w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Acute
lymphoblastic
leukemia
in
children
and
adolescents:
prognostic
factors
and
analysis
of
survival
Daniel
Willian
Lustosa
de
Sousa
a,∗,
Francisco
Valdeci
de
Almeida
Ferreira
a,
Francisco
Helder
Cavalcante
Félix
b,
Marcos
Vinicios
de
Oliveira
Lopes
aaUniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil bHospitalInfantilAlbertSabin(HIAS),Fortaleza,CE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15November2014 Accepted7January2015 Availableonline14April2015
Keywords:
Leukemia Lymphoid Child Adolescent Survival
a
b
s
t
r
a
c
t
Objective:Todescribetheclinicalandlaboratoryfeaturesofchildrenandadolescentswith acute lymphoblastic leukemia treated at three referral centers in Cearáand evaluate prognosticfactorsforsurvival,includingage,gender,presentingwhitebloodcellcount, immunophenotype,DNAindexandearlyresponsetotreatment.
Methods:Seventy-sixunder19-year-oldpatientswithnewlydiagnosedacutelymphoblastic leukemiatreatedwiththeGrupoBrasileirodeTratamentodeLeucemiadaInfância–acute lymphoblasticleukemia-93and-99protocolsbetweenSeptember2007andDecember2009 wereanalyzed.Thediagnosiswasbasedoncytological,immunophenotypicand cytoge-neticcriteria.Associationsbetweenvariables,prognosticfactorsandresponsetotreatment wereanalyzedusingthechi-squaretestandFisher’sexacttest.Overallandevent-free sur-vivalwereestimatedbyKaplan–Meieranalysisandcomparedusingthelog-ranktest.ACox proportionalhazardsmodelwasusedtoidentifyindependentprognosticfactors.
Results:Theaverageageatdiagnosiswas6.3±0.5yearsandmaleswerepredominant(65%). Themostfrequentlyobservedclinicalfeatureswerehepatomegaly,splenomegalyand lym-phadenopathy.Centralnervoussysteminvolvementandmediastinalenlargementoccurred in6.6%and11.8%,respectively.B-acutelymphoblasticleukemiawasmorecommon(89.5%) thanT-acutelymphoblasticleukemia.ADNAindex>1.16wasfoundin19%ofpatientsand wasassociatedwithfavorableprognosis.OnDay8ofinductiontherapy,95%ofthepatients hadlymphoblastcounts<1000/Landwhitebloodcellcounts<5.0×109/L.Theremission
inductionratewas95%,theinductionmortalityratewas2.6%andoverallsurvivalwas72%.
Conclusion: Theprognosticfactorsidentifiedarecompatiblewiththeliterature.The5-year overallandevent-freesurvivalrateswerelowerthanthosereportedfordeveloped coun-tries.Asshownbythemultivariateanalysis,ageandbaselinewhitebloodcellcountwere independentprognosticfactors.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:RuaCapitãoFranciscoPedro,1290,HematologiaSala41,RodolfoTeófilo,60430-370Fortaleza,CE,Brazil. E-mailaddress:[email protected](D.W.L.d.Sousa).
http://dx.doi.org/10.1016/j.bjhh.2015.03.009
Introduction
Acute lymphoblastic leukemia (ALL) is the most common malignancy in children and represents 75–80% of acute leukemiainthisagegroup.TheincidenceofchildhoodALL is3–4casesper100,000inunder15-year-oldchildren.Despite affectingchildrenofallages,theincidencepeaksbetweentwo andfiveyearsofage,withaslightpredominanceamongboys.1 ALLisaheterogeneousdisease;subtypesdifferwithregard tobiological,cellularandmolecularcharacteristics,response totherapyandriskofrelapse,andareassociatedwithdifferent outcomes.2
ThesurvivalrateofpediatricALLpatientshasimprovedto approximately90%inrecentyears,especiallyforgroupswith goodprognosis.Thisprogressismainlyduetotheadoptionof modificationsintherapybasedonpatients’individual phar-macodynamicsandpharmacogenomics,risk-adaptedtherapy andimprovedsupportivecare.2,3
Stratificationintoriskgroupsisbasedonarangeof clini-cal,biologicalandgeneticfeatures,suchasageandgender, white blood cell (WBC) countat diagnosis, immunopheno-typic, cytogenetic and molecular characteristics, and early medullarresponsetoinductiontherapy.4–6Earlyresponseto therapydeterminedbythelevelofminimalresidualdisease (MRD)attheendofinductioniscurrentlythemostimportant prognosticfactorinpatientswithALL.7
Theidentificationofprognosticfactors,animproved strat-ificationof riskgroups and survivalanalysis havemade it possibleto identifypresenting featuresof the disease and evaluate treatment outcome in referral centers in Ceará, therebycontributingtocurrentknowledgeofthe epidemiol-ogyofpediatricmalignancies,bothlocallyandthroughoutall Brazil.
