www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Investigation
of
neutrophil-to-lymphocyte
ratio
and
mean
platelet
volume
in
sudden
hearing
loss
夽
,
夽夽
Rauf
O˘
guzhan
Kum
a,∗,
Muge
Ozcan
a,
Deniz
Baklaci
a,
Nurcan
Yurtsever
Kum
a,
Yavuz
Fuat
Yilmaz
a,
Adnan
Unal
b,
Yonca
Avci
aaAnkaraNumuneEducationandResearchHospitalENTClinic,Ankara,Turkey bDepartmentofOtorhinolaryngology,HititUniversity,C¸orum,Turkey
Received18June2014;accepted8October2014 Availableonline7September2015
KEYWORDS
Hearingloss, sensorineural; Hearingloss,sudden; Neutrophils;
Plateletcount; Biologicalmarkers; Lymphocytecount
Abstract
Introduction:Severaltheoriesattempttoexplainthepathophysiologyofsuddenhearingloss. Objective:Theobjectiveofthisstudywastoinvestigatethepossibleroleofinflammationand atherothrombosisinsuddenhearinglosspatientsthroughtheneutrophil-to-lymphocyteratio andmeanplateletvolume.
Methods:Studydesign ---retrospectivecross-sectional historicalcohort.Thisstudy was con-ductedontwogroups:onewith59individualsdiagnosedwithsuddenhearingloss,andother with 59 healthy individuals with the same characteristics of gender and age distribution, neutrophil-to-lymphocyteratio andmeanplatelet volumelevels weremeasured inpatients diagnosedwithsuddenhearinglossaswellasinthecontrolgroup,anditwasverifiedwhether theseresultsinterferedforabetterorworseprognosiswithtreatmentofsuddendeafness. Results:Neutrophil-to-lymphocyte ratio levels are much higher inpatients diagnosed with suddenhearing losscomparedto thecontrolgroup.Similarly, meanlevelsof neutrophil-to-lymphocyteratioarehigherinnon-recoveredversusrecoveredpatients(p=0.001).However, wecouldnotfindacorrelationwithmeanplateletvolumelevels(p>0.05).
Conclusion:Neutrophil-to-lymphocyteratioisaquickandreliableindicatorregarding diagno-sisandprognosis ofsudden hearing loss;ontheotherhand, meanplatelet volumemay be consideredalessimportantindicatorinthisaspect.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:KumRO,ÖzcanM,BaklacıD,KumNY,YılmazYF,UnalA,etal.Investigationofneutrophil-to-lymphocyteratio andmeanplateletvolumeinsuddenhearingloss.BrazJOtorhinolaryngol.2015;81:636---41.
夽夽Institution:AnkaraNumuneEducationandResearchHospitalENTClinic,Ankara,Turkey.
∗Correspondingauthor.
E-mail:[email protected](R.O.Kum). http://dx.doi.org/10.1016/j.bjorl.2015.08.009
PALAVRAS-CHAVE
Perdaauditiva neurossensorial; Perdaauditivasúbita; Neutrófilos;
Plaquetas; Marcadores biológicos; Linfócitos
Investigac¸ãodarelac¸ãoneutrófilos/linfócitosevolumemédiodeplaquetasnasurdez súbita
Resumo
Introduc¸ão: Váriasteoriastentamexplicarafisiopatologiadasurdezsúbita(SS).
Objetivo: :Oobjetivodesteestudofoiinvestigaropossívelpapeldainflamac¸ãoeda aterotrom-bosenospacientesdeSSatravésdarelac¸ãoneutrófilos/linfócitos(RNL)evolumeplaquetário médio(VPM).
Método: Formadeestudo---coortehistóricacomcortetransversal(retrospectivo).Esteestudo foirealizadocom59indivíduosportadoresdeSSe59saudáveis,comasmesmas característi-casemdistribuic¸ãodegêneroeidade.OsníveisdeVPMeRNLforammedidosnospacientes diagnosticadoscomSSenogrupocontrole,verificando-sesetaisresultadosimplicavamemum melhoroupiorprognósticocomotratamentodasurdezsúbita.
