w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Differences
between
polydioxanone
and
poliglactin
in
intestinal
anastomoses
–
a
comparative
study
of
intestinal
anastomoses
Carlos
Henrique
Marques
dos
Santos
a,b,∗,
Kerginaldo
Gondim
dos
Santos
Filho
a,
Pedro
Carvalho
Cassino
a,
Camila
Vieira
Chiquetti
a,
Alvaro
Pereira
de
Mello
a,
Doroty
Mesquita
Dourado
baUniversidadeFederaldeMatoGrossodoSul(UFMS),HospitalUniversitárioMariaAparecidaPedrossian(HUMAP),CampoGrande,
MS,Brazil
bUniversidadeAnhanguera(Uniderp),CampoGrande,MS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30March2017 Accepted17May2017 Availableonline14July2017
Keywords:
Anastomosis,surgical Polydioxanone Polyglactin910 Rats
Smallintestine
a
b
s
t
r
a
c
t
Introduction:Intestinalanastomosisisasurgicalpracticeconstantlyrealizedbysurgeons worldwide.Whentheoptionistoperformmanualanastomosis,whichisstillwidelyused foritslowcost,thequestionarisesastothebestmaterialtobeapplied.
Objective:To compare polydioxanone and polyglactin threads for healing and tensile strengthinintestinalanastomosisinrats.
Method:Weused25ratsWistar;afteranesthesia,ingroupsAandB(10ratseach), laparo-tomywasperformed,transectionoftheileumat5and10cmproximallytotheileocecal valve;ingroupA,anastomosiswasperformedwith4separateextramucosalsutureswith polidioxanone;ingroupB,anastomosiswasperformedwithpolyglactin;ingroupC(5rats), laparotomyandmanipulationoftheileumwereperformed.After21days,theanimalswere anesthetizedandsubmittedtoeuthanasia.Thespecimensweresentforhistopathological studyandtensilestrengthanalysis.StatisticalanalysiswasperformedusingtheTurkeyand Student’sttests,withasignificanceofp<0.05.
Results:Theresultsshowedthatinthetensilestrengthanalysis,therewerenosignificant differencesbetweenthem.Thehistologicalanalysisshowedsignificantdifferencesbetween thecicatrizationpattern,wherepolydioxanonecausedlessfibrosisthanpolyglactin.
Conclusion: Polydioxanonecausedlessfibrosisthanpolyglactininintestinalanastomosesof rats.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](C.H.Santos). http://dx.doi.org/10.1016/j.jcol.2017.05.004
Diferenc¸as
entre
polidioxanona
e
poliglactina
em
anastomoses
intestinais
–
estudo
comparativo
de
anastomoses
intestinais
Palavras-chave:
Anastomosecirúrgica Polidioxanona Poliglactina910 Ratos
Intestinodelgado
r
e
s
u
m
o
Introduc¸ão: Anastomoseintestinaléumapráticacirúrgicaconstantementerealizadapelos cirurgiõesemtodoomundo.Quandoaopc¸ãoéaanastomosemanual–umprocedimento aindaamplamenteempregado,grac¸asaseubaixocusto–coloca-seoproblemadesaber qualéomelhormaterialaseraplicado.
Objetivo: Compararfiosdepolidioxanonaepoliglactinaquantoàcicatrizac¸ãoeresistência àtrac¸ãoemanastomosesintestinaisemratos.
Método:Utilizamos25ratosWistar;depoisdaanestesia,foirealizadalaparotomianosgrupos AeB(10ratoscada),comtransecc¸ãodoíleoa5e10centímetrosproximalmenteàválvula ileocecal;nogrupoA,aanastomosefoirealizadacom4suturasdemucosaseparadascom usodepolidioxanona;nogrupoB,aanastomosefoirealizadacompoliglactina;nogrupoC (5ratos),foirealizadaapenasalaparotomiaemanipulac¸ãodoíleo.Transcorridos21dias, osratosforamanestesiadosesubmetidosàeutanásia.Osespécimesforamenviadospara estudohistopatológicoeanálisederesistênciaàtrac¸ão.Aanáliseestatísticafoiefetuada comaaplicac¸ãodostestesdeTukeyedetdeStudent,comsignificânciadep<0,05.
Resultados: Os resultados demonstraram que, na análise de resistência à trac¸ão, não foramobservadasdiferenc¸assignificativasentreosmateriais.Aanálisehistológica rev-eloudiferenc¸assignificativasentrepadrõesdecicatrizac¸ão,emquepolidioxanonacausou menosfibroseversuspoliglactina.