The purpose of this study was to describe the clinical andlaboratoryfeaturesofchildrenandadolescentswithALL treatedatthreereferralcentersinthestateofCeará,Braziland evaluateprognosticfactorsforsurvival,includingage,gender, presentingWBCcount,immunophenotype,DNA indexand earlyresponsetotreatment.
Methods
Thisprospectivestudy wasbasedon asampleof76under 19-year-oldpatientswithnewlydiagnosedALLtreatedwith the GrupoBrasileiro de Tratamento deLeucemia da Infân-cia–acutelymphoblasticleukemia (GBTLI-ALL)-93protocol (n=64)ortheGBTLI-ALL-99protocol(n=12)between Septem-ber 2007and December 2009.Patients were treated atthe pediatriconcologyservicesofHospitalInfantilAlbertSabin (HIAS),HospitaldoCâncerHaroldoJuac¸aba(HC)andHospital LuisFranc¸a(HLF).HIASandHCarepublicreferralhospitals providingtreatment ofchildhood cancerin Ceará. All par-entsand/orpatientsgavetheirwritteninformedconsent.The studywasapprovedbytheResearchEthicsCommitteesofHC (Protocol66/2007)andHIAS(Protocol058/08).
The observedclinical variables included age at diagno-sis,gender,hepatomegaly,splenomegaly,lymphadenopathy, mediastinalmass,infiltrationofthecentralnervoussystem
(CNS), WBC count, hemoglobin and lactate dehydrogenase (LDH) levels, platelet count, immunophenotype and DNA Index(DI).
Treatmentresponsewasevaluatedbasedonthe present-ingWBCcount,thelymphoblastcountontheeighthdayof inductiontherapy(Day8),andbonemarrow(BM)analysison Day28ofinduction.
ALLwasdiagnosedinpatientswith≥25%lymphoblastsin BM(basedonmorphologicalandcytochemicalevaluationsof BMsmears)andpositivityinimmunophenotypingand cytoge-netics.TheDIwasdeterminedbyflowcytometry.Peripheral blood,bonemarrowandcerebrospinal fluid(CSF) were col-lectedatreferralhospitals.
CNS involvement was diagnosed in patients with >5 WBC/LinCSFandlymphoblastsidentifiedonthe
cytocen-trifugeslide.
AccordingtotheGBTLIriskcriteria,riskofrelapse(lowvs. high)wasstratifiedbasedonage,WBCcountatdiagnosisand earlyresponsetotherapy.Thefollowingpretreatment char-acteristicswereobservedinhigh-riskpatients:agelessthan one,agegreaterthannine,WBC>50.0×109cells/L,and lym-phoblastcount>1000cells/LorWBCcount>5.0×109cells/L
on Day 8. All other patients were classified as low riskof relapse.8,9
Statisticalanalysis
The statisticalanalysis was carried out using the R statis-ticallanguageversion2.1.10Descriptivestatisticswereused tocharacterizethepatients.Associationsbetweenvariables, prognosticfactorsandresponsewereanalyzedwiththe chi-squaretestandFisher’sexacttest.Five-yearoverallsurvival (OS)andevent-freesurvival(EFS)rateswereestimatedwith the Kaplan–Meiermethodandcomparedwiththe log-rank test.TheCoxproportionalhazardsmodel11wasusedto iden-tifyindependentprognosticfactorswithrespecttoEFSand OS.Thelevelofstatisticalsignificancewassetat5%(p-value <0.05).
Results
Theclinicalandlaboratoryfeaturesatdiagnosisforthis sam-pleof76patientsaresummarizedinTables1and2.Lowand high risk ofrelapse wasattributedto 54% (n=41) and 46% (n=35)ofthesample,respectively.