Resultados: OsníveisdaRNLsãomuitomaisaltosempacientescomSS,emcomparac¸ãocom ogrupocontrole.Deformasemelhante,níveismédiosdaRNLsãomaisaltosnospacientesnão recuperados,emcomparac¸ãocomosrecuperados(p=0,001).Essasdiferenc¸asentretanto,não foramobservadasemrelac¸ãoaosníveisdeVPM(p>0,05).
Conclusão:RNLéumindicadorrápidoeconfiávelnoquedizrespeitoaodiagnósticoe prognós-ticodeSS;poroutrolado,VPMpodeserumindicadormenosimportantenesteaspecto. ©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Sudden hearing loss (SHL)is a disease characterized by a lossofhearinggreater than30dB inthreecontiguous fre-quenciesthatoccursinlessthanthreedays.1Theincidence
ofSHLrangesfrom5to20casesper100,000individuals.2,3
SincethephysiopathologyofSHLisstillunclear,thereare many theories as to the origin of this disease, including bacterial, viral and protozoal infections, blood disorders, vascular occlusion,immunedisorders,ototoxicdrugs, and metabolicconditions.3---7
Thecochleaisverysusceptibletoanyalterationof blood-stream.Vasculardiseasesandplateletalterationsmaycause somecochlearinjuriesandberelatedtoSHL.8
Platelets secrete and express a large number of substancesthatarecrucialmediatorsofcoagulation, inflam-mation, thrombosis, and atherosclerosis.9 The size and
functional activity of circulating platelets vary. Larger platelets are often younger, more reactive, and produce more thrombogenic factors.Mean plateletvolume (MPV), which is an indicator of platelet activation, is also used asamarkerof atherothrombosis,10 and maybean
impor-tant prophylactic and diagnostic tool in thrombotic and prothromboticcases.
White blood cell (WBC) count is auseful inflammatory biomarker in clinical practice. Even if the WBC is within a normal range, subtypes of WBC, such as neutrophil-to-lymphocyte ratio (NLR), may predict cardiovascular mortality.11,12 NLR is an easily measurable laboratory
markerthatisusedtoevaluatesystemicinflammationand it has also superiority compared to other WBC subtype counts (e.g.,neutrophil, lymphocyte,andtotal leukocyte counts). This superiority may be due to the stability of NLR compared to the other WBC subtype counts, which couldbeaffectedbyvariouspathologicalandphysiological
conditions.As thesefactors can alter the individual WBC subtype counts, NLR may remain more stable. Moreover, NLR may represent both inflammatory and immune path-ways that exist together in the patients. NLR has been defined as a novel and potential marker to determine inflammationincardiacandnon-cardiacdisorders.11,13---18
Recently, the relationship between MPV and NLR with SHLwere investigatedindividually.15,19---21 However,tothe
authors’knowledge, thisis the firststudy evaluatingMPV andNLRtogether,andincomparisonwitheachother,inthe diagnosisandprognosisoftheSHLpatients.SinceNLRisan indicatorofinflammation andMPVindicates atherothrom-bosis, this study aimedto contribute tothe literature by investigatingtheroleofinflammationandatherothrombosis inSHLpatientsbyusingNLRandMPV,respectively.
Methods
NLRwascalculatedasasimpleratiobetweenthe abso-lute neutrophil and the absolute lymphocytecounts. The Beckman Coulter LH 750 automated blood cell counter (Beckman Coulter analyzer, CA, United States) was used forcompletebloodcount(CBC)measurements(Neutrophil, lymphocyte,platelet,NLR,MPVandWBC),whichbasedon techniqueoflaserflow cytometryscattergrams,andwere performed within2h afterblood sampling.Bloodsamples fromthe patientgroup were obtainedbefore the patient wasadministeredany treatment. Allsamples were runin duplicate, and the mean values were used for statistical analysis.
