RevBrasAnestesiol.2014;64(5):365---368
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
CLINICAL
INFORMATION
The
development
of
ventricular
fibrillation
due
to
etomidate
for
anesthetic
induction:
a
very
rare
side
effect,
case
report
Murat
Karcioglu
a,∗,
Isil
Davarci
a,
Nuray
Kirecci
a,
Adnan
Burak
Akcay
b,
Selim
Turhanoglu
a,
Kasim
Tuzcu
a,
Sedat
Hakimoglu
a,
Seckin
Akkucuk
c,
Akin
Aydogan
caDepartmentofAnesthesiologyandReanimation,FacultyofMedicine,MustafaKemalUniversity,Hatay,Turkey bDepartmentofCardiology,FacultyofMedicine,MustafaKemalUniversity,Hatay,Turkey
cDepartmentofGeneralSurgery,FacultyofMedicine,MustafaKemalUniversity,Hatay,Turkey
Received28February2013;accepted10June2013 Availableonline16October2013
KEYWORDS
Etomidate; Inductionof anesthesia; Ventricular fibrillation
Abstract
Backgroundandobjectives: Ventricularfibrillationoccurringinapatient canresultin unex-pectedcomplications. Here,ouraimistopresentacaseofventricularfibrillationoccurring immediatelyafteranesthesiainductionwithetomidateadministration.
Casereport: Afifty-six-year-oldfemalepatientwithapre-diagnosisofgallstoneswasadmitted totheoperatingroomforlaparoscopiccholecystectomy.Theinductionwasperformedby eto-midatewithabolusdoseof0.3mg/kg.Severeandfastadductionappearedinthepatient’sarms immediatelyafterinduction.AtachycardiawithwideQRSandventricularrate188beat/min wasdetected onthemonitor.TherhythmturnedtoVFduringthepreparationof cardiover-sion.Immediatelywe performeddefibrillationtothepatient.Sinusrhythmwasobtained.It wasdecidedtopostponetheoperationduetothepatient’sunstablecondition.
Conclusion: Inadditiontootherknownsideeffectsofetomidate,veryrarely,ventricular tachy-cardia andfibrillationcan bealsoseen.Tothebestofourknowledge, thisisthefirstcase regardingetomidatecausingVFintheliterature.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Etomidato;
Induc¸ãodaanestesia; Fibrilac¸ãoventricular
Desenvolvimentodefibrilac¸ãoventricularporcausadeetomidatoparainduc¸ão anestésica:umefeitocolateralmuitoraro,relatodecaso
Resumo
Justificativaeobjetivos: Aocorrênciadefibrilac¸ãoventricularemumpacientepoderesultar em complicac¸õesinesperadas.Nossoobjetivoéapresentarumcasodefibrilac¸ãoventricular queocorreuapósainduc¸ãoanestésicacomadministrac¸ãodeetomidato.
∗Correspondingauthor.
E-mail:[email protected](M.Karcioglu).
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
366 M.Karciogluetal.
Relatodecaso:Pacientedosexofeminino,56anos,compré-diagnósticodecálculosbiliares, foiadmitidanasaladecirurgia paracolecistectomialaparoscópica. Aanestesiafoiinduzida comaadministrac¸ãodeetomidatocomuma doseembolusde0,3mg/kg. Apaciente apre-sentouumagraveerápidaaduc¸ãodosbrac¸oslogoapósainduc¸ão.TaquicardiacomQRSlargo efrequênciaventricularde188bpmforamdetectadasnomonitor.Oritmoconverteu-seem fibrilac¸ãoventricular(FV)duranteapreparac¸ãoparaacardioversão.Apacientefoi imediata-mente submetidaadesfibrilac¸ão.Oritmo sinusalfoi obtido.Decidimosadiaracirurgia por causadacondic¸ãodeinstabilidadedapaciente.
Conclusão:Alémdosefeitos secundáriosconhecidosdeetomidato, taquicardiaventriculare fibrilac¸ão,emboramuitoraramente,tambémpodemserobservadas.Atéondesabemos,esse éoprimeirocasonaliteraturadeFVcausadoporetomidato.