The average age at diagnosis was 6.3±0.5 years (median=5.3). Males (65.8%) were predominant in the sample(male/femaleratio=1.9:1).
Themostprevalentagegroupwasonetonineyears(75%). Underone-year-oldandovernine-year-oldpatientsaccounted for2.6%and22.4%,respectively.Agelessthanonewas associ-atedwithunfavorableprognosticfactors,suchaspresentinga highbaselineWBCcount,pro-BimmunophenotypeandCD10 negativity.Agebetweenoneandnineyearswasassociated withmorefavorableprognosticfactors,suchasaWBCcount <50.0×109cells/L,CD10positivityandDI>1.16.
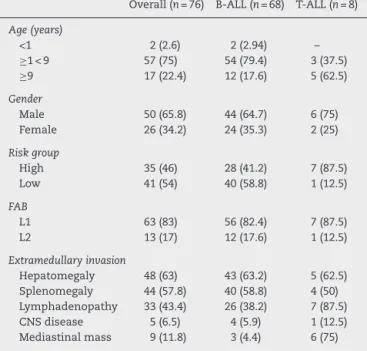
Table1–Presentingclinicalandbiological
characteristicsof76childrenandadolescentswithacute lymphoblasticleukemia(B-ALLandT-ALL)treatedat threereferralcentersinCeará,Brazil,between September2007andDecember2009.
Overall(n=76) B-ALL(n=68) T-ALL(n=8)
Age(years)
<1 2(2.6) 2(2.94) –
≥1<9 57(75) 54(79.4) 3(37.5)
≥9 17(22.4) 12(17.6) 5(62.5)
Gender
Male 50(65.8) 44(64.7) 6(75)
Female 26(34.2) 24(35.3) 2(25)
Riskgroup
High 35(46) 28(41.2) 7(87.5)
Low 41(54) 40(58.8) 1(12.5)
FAB
L1 63(83) 56(82.4) 7(87.5)
L2 13(17) 12(17.6) 1(12.5)
Extramedullaryinvasion
Hepatomegaly 48(63) 43(63.2) 5(62.5) Splenomegaly 44(57.8) 40(58.8) 4(50) Lymphadenopathy 33(43.4) 26(38.2) 7(87.5)
CNSdisease 5(6.5) 4(5.9) 1(12.5)
Mediastinalmass 9(11.8) 3(4.4) 6(75)
Valuesareexpressedinabsolutenumbersofpatientswithcertain characteristics(percentagerelativetothetotalnumberofpatients intheirsubgroupinparentheses).FAB:French-American-British; CNS:centralnervoussystem.
and mediastinal mass were observed in 6.6% and 11.8%, respectively.
Anemiawasdiagnosedin85%ofthepatients,35%ofwhom hadsevereanemia(Hb<7g/dL);themean hemoglobinlevel was 8.24g/dL. Atdiagnosis, patients with T-ALL presented significantlyhigherHb levels(10.6±2.45g/dL)thanpatients withB-ALL(7.9±2.55g/dL;p-value=0.011).Aplatelet count <100.0×109cells/Lwasobservedin65%,and10.5%hadsevere thrombocytopeniawithplateletcounts<20.0×109cells/L.The averageWBCcountatdiagnosis was31.8±53.4×109cells/L (range: 0.9–320.0×109cells/L). Sixteen patients (21%) were classifiedashighriskofrelapse(WBCcount>50.0×109cells/L) (Table 2). In 4%, the peripheral blood cell count was nor-malatdiagnosis,withnochangesinhemoglobinlevel,WBC orplatelet countsand nolymphoblastsinperipheralblood smears.
LDH >1000U/L was used as a prognostic marker (nor-mal:480U/L).Thus,39patients(51.3%)presentedLDHlevels >1000U/L(mean:1506.43±1194.03U/L)(Table2).
BimmunophenotypeALLwasidentifiedin89.5%.Themost prevalent subtypes were common B-ALL (51.5%)and pre-B (45.5%).Pro-Bwasfoundinabout3%ofcases.Patientswith matureBorFrench-American-British(FAB)classificationofL3 werenotincludedinthisstudy.
