwithfracturesoftheradialheadandcoronoid.JBone JointSurgAm.2002;84(4):547–51.
15.GomideLC,CamposDO,SáJMR,SousaMRP,CarmoTC, AndradaFB.Tríadeterríveldocotovelo:avaliac¸ãodo tratamentocirúrgico.RevBrasOrtop.2011;46(4): 374–9.