Braz. Dent. J. vol.25 número3
Texto
Imagem
Documentos relacionados
Remelted zone of the probes after treatment with current intensity of arc plasma – 100 A, lower bainite, retained austenite and secondary cementite.. Because the secondary
The development of comprehensive care services for young persons and adolescents continues to be promoted. Among the activities under- taken, mention may be made
7. Mental hygiene classes shall be included in the program to assist in protecting the child against mental and physical diseases. Mentally deficient children and those
Aim: This prospective cohort study was to evaluate the independent and mutual effects of socioeconomic, oral health behaviors and individual clinical factors, including
Abstract: This cross-sectional study assessed the impact of Developmen- tal Enamel Defects (DED) on Child Oral Health-Related Quality of Life (COHRQoL).. The children completed
resentative sample of 12-year-old Brazilian children, we assessed the inluence of socioeconomic factors and self-rated oral health on the utilization of dental health
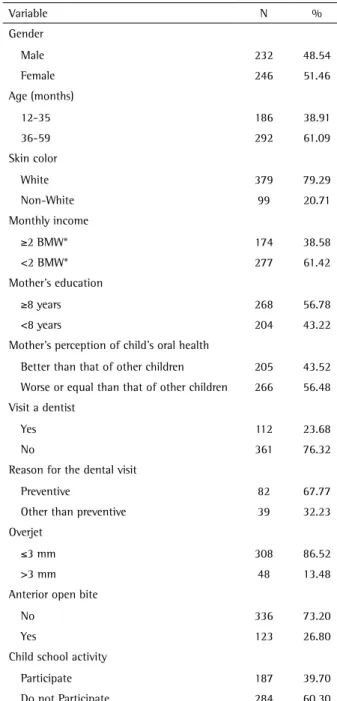
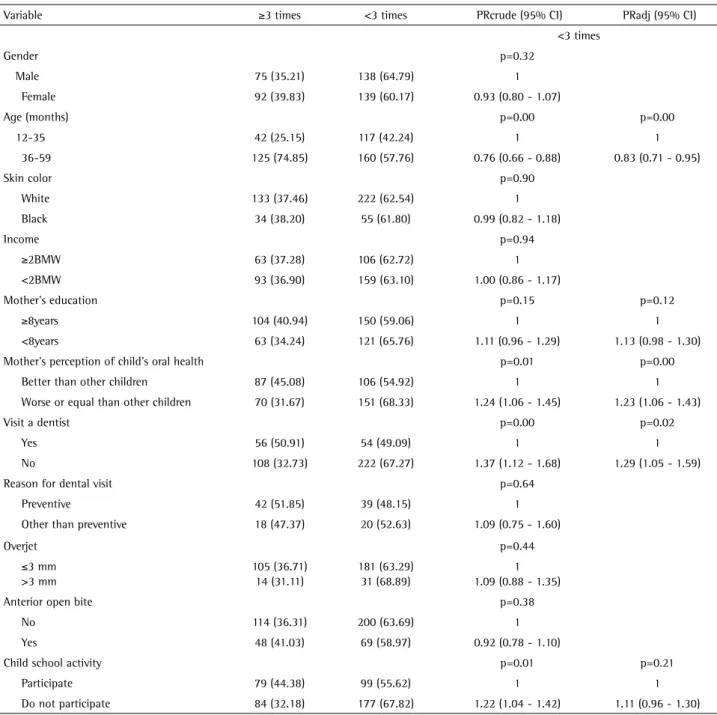
The aim of this study was to assess the impact of socioeconomic factors and clinical conditions on the child oral health-related quality of life (COHRQoL) of preschool
The objective of this study was to evaluate the influence of the socioeconomic level on oral health conditions and infantile growth in preschool children.. The targets of this