TimmunophenotypeALLwasfoundin10.5%.Themost prevalentEuropeanGroupfortheImmunological Character-izationofLeukemias (EGIL)subtypes were pre-T(50%) and corticalT(37.5%).T-ALLwasassociatedwithunfavorable fac-torsincludingthefollowing:beingmale, overnineyearsin age,leukocytosis,CD10negativity,mediastinalmass,andCNS involvement(Table1).
DI was determined by flow cytometry in 58 patients. Overall, 76% were diploid (DI=1) and 24% were hyper-diploid (DI>1.0).Observedin 19%,DI >1.16 wasassociated with low riskof relapse and favorable factors suchas age betweenoneandnineyears,WBCcount<20.0×109cells/L(p -value=0.028),Bimmunophenotype,and100%CD10positivity (Table3). Thesepatients respondedwell toinduction ther-apy(onDay 8,lymphoblastcount<1000/LandWBCcount
<5.0×109cells/L),withcompletehematologicalremissionand absenceofearlyrelapse.OutcomeaccordingtoDIshowedthat patients withDI >1.16 fared better(5-yearEFS:100%)than patientswithDI<1.16(5-yearEFS:66%;p-value=0.03).
The median follow-up was 60 months. Seventy-two patients(95%)achievedcompleteremission.OnDay 8,95% ofthepatientshadalymphoblastcount<1000/LandWBC
count <5.0×109cells/L.Twelve (16%) patients relapsed and two(2.6%)diedduringinduction.
EFSforall76patientswas71.2±5.2%[95%confidence inter-val(95%CI):62.1–82.8%]and5-yearOSwas72±5.24%(95%CI: 62–82%),withhigherEFSratesinthelow-riskgroup(83%;95% CI:72–95%)andinpatientswithB-ALL(73%;95%CI:63–85%) (Figure1AandB).
AgeatdiagnosisandpresentingWBCcountwere statis-tically significant prognosticfactors. Thehighest EFSrates were observed in children aged one to nine years (73%; 95%CI:63–85%)andinpatientswithpresentingWBCcount <50.0×109cells/L(73%;95%CI:63–85%)(Figure1CandD).
Inthemultivariateanalysis,ageatdiagnosis,presenting WBCcountandlymphoblastcountonDay8remained statis-ticallysignificantwithregardtoriskofrelapseafteradjusting forgender,riskgroup,CD10expression,andearlyresponseto therapy(Table3).
Table2–Baselinelaboratorycharacteristicsof76childrenandadolescentswithacutelymphoblasticleukemia(B-ALL andT-ALL)treatedatthreereferralcentersinCeará,Brazil,betweenSeptember2007andDecember2009.
Overall(n=76) B-ALL(n=68) T-ALL(n=8)
Hemoglobin(g/dL) 8.24±2.68 7.9±2.55 10.8±2.45
WBC×109cells/L 31.77±53.35 24.30±4.80 95.25±36.31
Platelets×109cells/L 109.80±122.92 109.97±123.16 108.38±129.34
LDHlevel(U/L) 1506.43±1194.03 1458.50±140.5 1913.88±524.17
CD10positivityn(%) 72(95) 66(97.1) 2(25)
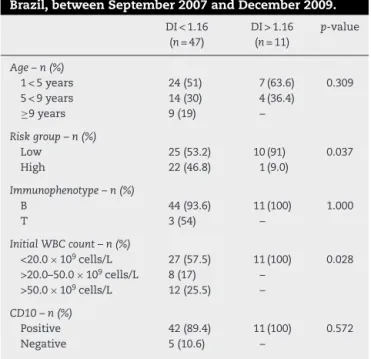
Table3–CharacteristicsaccordingtoDNAploidyof76 childrenandadolescentswithacutelymphoblastic leukemiatreatedatthreereferralcentersinCeará, Brazil,betweenSeptember2007andDecember2009.
DI<1.16 (n=47)
DI>1.16 (n=11)
p-value
Age–n(%)
1<5years 24(51) 7(63.6) 0.309
5<9years 14(30) 4(36.4)
≥9years 9(19) –
Riskgroup–n(%)
Low 25(53.2) 10(91) 0.037
High 22(46.8) 1(9.0)
Immunophenotype–n(%)
B 44(93.6) 11(100) 1.000
T 3(54) –
InitialWBCcount–n(%)
<20.0×109cells/L 27(57.5) 11(100) 0.028 >20.0–50.0×109cells/L 8(17) –
>50.0×109cells/L 12(25.5) –
CD10–n(%)
Positive 42(89.4) 11(100) 0.572
Negative 5(10.6) –
Valuesareexpressedinabsolutenumbersofpatientswithcertain characteristics(percentagerelativetothetotalnumberofpatients intheirsubgroupinparentheses).