©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Ventricularfibrillation(VF)isacardiacpathologyinwhich theventricleis completely chaoticand does notcontract effectively.VFcancauseveryseriousendpoints.Etomidate isahypnoticagentthathasastablecardiovascularprofile andresultsinminimalrespiratorysideeffects.Forthis rea-son,itiscommonlypreferredfortheinductionofanesthesia inhemodynamicallyunstablepatients.1
The reported side effects related to etomidate are myoclonus,vomiting,painoninjectionsite,and adrenocor-ticalsuppression.2
Inrarecases,otheradverseeffectsregardingetomidate havebeen mentioned.Inthe currentreport,we aimedto presentacaseinwhichVFdevelopedduringinductionwith etomidateinapatientunderwentlaparoscopic cholecystec-tomy due to gallstones.In the literature, this is the first reportinvestigatingthisassociation.
Figure1 PreanestheticECGImage.
Case
report
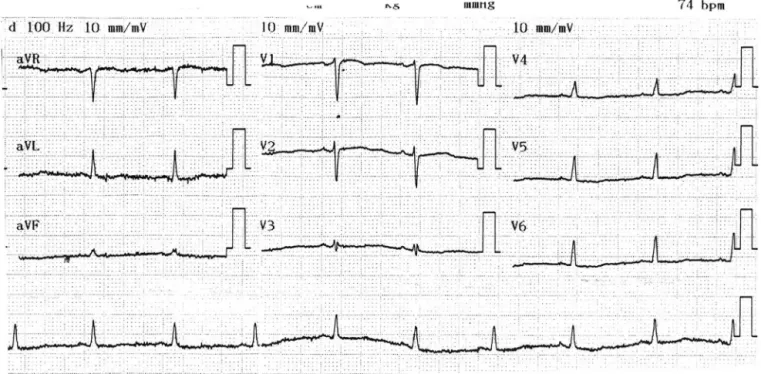
A fifty-six-year-old female patient with a pre-diagnosis of gallstones was admitted to the operating room for laparoscopic cholecystectomy. The patient’s history of hypertension with the irregular use of an antihyperten-sivedrugwasknownduringthepre-anesthesiaevaluation. Routine biochemical and hematological tests were nor-mal. ECG wasin normal sinus rhythm (Fig.1), heart rate was74beats/min,PAchest X-raywasnormal,and consid-ered ASA II. The patient was monitored, and the initial arterial blood pressure (BP): 140/110mmHg, heart rate: 118beats/min,presenceof sinus tachycardia rhythm,and peripheraloxygensaturation(SpO2):98%weredetected.
Thedevelopmentofventricularfibrillationduetoetomidate 367
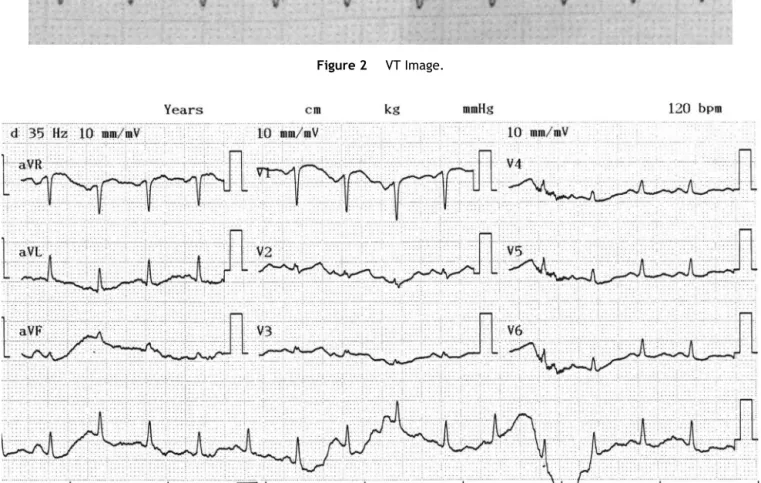
Figure2 VTImage.