Audiometric examinations were performed in quiet rooms with an Interacoustics AC-40 clinical audiometer accordingtothemanufacturerinstructions,andallthetests wereconductedbythesameaudiometrist.Audiologicdata werereportedinaccordancewiththerecommended meth-odsoftheHearingCommitteeoftheAmericanAcademyof Otolaryngology, Head, and Neck Surgery, which endorsed a new minimal standard for reporting hearing results in clinicaltrials.22 Audiometricexaminationswereperformed
initiallyandafteronemonthofthetreatment.SHLpatients hadaminimumof 30dBhearingloss atthreeconsecutive frequencies thatdeveloped within 72h andwas not asso-ciated withother known pathologies, including Meniere’s disease,autoimmunedisease,ototoxicity,orneoplasm.The hearinglosswasunilateralinallpatients.
Allofthe patientsweretreated withthe standardSHL protocol,whichincludedprednisoneinthedoseof1mg/kg perday,withaprogressivedosereduction,maintainedfor at leasttwo weeks.The mean intervalof theblood tests followingtheonsetofSHLwas1.98±1.26days(range1---6 days)
Patients were classified as follows (according to the recoveryobservedinonemonthoffollow-up):1---Complete: puretoneaverage(PTA)within10dBhearinglevels(HL)of initialHLorwithin10dBHLoftheHLoftheunaffectedear; 2--- Partial: PTAdB HLwithin50% of initial HLor greater than10dBHLimprovementoftheHL;and3---norecovery: lessthan10dBHLimprovementinHLrelativetotheinitial HL1.Then,the patients weredivided intotwogroups as
recovered(Complete+Partial)andunrecovered(No recov-ery). The patientswere alsodivided intothreesubgroups accordingtoseverityofhearinglossasmild(<40dBlossfor anyfrequency),moderate(upto80dB),andsevere(>80dB). Age, gender, MPV, NLR, and other laboratory data of thepatientswererecordedforallgroups.Thecorrelations betweentheMPVandNLRwereevaluatedintheSHLgroup andinthecontrolgroup,andSHLpatientswerecompared accordingtotherecoveryandseverityofhearingloss.Also, correlationbetweentheMPVandNLRwasdeterminedinthe SHLpatientgroup.
Thestudy wasapprovedby thelocalethicscommittee and conducted in accordance with the ethical principles describedbytheDeclarationofHelsinki.Aninformed con-sent was obtained from all participants prior to their participationinthestudy.
SPSSfor Windows,version 15.0,softwarewasusedfor alldataanalyses.Datadistributionswereanalyzedwiththe Shapiro---Wilk test. Student’s t-test for independent sam-ples was used to analyze age, MPV values, and platelet count. In cases of normal distribution,Mann---Whitney’s U test was used to compare the groups (gender). The cor-relations between the variable pairs were analyzed using Pearson’scorrelationtest.Alevelofp<0.05wasconsidered significant.
Results
Therewasnosignificantdifferencebetweentheageor gen-derintheSHLandcontrolgroups.Themeanageofpatients and controls were 46.10±11.91 and 42.84±11.85 years, respectively.Themale-to-femaleratiointheSHLgroupwas 38:21,and31:28inthecontrolgroup(Table1).
Thelaboratorydataofpatients andcontrols areshown in Table 1.The mean MPVvalue was9.83±1.50fLin the patients and 9.98±0.07fL in the control group, and the differencewasnot statisticallysignificant (p=0.470).The mean NLR value was 3.24±2.26 in the SHL patients and 1.53±0.47 in the control group, and the difference was statisticallysignificant(p=0.001;Table1).
Table1 Intergroupcomparisonofage,gender,meanplateletvolume(MPV),neutrophil-to-lymphocyteratio(NLR)values,and plateletcountsofthepatientsandthecontrolgroup.