DI:DNAIndex.
Thecomparisonofrelativeriskrevealedthattheriskwas higherforpatientswithWBCcounts>50.0×109cells/Lat diag-nosis(HR=589;95%CI:7–4757).ThewiderangeoftheCIisdue totherelativelysmallnumberofpatientswithelevatedWBC counts(n=16).Theotherprognosticfactors(ageandnumber oflymphoblastsonDay8)hadarelativeriskbetween0.2and 1.0,withawidevariationof95%CI,indicatingaweaker influ-enceonOS.Thesameprognosticfactorswereassociatedwith EFS,withrelativerisksofthesamemagnitude.
Discussion
Littlehasbeenpublishedontheepidemiologyofchildhood andjuvenileALL inNortheasternBrazil.Thepresent study looksintotheepidemiologicalandclinicalaspects,prognostic factorsandresponsetotherapyofchildrenwithALLtreated atreferralcentersinthestateofCeará.
Theageofourpatientswassignificantlycorrelatedwith prognosis.Thus,under1-year-oldinfantsandpatientsolder thanninepresentedpoorerprognoses.Infancywasassociated withunfavorableprognosticfactorssuchashighpresenting WBCcount,Pro-Bimmunophenotype,CD10negativity, hep-atosplenomegalyandpoorresponsetoinductiontreatment, thusmatchingfindingsintheliterature.12
Overnine-yearoldchildrenandadolescentsaccountedfor 22.4%ofthecasesinthisstudy.Historically,adolescentsand youngadultshavehigherrelapseratesandshortersurvival thanchildrenagedonetonine years.Theworseoutcomes in this group may be due to the high prevalence of bio-logically high-risk leukemia (e.g. breakpoint cluster region
protein-Abelson murine leukemia viral oncogene homolog 1 [BCR-ABL1]and mixed-lineageleukemia [MLL] rearrange-ments)inassociationwithunfavorablefactorssuchashigh WBCcount,T-cellimmunophenotype,andpooradherenceto andtoleranceoftherapy.13,14
Recent studies haveshown that adolescents and young adultshavebetteroutcomesandhigherratesofcontinuous remissionwhentreatedaccordingtopediatricprotocolswith higherdosesofnon-myelosuppressivedrugs,ratherthanwith adultregimens.14,15
Males were predominantinthe presentstudy matching thefindingsofBrazilianstudiesfromBahia,16Pernambuco,17 and RioGrandedoSul,18 andthe GBTLI-ALL-99 protocol.19 In two studies, males with low EFS rates had unfavorable prognoses.19,20
Hepatomegaly,splenomegalyandlymphadenopathy,fever andsevereanemiawerethemostfrequentlyobserved clini-calfeaturesinthisstudyasinotherpublishedreports.1CNS involvementoccurredin6.6%ofthepatients.Thisis consis-tentwiththerate(6.7%)reportedinBahia,16 andelsewhere in the world (0.6–12.4%).21 The GBTLI-ALL 93 protocol and theGBTLI-ALL99protocolyieldedlowerrates(1.7%and2.4%, respectively).8,9
Anemiaoccurredin85%ofthepatientsinthecurrentstudy, mostofwhomwere normochromicandnormocytic.Severe anemia (Hb <7g/dL) was observedin35%.Patients with T-ALLpresentedsignificantlyhigherHblevelsatdiagnosisthan patients with B-ALL (mean Hb level, 10.6g/dL vs. 7.9g/dL). Accordingtosomeauthors,lowerHblevelsatdiagnosisare associatedwithmoreadvanceddisease.22
Platelet counts <20.0×109cells/L were found in 10.5%. Despitetheincreasedriskofbleeding;noseverebleedingwas observedinoursample.
WBCcountatdiagnosis>50.0×109cells/Lwasregistered in21% ofthepatients, matchinginternationalstudies that report WBCcounts>50.0×109cells/L inapproximately 20% of cases.21 Patients with severe leukocytosis at diagnosis may present bulky tumormass, mediastinal enlargement, hepatosplenomegalyandsignificantlymphadenopathy.This findingisusuallyassociatedwiththeunfavorable chromoso-maltranslocationst(4;11)andt(9;22).