Conclusão::Polidioxanonacausoumenosfibroseversuspoliglactinaemanastomoses intesti-naisrealizadasemratos.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Many methods of intestinal suture have been performed sincetheearliestdaysofsurgery.However,onlyintheyear 1264,Ruggieropresentedthesurgicalpracticeofthe diges-tivesuture,usingsilkthreads.Richerand,inthenineteenth century, presentedthe theory of incoherenceof the union ofserosawithmucosa,beginningtheideaofperformingan intestinalanastomosisjoiningtheextramucosallayers.1
Afearedcomplicationinthistypeofanastomosis, dehis-cences and fistulas represent an important problem for specialistsdealingwiththedigestivetract,sincetheycanlead tosevere electrolytedepletion, acid-baseimbalance, infec-tionandsevere malnutrition,withalong hospitalstayand thehighcostoftreatment.Severalfactorssuchas malnutri-tion,infection,ischemia,etc.mayberelated,butthetechnical failure and type of anastomosis performed must also be considered.2
Intestinal anastomoses can be performed with one or twocontinuouslayers,separatestitches,withan invaginat-ing orevadingend resultoftheedgesofthe anastomosis. Variousmaterialsareusedtomakethesesutures, suchas: silk, cotton, linen and synthetic threads. The most com-monlyusedmanualtechniqueissingle-layer,extra-mucosal, withmonofilamentyarns,whilemanyuse mechanical sta-plers,whichhavetheadvantageofshorteningoperativetime, althoughtheyincreasethecostoftheprocedure.3
Thereisnoevidencethatstapledanastomosisissuperiorto manual.Infact,thestapledsuturemayevenleadtoahigher
rateofpostoperativebleedinginsomesituations.4,5 Despite
this,staplingwasaveryimportantadvanceinintestinal anas-tomosesandshouldbeincreasinglyimproved.However,there isstillroomformanualanastomosis,especiallysinceitallows forlowercosts.
Garude et al.6 demonstrated that thereis no benefitin
performing intestinalanastomosis intwoplanes,the anas-tomosisinanextramucosalsingleplanebeingasefficientas that,butperformedmorequicklyandeconomically.
Bernis-Filhoetal.7 comparedcotton,polyglecaproneand
polyglactin threads in intestinal anastomoses ofdogs and observed no difference between these materials. It would beexpectedthat multifilamentthreadssuchascottonand polyglactin caused a greater tissue reaction, which was not proven when compared to polyglecaprone. Although polydioxanoneandpolyglecaprone arebothabsorbableand monofilamentary, they have different characteristics, and polydioxanonehasbeenpreferredforintestinalanastomosis, althoughthereisnoscientificevidenceofitssuperiority.Thus, itremainstobeseenwhetherthereisanydifferencebetween thetypeofmaterialusedforsuchanastomoses,andthe objec-tiveofthisstudyistocomparepolydioxanoneandpolyglactin threadsforhealingandtensilestrengthinintestinal anasto-mosesinrats.
Objective
Material
and
methods
ThestudywassubmittedtotheapprovaloftheAnimalEthics CommitteeoftheFederalUniversityofMatoGrossodoSul, followingalltherulesoftheCEUA–EthicsCommitteeon Ani-malUse,andCOBEA–BrazilianSocietyofAnimalLaboratory Science.
Twenty-fivemaleWistar(Rattusnorvegicus)rats,weighing approximately300gwerestudied,fromtheVivariumofthe FederalUniversityofMatoGrossodoSul.Theanimalswere keptintheexperimentalareaoftheUFMSCentralVivarium, accordingtoallstandards.
Theanimalsweredistributedintothreegroups:
- GroupA(polidioxanone):10ratssubjectedtointestinal sec-tionandanastomosiswithpolydioxanone4–0.
- GroupB(polyglactin):10ratssubjectedtointestinalsection andanastomosiswithpolyglactin4–0.
- Group C (control): 5 rats subjected to laparotomy and manipulationoftheileum,withoutintestinalsectionand anastomosis.
Anesthesiawasperformedbyintraperitoneal administra-tion of ketamine and xylazine, in the same syringe. The solutionwascomposedof1.0mLofketamine10%and1.0mL ofxylazine2%,0.1mLofthesolutionbeingadministeredper 100gofweight.