Variables Patient(n=59) Mean±SD
Control(n=59) Mean±SD
p-Value
Age(years) 46.10±11.91 42.84±11.85 0.140
Gender 0.193
Female 21(35.6%) 28(47.5%)
Male 38(64.4%) 31(52.5%)
NLR 3.24±2.26 1.53±0.47 0.001a
MPV(fL) 9.83±1.50 9.98±0.07 0.470
Platelet(103U) 249.44±48.16 244.86±47.25 0.603
WBC(103U) 8.39±2.83 6.29±0.973 0.001a
Neutrophil(103U) 5.64±2.55 3.43±0.71 0.001a
Lymphocyte(103U) 2.06±0.77 2.35±0.53 0.029a
SD,standarddeviation;WBC,whitebloodcell.
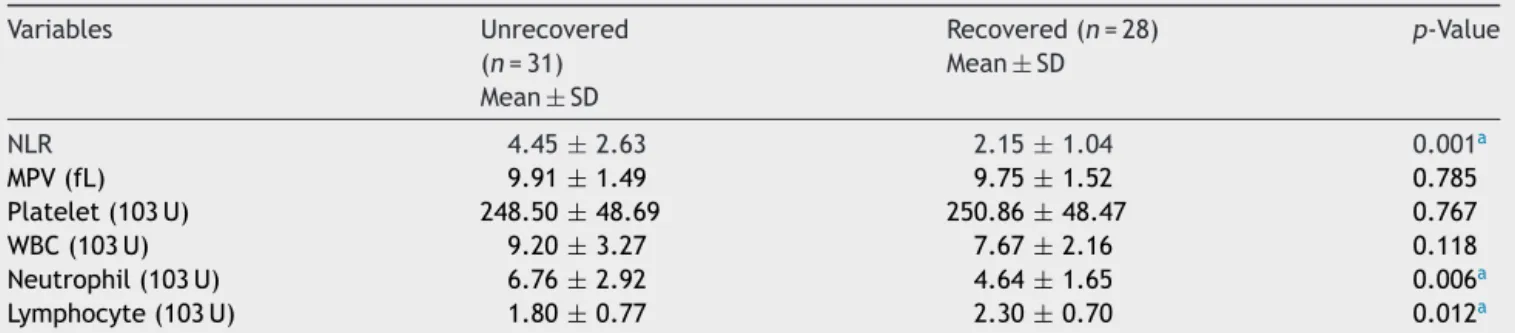
The laboratory data of the SHL group according to response tothe treatment asrecovered and unrecovered groups are shown in Table 2. The mean MPV value was 9.91±1.49fL in theunrecovered group and9.75±1.52fL in the recovered group, and the difference was not sta-tistically significant (p=0.785). The mean NLR value was 4.45±2.63intheunrecoveredgroupand2.15±1.04inthe recoveredgroup,andthedifferencewasstatistically signif-icant(p=0.001;Table2).
The meanNLRandMPV valuesaccording toseverityof hearinglossareshowninTable3.Astatisticallysignificant correlation wasobserved between NLR values and sever-ityofhearingloss(p=0.015).The meanNLRvaluesinthe patients withsevereSHL weresignificantly higherthanin themildSHLgroup(p=0.004).However,therewasno cor-relation between MPV values and severity of hearing loss (p=0.701).
NocorrelationwasobservedbetweenMPVandNLRinthe SHLgroup(r=0.190;p=0.149).
Discussion
The key to successful treatment of diseases lies in the understanding of their etiopathogenesis. Since the phys-iopathology of SHL is still unclear, there are conflicting theoriesregardingitstruecause.8,23,24Therearemany
theo-riesastotheoriginofthisdisease,includingviralinfections, inflammation, blood disorders, vascular causes, immune disorders,andruptureofthelabyrinthinemembrane.12,25,26
Sincethecochlea is mainlysupplied by asingle,terminal
artery(thelabyrinthineartery),theinnerearisverymuch prone to circulatory alterations.27 In vascular cases, the
problemsmaybepresentonthebloodvesselwall,asisthe caseinarteritisandspasms,ortheymaybeintravascular. Ahistoryof vascular diseaseor platelet alterationsis the onlyclinicalfindingthatcouldleadonetoinferavascular causeofSHL. Althoughthe mostwidely accusedfactor in theetiology is viralinflammation ofthe neuralfibers and ganglia,28thishasnotbeenprovenyet.