Figure3 PostextubationECGimage.
movementswereconsideredtobeduetoetomidateanda doseof0.6mg/kgrocuronium(Esmeron®N.V.OrganonOss, Netherlands)wasgiven.Atthistime,BPwas150/110mmHg, SpO2was98%,heartratewas110---130beats/min,andthe heart rate increased gradually. A tachycardia with wide QRS and ventricular rate 188beat/min was detected on themonitor(Fig.2).Bloodpressurewasseenasdecreased to 90/60mmHg. The rhythm turned to VF during the preparation of cardioversion. Immediately we performed defibrillation to the patient (biphasic shock with 200J). Sinusrhythmwasobtained.Wedecidedtogiveamiodarone tothepatienttoavoidrecurrentVT.
A150mgofIVamiodarone(Cordarone® MefarIstanbul, Turkey)loadingdosewasappliedwithin15minandwas fol-lowedbymaintenancetherapy.Itwasdecidedtopostpone theoperationduetothepatient’sunstablecondition.
Anesthesia was maintained with oxygen, air, sevoflu-rane(Sevorane®AbbottLaboratoriesLtd.,UK)andfentanyl (Fentanyl® Janssen N.V., Belgium). Thirty-seven minutes after the induction of anesthesia, the patient started to breathe spontaneously and extubation was proposed. The patient was extubated and admitted to the inten-sive care unit (ICU). A cardiology consultation was made in ICU. On patient echocardiography, Left ventricle (LV)
diameters were normal, systolic function was adequate, Left atrium (LA)dilatation was(4.1cm), 1+ mitral regur-gitation and 2---3+ tricuspid regurgitation were noted, pulmonary hypertension was present (35---40mmHg), and ejectionfraction (EF) wasevaluated as63%. Sinus tachy-cardia (120beats/min) and nonspecific ST changes in the patient’sECG(Fig.3)werefoundbythecardiologists. Hema-tological,biochemical, thyroid function tests werewithin normallimits.
The patient was discharged after threedays following upintheICU.Twoweekslater,thepatientwasadmittedfor thelaparoscopiccholecystectomy.Thepatientwasoperated withoutanycomplication,withtheinductionbythiopental, fentanylandrocuronium,andsenthome.
Discussion
368 M.Karciogluetal.
Encounteringunpredicteddisordersarecommonduring anesthesiainduction, themaintenance ofanesthesia, and awakening from anesthesia. In this case, we reported a process of ventricular tachycardia and fibrillation occur-ring immediately after the induction of anesthesia with etomidate.The well-knownside effects of etomidate are myoclonus, pain on injection site, and adrenal suppres-sion. The mechanism of myoclonus is not clear, though it is a form of seizure activity. High doses of etomidate depress cortical activity before than subcortical activity, andresearchers have proposed thatthis is a disinhibition phenomenon.3,4Subcorticalneuronalactivityinhibitordrugs
suchasbenzodiazepines andopioidspreventthe develop-mentofmyoclonus.5
Etomidateinjectionhassideeffectsintermsofpainand myoclonusbecauseitisformulatedwithpropyleneglycol.6,7
However,analternatepharmaceuticalformulationexiststo reducethepainofinjection.Inthisnewformulation, etomi-dateisdissolvedinafatemulsioncomposedofmediumand longchaintriglycerides.8Inastudy,usingonlyasinglebolus
dose of etomidatecause adrenal dysfunctionin aspect of hypocortisolemia.9Thisimpairedfunctionresultsina
tran-sientandclinicallyinsignificanteffectonadrenalgland.7,9
Insomecases,adrenaldysfunctioncanbeveryimportant. Thereforepractitionersmustbeawareof thisinformation regardingthedrug.