Each animal was anesthetized and then placed in dor-saldecubitusposition,withabductionpaws,withamedian laparotomyof3cm.IngroupC,theileumwasonly manipu-lated,followedbyclosureoftheabdominalwall.Intheother groups,theintestinewasexternalizedtothelocationofthe ileocecalvalve;5cmand10cmproximaltotheileocecalvalve wereperformedthetransectionsoftheentireintestinal cir-cumferencewithcoldscalpel,preservingthemesentery.An extramucosalend-to-endanastomosiswasthenperformed withfour separatesites inthe twotransectionareas, with 4–0polydioxanone(PDS®,Ethicon,USA)ingroupAand4–0 polyglactin(Vicryl®,Ethicon,USA)ingroupB.Theintestine wasrepositionedintheabdominalcavity,whichwasclosed bycontinuoussuturewith3–0nylonthread.
Theanimals were keptin individual cages for 21 days, withfoodandwateradlibitum.Afterthisperiod,theywere againanesthetizedandsubjectedtoeuthanasiaby intracar-diacadministrationofsodiumthiopental.Anewlaparotomy wasperformedand15cmoftheileumfromtheileocecalvalve wereresected.Thesegmentscontainingthe5cmpoint anas-tomosisofgroupsAandBandtheequivalentareawithout sutureofgroupC,withproximalanddistalmarginsof2cm (sample1) (Fig.1),wereremoved,washedwithsaline solu-tionandplacedinpreviouslyidentifiedtubescontaining10% formaldehydeforfurtherhistologicalanalysis.Thismaterial wassenttothe pathologyforthe preparationofthe slides thatwerestainedwithhematoxylinandeosinforanalysisof granulationtissueandhealingwithaNikonE200microscope andmillimetereyepieces.Thesegmentscontainingthe10cm pointanastomosisofgroupsAandBandtheequivalentarea withoutsutureofgroupC,withproximalanddistalmargins of2cm(sample2)(Fig.1),wereremoved,washedwithsaline
Ileocecal value
5cm 10cm
2cm
Sample 1 Sample 2
2cm 2cm 2cm
Fig.1–Schematicdiagramshowingtheresectedsegments forstudy.Sample1:histopathologicalstudy;Sample2: tensileforceanalysis.
solutionandsubmittedtotensilestrengthanalysiswiththe use oftheInstrol apparatus, calibratedinNewton (N).The apparatus wasprogrammedto exerttensile forceuntil the ruptureofthetissuethatwasmountedintheapparatuswith theuseofownclaws,respectingthedistanceof2cmof mar-ginoftheanastomosisforeachsideofthefixation.Thevalue oftheresultinNewton(N)wasconvertedtokilogramforce (kgf),toperformthestatisticalanalysis.
Statistical analysiswasperformedusingthe Turkeyand Student’sttests,withasignificanceofp<0.05.
Results
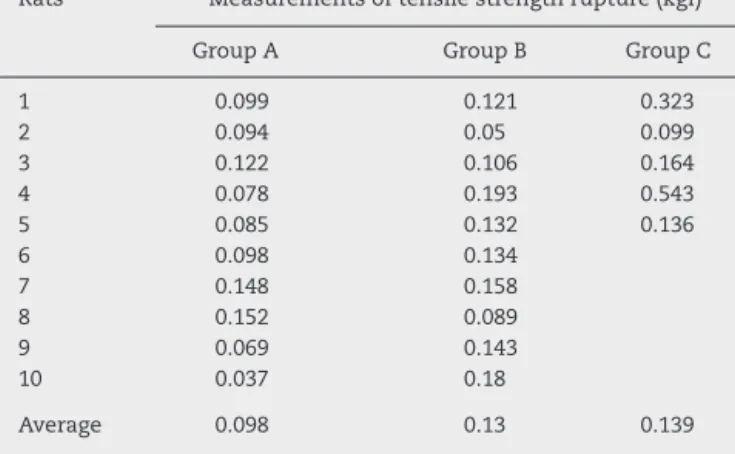
The results in relation to the tensile strength of rupture showedaverage0.098ingroupA,0.13ingroupBand0.139 ingroupC(Table1andFig.2).
Theanalysisofvariance appliedtothe differentgroups revealed no significant difference betweenthem (p=0.085). Thus,therewasnoneedtocomplementtheanalysisbythe Tukeytestfortwo-to-twocomparisons.