NLR is an easily measured biomarker that correlates with clinical status. It is calculated from CBC, and is an inexpensive, easy to obtain, widely available marker of inflammation that can aid in the risk stratification of patients withvarious diseases.1,13,29,30 It is as valuable as
some high-cost inflammatory markers, including IL-6, IL-1, IL-8, and TNF-␣.31 Conversely, MPV can be used as
marker for high platelet activity, which takes an active roleinthepathophysiologyofthrombosis,coagulation,and atherosclerosis.32
Inrecent studies,NLRwasdeterminedtobeareliable markerforthediagnosisandpredictionoftheSHLandBell’s palsyprognoses.14,15,33 Ulu et al. reported that when the
patientswithSHLwerecomparedaccordingtotherecovery, NLRlevelswerehigherinpatientswhodidnotrecover.This may be explainedwith the higher inflammatory situation inunrecoveredpatients,andthisresultmayhelpclinicians caringforSHL patientswithhigherNLR levelsinterms of treatmentandprognosis.15InthepreviousstudybyMasuda
etal.,neutrophilandlevelsofinflammatorymarkerswere higherinSHLpatients.34 Mostrecently,OzlerclassifiedSHL
patientsaccordingtoseverityofhearinglossasmild(<40dB
Table2 Comparisonoflaboratorydatabetweentherecoveredandunrecoveredpatients.
Variables Unrecovered (n=31) Mean±SD
Recovered(n=28) Mean±SD
p-Value
NLR 4.45±2.63 2.15±1.04 0.001a
MPV(fL) 9.91±1.49 9.75±1.52 0.785
Platelet(103U) 248.50±48.69 250.86±48.47 0.767
WBC(103U) 9.20±3.27 7.67±2.16 0.118
Neutrophil(103U) 6.76±2.92 4.64±1.65 0.006a
Lymphocyte(103U) 1.80±0.77 2.30±0.70 0.012a
SD,standarddeviation;MPV,meanplateletvolume;NLR,neutrophil-to-lymphocyteratio;WBC,whitebloodcell.
a p<0.05.
Table3 MeananalysisforNLRandMPVaccordingtoseverityofhearinglossasmild(<40dB),moderate(upto80dB),and severe(profound,>80dB).
1Mild(n=24) 2Moderate(n=24) 3Severe(n=11) p Mean±SD Mean±SD Mean±SD
MPV(fL) 9.83±1.58 9.74±1.56 10.00±1.27 0.701 NLR 2.35±1.14 3.25±2.06 5.15±3.33 0.015a
1---2,p=0.117 2---3,p=0.092 1---3,p=0.004a
SD,standarddeviation;MPV,meanplateletvolume;NLR,neutrophil-to-lymphocyteratio.
lossforanyfrequency),moderate(upto80dB),andsevere (>80dB),and found thatthe meanNLR valuesin patients withSHLweresignificantlyhigherthaninthecontrolgroup, andthatthemeanNLRvaluesinpatientswithsevere sen-sorineuralhearinglossweresignificantlyhigherthaninthe othergroups.35 In thepresent study,NLRvalueswere
sig-nificantlyhigherinpatientswithSHLwhencomparedwith thecontrolgroup.Similarly,themeanNLRwashigherinthe unrecoveredpatientswhencomparedwiththosewho recov-ered; asignificant correlation wasobserved between NLR valuesandseverityofhearingloss,indicatingthepresence ofinflammation.