Case reports related to adrenal adverse effects with etomidateare common.However, the cardiovascularside effects are found in only one report associated with the drug. Etomidate typically does not alter myocardial con-tractility and cardiac output.10 Fideler et al. reported a
caseofthyrotoxicosisoccurringafterapplyingamiodarone treatment to a patient with heart failure and suffering fromatrialfibrillationforthefirsttime.Thyroidectomywas plannedwhenhyperthyroidismwasunresponsivetomedical treatment.Thestaffnoteddecreasedbloodpressureafter inductionwithetomidate,sufentaniland rocuronium,and norepinephrineinfusionwasstartedbeforethepatienthad VFfollowedby cardiacarrest.11 Inourcase, thepatient’s
thyroidfunctiontests werenormaland nosignificant car-diacpathologywasdetectedexceptforthedevelopmentof sinus tachycardia anda slightrise in blood pressureprior toinductionintheoperatingroom.Theinjectionof etomi-datewasconsideredtobetheonlyprobableetiologyforthe developmentofVTandVF.
WhenetomidateandVFwereinvestigatedusingtheFDA Adverse Event Reporting System (FAERS), a total of 4 VF eventshadbeenreportedforetomidate.12
According toanothersource, 1023cases of etomidate-relatedadverseeffectshavebeenfound.Amongthem,VF wasreportedin23patients(2.25%).Ofthesecases,72.7% werefemales,27.3%weremales,22.7%wereintherange of 0---1 years old,13.6% in the rangeof 20---29 years old,
4.5%intherangeof30---39yearsold,27.3%intherangeof 50---59yearsold,31.8%percentovertheageof60years.The drugsusedinthesepatientswithVFwereSufentanilcitrate, Propofol, Fentanyl,Rocuroniumbromide, andAmiodarone HCL.13
Asaresult,itis suggestedthat thedevelopmentof VF inthiscase, aftertheexclusionoftheprobable etiologies may bedue totheinduction withetomidate. To thebest ofourknowledge,thisisthefirstcaseregardingetomidate causing VFin theliterature.We aimedtoreportthat fol-lowinginductionwithetomidateVFcanoccurinrarecases, andearlydiagnosisandimmediateinterventionwithclose follow-uparerequiredtoachievepositiveoutcomesinthese patients.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
References
1.GultopF,AkkayaT, Bedirli N,et al. Lidocainepretreatment reducesthefrequencyandseverity ofmyoclonusinducedby etomidate.JAnesth.2010;24:300---2.
2.RuthWJ,BurtonJH,BockAJ.Intravenousetomidatefor proce-duralsedationinemergencydepartmentpatients.AcadEmerg Med.2001;8:13---8.
3.DoenickeAW, RoizenMF,KuglerJ,etal.Reducingmyoclonus afteretomidate.Anesthesiology.1999;90:113---9.
4.ReddyRV,MoorthySS,DierdorfSF,etal.Excitatoryeffectsand electroencephalographiccorrelationofetomidate,thiopental, methohexital,andpropofol.AnesthAnalg.1993;77:1008---11.
5.Modica PA,Tempelhoff R, White PF. Pro- and anticonvulsant effectsofanesthetics(PartII).AnesthAnalg.1990;70:433---44.
6.DoenickeAW,RoizenMF,HoerneckeR,etal.Solventfor eto-midate may cause pain and adverse effects. Br J Anaesth. 1999;83:464---6.
7.Nyman Y,Von Hofsten K, PalmC,et al. Etomidate-Lipuro is associated with considerably less injection pain in children comparedwithpropofolwithaddedlidocaine.Br JAnaesth. 2006;97:536---9.
8.CameronE,JohnstonG,CroftsS,etal.Theminimumeffective doseoflignocainetopreventinjectionpainduetopropofolin children.Anaesthesia.1992;47:604---6.
9.KulstadEB,KalimullahEA,TekwaniKL,etal.Etomidateasan inductionagent insepticpatients: redflags orfalsealarms? WestJEmergMed.2010;11:161---72.
10.MorganGE,MichaelSM,MurrayJM,etal.Clinical anesthesiol-ogy.3rded.NewYork:McGrawHill;2002.
11.FidelerFJ,DieterichHJ,SchroederTH.Fataloutcomeduring anaesthesiainduction ina patient withamiodarone-induced thyrotoxicosis.EurJAnaesthesiol.2008;25:337---9.
12.Drugcite.SeedrugsideeffectsreportedtotheFDAbypeople likeyou.