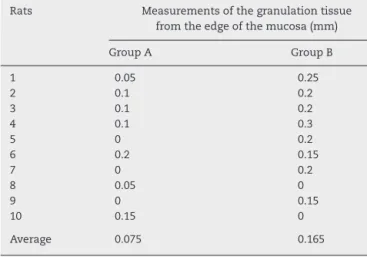
Theresultsoffibrosisevaluationfoundwere0.075forgroup A and 0.165 for group B (Table 2 and Fig. 3). Student’s t -testappliedtothelengthofthemucosalborders,revealeda significantdifferencebetweenthemeasuredhealingpattern (p=0.027),andtherewaslessfibrosiswithpolydioxanone.
Discussion
Thecicatricialprocessisofextremeimportanceinan intesti-nalanastomosis,andoccursinthreephases:inflammatory,
Table1–Analysisoftensilestrengthbetweendifferent groups.
Rats Measurementsoftensilestrengthrupture(kgf)
GroupA GroupB GroupC
1 0.099 0.121 0.323
2 0.094 0.05 0.099
3 0.122 0.106 0.164
4 0.078 0.193 0.543
5 0.085 0.132 0.136
6 0.098 0.134
7 0.148 0.158
8 0.152 0.089
9 0.069 0.143
10 0.037 0.18
0.16
0.14
0.12
0.1
0.08
0.06
0.04
0.02
0
Group A Group B Group C
Fig.2–Averageofrupturetensilebetweenthedifferent groups,expressedinkgf.
Table2–Measurementsofgranulationtissueinthe anastomosisareabetweenthedifferentgroups.
Rats Measurementsofthegranulationtissue
fromtheedgeofthemucosa(mm)
GroupA GroupB
1 0.05 0.25
2 0.1 0.2
3 0.1 0.2
4 0.1 0.3
5 0 0.2
6 0.2 0.15
7 0 0.2
8 0.05 0
9 0 0.15
10 0.15 0
Average 0.075 0.165
proliferativeandmaturationandremodeling,whichpresent certainoverlapatcertainmoments.Ahealthybodyshould haveadequatehealing,whichcouldbehamperedbyfactors such as malnutrition, local and systemic infection, use of certaindrugssuchascorticosteroids,etc.Theseare usually factorsinherenttothepatientandwithlimitedpossibilityof theattendingphysician.Thus,thosefactorsdirectlyrelated
0.18
0.16
0.14
0.12
0.1
0.08
0.06
0.04
0.02
0
Group A Group B
Fig.3–Averagelengthofedgesofthemucosa,expressed inmillimeters.
to thesurgeon’s performanceduringananastomosis,such asthepreservationofadequate bloodsupply,theoperative techniqueandthematerialused,becomemoreimportantin medicalpractice.8
Whenahand-sewnanastomosisisperformed,thethread usedwillplayaroleinthefirststageofhealing,whenthere isareactionagainstthematerial,sincethisisaforeignbody andwilltriggeraninflammatoryprocessthatwillbeoflonger orshorterduration,aswellaslargerorlessintensity depend-ingontheamountofthreadused,itsstructure,i.e.whether itismonoormulti-filamentandthematerialofwhichitis composed.9Whetherthesefactorsinfluencetensilestrength
andtheincidenceofdehiscencearestilltobeanswered. In the present study, it was observed that the poly-dioxanone thread presented less fibrosis formation than polyglactin, which can beunderstood bythe fact that the first one is monofilament, which would lead to a lower inflammatoryprocessandconsequentlylesstissuefibrosis.10
Comparison ofhand-sewn anastomoses withstapled ones andmorerecentlywiththeuseofcompressiondevicesmake usobservethatthesmallertheuse offoreignmaterial,the bettertheanastomosisduetothelowerfibrosis.Inarecent study usingacompressiondevice, satisfactoryresultswere obtainedwithoutthepresenceofforeignmaterialandits pos-siblecomplications.11Inasystematicreviewof1233patients
comparingmechanicalstaplerswithhand-sewnbowelsuture, nodifferenceswerefoundintheresults,however,staplesare knowntotriggeralowerinflammatoryresponsethan multi-filamentthreadssuchaspolyglactin.12
The sutures are performed for two purposes: to main-taincoaptationoftheedgesoftheoperativewoundandto resisttheextrinsictensionforcesuntilthescaracquiresits owntensionforce.Normallyinthefirstfourdaysthis intrin-sicforceisvirtuallyzero,growingprogressivelyuntilhealing keepstheedgestogetherindependentlyofthestitches.The timetakenforthistooccurisvariable,dependingonthe tis-sueanalyzed,thespeciesandthefactorsrelatedtosurgery, suchasinfectionanddruguse,forexample.Intherat intes-tineit isnotyetwelldefinedwhatthistimewould be,but theresultsobtainedhereshowedthatat21daystherewas nodifferenceintensilestrengthbetweenthestudied materi-als,provingthatbothareeffectivewiththesameintensityin maintainingtheintegrityoftheanastomosisuntilthisperiod. Astherewasgreaterfibrosiswithpolyglactin,onecouldexpect greater resistancethan with polydioxanone,which didnot happen,thatis,greaterfibrosisdoesnotmeangreater pro-tectionagainstdehiscence.13
Werraetal.14 hadcompareddifferentthreadsin
intesti-nal anastomoses of rats, among them polydioxanone and polyglactin, and found no important differences in the histopathologicalstudy,however, usingdifferentevaluation periodsthanthoseusedhere.Consideringthescarcityof pub-licationsonthesubjectanditsgreatrelavance,considering thathand-sewnanastomosisisstillpracticedonalargescale, studiesshouldbecarriedoutinthisdirection.