Platelets play an active role in the pathophys-iology of thrombosis, coagulation, inflammation, and atherosclerosis.9,36 Upon activation, platelets release
vasoactiveandthrombogenicagents, whichareimportant factorsin the formation ofthrombosis in thevessel. Sev-eralinvestigatorshaveusedaseriesofplateletindicesthat aremeasuredbyhematologyanalyzers,sinceplatelet acti-vationleadstomorphologic changes.37 Largeplatelets are
metabolically and enzymatically more active and have a higherthromboticpotential.38 Higher MPVvaluesare
ben-eficialmarkers ofhigher plateletactivity andwere found tobe associatedwith atherothrombosis. In addition,MPV is oneof the most extensivelystudied platelet activation markers.32,39
MPVvalueswerestudied inpatients withSHL,yielding controversial results. In the recent studies by Ulu et al. (with 40 patients and controls) and by Sagit et al. (with 31 patients and controls), the mean MPV values in SHL patientswere10.5±0.9fLand9.01±1.24fL,respectively, whichweresignificantlyhigherthanthevaluesofthecontrol groups(9.6±0.5fLand8.21±0.76fL,respectively).20,21In
another study by Karli et al. (with 46 patients and con-trols),themeanMPVvaluewas8.25±0.86fLinSHLpatients and7.98±0.87fLinthecontrolgroup,whichwasnot sig-nificantly different, and they concluded that there was nomicrovascular responsein theetiology ofSHL.19 Inthe
presentstudy(with59patientsandcontrols),themeanMPV valuewas9.83±1.50fL inSHLpatients and9.98±0.07fL in the control group; similarly, the mean MPV value was 9.91±1.49fLintheunrecoveredgroup,and9.75±1.52fL intherecovered group,andtherewasnosignificantly dif-ferencebetweenthegroups.Theabsenceofanycorrelation ofMPVwithanyofthestudiedparametersmaysuggestthat microvascularresponseisasuspicioustheoryin etiopatho-genesisofSHL.
In a large epidemiologic study with 326 patients by Demirinetal.,themeanMPVvalueinnormalTurkishadults was 8.9±1.4fL, and 95% of the individuals had an MPV between 7.2 and 11.7fL.40 If the MPV values of the
con-trol group in this study were equivalent to those of the studybyDemirinetal.,thepresentresultswouldhavebeen consideredsignificant.
Conclusion
Theresults ofthe presentstudy indicated that,whenthe SHLpatientswerecomparedaccordingtotherecovery,NLR levelswerehigherinpatientswhodidnotrecover.However, nosuchcorrelation wasobservedbetween MPVlevelsand
patientrecovery.Thismayindicatethatinflammationplays alargerroleinthepathogenesisofSHLthanthe microvas-cular response. In the evaluation of SHL, NLR is a quick andreliable markerfor predictingthe diagnosisand prog-nosis,whileMPVmaybealessimportantmarker.Although the presentsample size waslargerthan thatusedin pre-vious studies, thisissue shouldbeinvestigatedin alarger patientcohort.Becausethisareaofresearchisanovelfield, prospective,multicenter,controlledstudiesareneeded.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.WilsonWR,BylFM,LairdN.Theefficacyofsteroidsinthe treat-mentofidiopathicsuddenhearingloss.Adouble-blindclinical study.ArchOtolaryngol.1980;106:772---6.
2.CadoniG,AgostinoS,MannaR,DeSantisA,FetoniAR, Vulpi-aniP,etal.Clinicalassociationsofserumantiendothelialcell antibodiesinpatientswithsuddensensorineuralhearingloss. Laryngoscope.2003;113:797---801.
3.ChauJK,LinJR,AtashbandS,IrvineRA,WesterbergBD. Sys-tematicreviewoftheevidencefortheetiologyofadultsudden sensorineuralhearingloss.Laryngoscope.2010;120:1011---21. 4.Cadoni G, Agostino S, Scipione S, Ippolito S, Caselli A,
MarcheseR,etal.Suddensensorineuralhearingloss:our expe-rienceindiagnosis, treatment,and outcome.JOtolaryngol. 2005;34:395---401.
5.MerchantSN,DurandML,AdamsJC.Suddendeafness:isitviral? ORLJOtorhinolaryngolRelatSpec.2008;70:52---60[discussion -2].
6.KuhnM,Heman-AckahSE,ShaikhJA,RoehmPC.Sudden sen-sorineuralhearingloss:areviewofdiagnosis,treatment,and prognosis.TrendsAmplif.2011;15:91---105.
7.VasamaJP, Linthicum FH Jr. Idiopathic sudden sensorineural hearing loss: temporalbone histopathologicstudy. Ann Otol RhinolLaryngol.2000;109:527---32.
8.Lazarini PR, Camargo AC. Idiopathic sudden sensorineural hearingloss:etiopathogenicaspects.BrazJOtorhinolaryngol. 2006;72:554---61.
9.Coppinger JA, Cagney G, Toomey S, Kislinger T, Belton O, McRedmond JP, et al. Characterization of the proteins released from activated platelets leads to localization of novelplateletproteinsinhumanatheroscleroticlesions.Blood. 2004;103:2096---104.
10.OzkanB,UysalOK,DuranM,SahinDY,ElbasanZ,TekinK,etal. Relationshipbetweenmeanplateletvolumeand atherosclero-sisinyoungpatientswithSTelevationmyocardialinfarction. Angiology.2013;64:371---4.
11.RudigerA,BurckhardtOA,HarpesP,MullerSA,FollathF.The relativelymphocytecountonhospitaladmissionisariskfactor forlong-termmortalityinpatientswithacuteheartfailure.Am JEmergMed.2006;24:451---4.
12.Murai K, TsuikiT, ShishidoK, Hori A. Clinical studyof sud-dendeafnesswithspecialreferencetoonset.ActaOtolaryngol Suppl.1988;456:15---20.
13.Tamhane UU, AnejaS, MontgomeryD, Rogers EK,EagleKA, Gurm HS. Associationbetween admission neutrophil to lym-phocyteratio and outcomes inpatientswith acutecoronary syndrome.AmJCardiol.2008;102:653---7.
factoratthehearinglossofdiabeticpatients.EurArch Otorhi-nolaryngol.2014;271:2681---6.
15.Ulu S, Ulu MS, Bucak A, Ahsen A, Yucedag F, Aycicek A. Neutrophil-to-lymphocyte ratio as a new, quick, and reli-able indicator for predicting diagnosis and prognosis of idiopathic sudden sensorineural hearing loss. Otol Neurotol. 2013;34:1400---4.
16.UluSM,DoganM,AhsenA,AltugA,DemirK,AcarturkG,etal. Neutrophil-to-lymphocyteratioasaquickandreliable predic-tivemarkerto diagnosetheseverity ofdiabeticretinopathy. DiabetesTechnolTher.2013;15:942---7.
17.Ahsen A, Ulu MS, Yuksel S, Demir K, Uysal M, Erdogan M, et al. As a new inflammatory marker for familial Mediter-ranean fever: neutrophil-to-lymphocyte ratio. Inflammation. 2013;36:1357---62.
18.IsikT, AyhanE,UyarelH, TanbogaIH,Kurt M,Uluganyan M, etal.Associationofneutrophiltolymphocyteratiowith pres-enceofisolatedcoronaryarteryectasia.TurkKardiyolDernArs. 2013;41:123---30.
19.KarliR,AlacamH,UnalR, KucukH,AksoyA,AyhanE.Mean plateletvolume:isitapredictiveparameterinthediagnosis ofsuddensensorineuralhearingloss?IndianJOtolaryngolHead NeckSurg.2013;65:350---3.
20.SagitM,KavugudurmazM,GulerS,SomdasMA.Impactofmean plateletvolumeontheoccurrenceandseverityofsudden sen-sorineuralhearingloss.JLaryngolOtol.2013;127:972---6. 21.UluS,UluMS,AhsenA,YucedagF,AycicekA,CelikS.Increased
levelsofmean platelet volume: a possiblerelationship with idiopathic sudden hearing loss. Eur Arch Otorhinolaryngol. 2013;270:2875---8.
22.GurgelRK,JacklerRK,DobieRA,PopelkaGR.Anew standard-ized format for reporting hearingoutcome inclinical trials. OtolaryngolHeadNeckSurg.2012;147:803---7.