Conclusion
Polydioxanonecausedlessfibrosisthanpolyglactinin intesti-nalanastomosesofrats.Therewasnodifferencebetweenthe studiedthreadsasregardstensilestrength.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. FernandesLC,MatosD,NovelliMD,KimSB.Comparative studyofintestinalanastomosiswithmanualsutureand biofragmentableringindogsundercorticosteroid administration.RevAssocMedBras.2000;46:113–20. 2. ConnelME.Anexperimentalcontributionlookingtoan
improvedtechniqueinenterorraphy,wherebythenumberof knotsisreducedtotwo,orevenone.MedRec.1982;42:335–7. 3. BarrosM,GorgalR,MachadoAP,CorreiaA,MontenegroN.
Surgicalbasicskills:surgicalsutures.ActaMedPort. 2011;24:1051–6.
4. JiangHP,LinLL,JiangX,QiaoHQ.Meta-analysisof hand-sewnversusmechanicalgastrojejunalanastomosis duringlaparoscopicRoux-en-Ygastricbypassformorbid obesity.IntJSurg.2016;32:150–7.
5.KayaniB,GarasG,ArshadM,AthanasiouT,DarziA, ZacharakisE.Ishand-sewnanastomosissuperiortostapled anastomosisfollowingoesophagectomy.IntJSurg. 2014;12:7–15.
6.GarudeK,TandelC,RaoS,ShahNJ.Singlelayeredintestinal anastomosis:asafeandeconomictechnique.IndianJSurg. 2013;75:290–3.
7.Bernis-FilhoWO,WoutersF,WoutersAAP,BernisVMO,Lopes LR,AndreoloNA.Comparativestudyofcotton,polyglactin andpolyglecapronesuturesinintestinalanastomosesin dogs.ABCDArqBrasCirDig.2013;26:18–26.
8.GolubR,GolubRW,CantuR,SteinHD.Amultivariateanalysis offactorscontributingtoleakageofintestinalanastomoses.J AmCollSurg.1997;184:364–72.
9.García-OsogobioSM,Takahashi-MonroyT,VelascoL,Gaxiola M,Sotres-VegaA,Santillán-DohertyP.Single-layercolonic anastomosesusingpolyglyconate(Maxon)vs.two-layer anastomosesusingchromiccatgutandsilk.Experimental study.RevInvestClin.2006;58:198–203.
10.HolznerP,KulemannB,SeifertG,GlatzT,ChikhladzeS, HöppnerJ,etal.Double90degreescounterrotated end-to-end-anastomosis:anexperimentalstudyofan intestinalanastomosistechnique.EurJPediatrSurg. 2015;25:269–76.
11.González-ContrerasQH,Jesús-MossoM,Bahena-AponteJA, Aldana-MartínezO,Pineda-SolísK,Mejia-ArcadiaSN. Colorectalanastomosisusingacompressiondevice.CirCir. 2016;84:482–6.
12.NeutzlingCB,LustosaSA,ProencaIM,SilvaEM,MatosD. Stapledversushandsewnmethodsforcolorectalanastomosis surgery.CochraneDatabaseSystRev.2012;15:CD003144. 13.DuellJR,ThiemanMankinKM,RochatMC,RegierPJ,SinghA,
LutherJK,etal.Frequencyofdehiscenceinhand-suturedand stapledintestinalanastomosesindogs.VetSurg.
2016;45:100–3.