23.FukudaS,FurutaY,TakasuT,SuzukiS,InuyamaY,Nagashima K.Thesignificanceofherpesvirallatencyinthespiralganglia. ActaOtolaryngolSuppl.1994;514:108---10.
24.PitkarantaA, Julkunen I.Suddendeafness: lackof evidence for systemic viral infection. Otolaryngol Head Neck Surg. 1998;118:397---9.
25.ColeRR,JahrsdoerferRA.Suddenhearingloss:anupdate.Am JOtol.1988;9:211---5.
26.Yoshida Y, Yamauchi S, Shinkawa A, Horiuchi M, Sakai M. Immunologicalandvirologicalstudyofsuddendeafness.Auris NasusLarynx.1996;23:63---8.
27.MosnierI,StepanianA,BaronG,BodenezC,RobierA,MeyerB, etal.Cardiovascularandthromboembolicriskfactorsin idio-pathicsuddensensorineuralhearingloss:acase---controlstudy. AudiolNeurootol.2011;16:55---66.
28.Stokroos RJ,Albers FW,SchirmJ. Theetiology ofidiopathic sudden sensorineural hearingloss. Experimental herpes sim-plex virus infection of the inner ear. Am J Otol. 1998;19: 447---52.
29.Paramanathan A, Saxena A, Morris DL. A systematic review and meta-analysis ontheimpactofpre-operative neutrophil lymphocyteratioonlongtermoutcomesaftercurativeintent resectionofsolidtumours.SurgOncol.2014;23:31---9. 30.SzkanderaJ,Gerger A,Liegl-AtzwangerB,AbsengerG,Stotz
M, Friesenbichler J, et al. The lymphocyte/monocyte ratio predicts poor clinical outcome and improves the predictive accuracy inpatientswithsofttissue sarcomas.IntJCancer. 2014;135:362---70.
31.TurkmenK,GuneyI,YerlikayaFH,TonbulHZ.Therelationship between neutrophil-to-lymphocyte ratio and inflammationin end-stagerenaldiseasepatients.RenFail.2012;34:155---9. 32.Gasparyan AY, Ayvazyan L, Mikhailidis DP, Kitas GD. Mean
plateletvolume:alinkbetweenthrombosisandinflammation? CurrPharmDes.2011;17:47---58.
33.Bucak A, Ulu S, Oruc S, Yucedag F, Tekin MS, Karakaya F, et al. Neutrophil-to-lymphocyte ratio as a novel-potential marker for predicting prognosis ofBell palsy. Laryngoscope. 2014;124:1678---81.
34.MasudaM,KanzakiS,MinamiS,KikuchiJ,KanzakiJ,SatoH, etal.Correlationsofinflammatorybiomarkerswiththeonset andprognosisofidiopathicsuddensensorineuralhearingloss. OtolNeurotol.2012;33:1142---50.
35.Ozler GS. Increased neutrophil---lymphocyteratio inpatients withidiopathicsuddensensorineuralhearingloss.JCraniofac Surg.2014;25:e260---3.
36.Gawaz M, Langer H, May AE.Platelets in inflammation and atherogenesis.JClinInvest.2005;115:3378---84.
37.Gasparyan AY,Stavropoulos-KalinoglouA,MikhailidisDP, Dou-glasKM, KitasGD. Plateletfunction inrheumatoid arthritis: arthritic and cardiovascular implications. Rheumatol Int. 2011;31:153---64.
38.EndlerG,KlimeschA,Sunder-PlassmannH,SchillingerM,Exner M,MannhalterC,etal.Meanplateletvolumeisanindependent riskfactorformyocardialinfarctionbutnotforcoronaryartery disease.BrJHaematol.2002;117:399---404.
39.GreiseneggerS,EndlerG,HsiehK,TentschertS,MannhalterC, LalouschekW.Iselevatedmeanplateletvolumeassociatedwith aworseoutcomeinpatientswithacuteischemic cerebrovascu-larevents?Stroke.2004;35:1688---91.