T-ALL was observed in10.5%. Thisincidence is slightly lowerthanthoseoftheGBTLI-ALL93andGBTLI-ALL99 proto-cols(13%and14.2%,respectively)8,9butconsistentwithother nationalandinternationalstudies(7.4–16.4%).21,23
In this study, patients with T-ALL were more likely to presentunfavorable factorssuchasbeingmale,agegreater than nine years, high WBC count at diagnosis, low CD10 expression, mediastinalenlargementandCNSinvolvement (Tables 1 and 2). These results are compatible with those reportedbyGoldbergetal.23
Historically, theT-cell immunophenotypehasbeen con-sidered an adverse clinical prognostic factor in childhood ALL, althoughitseffecthasbeenreduced bycontemporary risk-adapted therapy andimproved supportivecare.23 Nev-ertheless, patientswith this immunophenotype are stillat increasedriskofinductionfailure,earlyrelapseandisolated CNSrelapse.
0 1.0
A
B
C
D
0.8
0.6
0.4
0.2
0.0
1.0
0.8
0.6
0.4
0.2
0.0
1.0
0.8
0.6
0.4
0.2
0.0 1.0
0.8
Overall survival Event-free survival
0.6
0.4
0.2
0.0
12 24 36
Months
48 60 0 12 24 36
Months
48 60
Months
0 12 24 36
Months
48 60 0 12 24 36
Months
48 60
Months Age < 9
Age > 9*
Low risk High risk
WBC count < 5x104
WBC count > 5x104**
Figure1–Kaplan–Meyerestimateofoverallsurvival(OS)andevent-freesurvival(EFS)ofchildrenandadolescentswith acutelymphoblasticleukemia.A–OSinBlackandEFSingray,with95%confidenceinterval;B–OSaccordingtoriskgroup (lowandhighrisk);C–OSaccordingtoageatdiagnosislessthanorgreaterthannineyearsold);D–OSbasedonwhite bloodcellcountatdiagnosis(lessthanorgreaterthan50×103/mm3).Medianfollow-upwas60months.Statistical
significanceinthemultivariateanalysis:*p-value<0.05;**p-value<0.01.
patientswithDI>1.16werealiveandwereincomplete remis-sionwithnoearlyrecurrence.Thesefindingsarecompatible withtheresultsofAricóetal.24andDastugueetal.,25 who foundastrongassociationbetweenhyperdiploidyand favor-ableprognosticfactorssuchasagebetweenoneandfiveyears andWBCcountatdiagnosis<20.0×109cells/L.
Inonestudy,24 the OSwas 95–96%andEFSwas 89% in patientswithDI≥1.16(correspondingto53 chromosomes). More recent investigations have shown that patients with B-ALLhyperdiploidy(58–66chromosomes) are almost com-pletelycurable.25Incontrast,hypodiploidpatientswithfewer than45chromosomes(nomorethan2%ofcases)haveapoor prognosis.
Early responsetotreatment wasdefined asa reduction inperipheralWBCsand circulating lymphoblastson Day 8 andearlybonemarrowresponseattheendofinduction(Day 28).26,27
On Day 8, 5% of our patients had lymphoblast counts >1000cells/LandWBCcounts>5.0×109cells/L.Defined as
poorresponders,thesepatientswereassociatedwith signif-icantlylowerEFSrates.Poorrespondersalsodisplayedlower EFSrates(∼45–52%)intheGBTLI-ALL-99protocol.9According toManabeetal.,patientswithnolymphoblastsinthe periph-eralbloodonDay8hadanexcellentoutcome,withover90%
survivingatfouryears.28ArecentstudybyVaghelaetal. sup-portstheprognosticvalueofperipherallymphoblastcounts onDay8ofinductiontherapy.29
Atthe endofinduction,95% ofthe patientsinthe cur-rentstudyhadachievedremission.Thisisinagreementwith Brazilianand internationalstudies thatshow acontinuous remissionrateof95–99%.9,20Inthisstudy,thebonemarrow evaluationonDay28wasperformedonlybymorphological analysis, although many authors havestressed the signifi-canceofresponsetoremissioninductiontherapyexpressed byminimalresidualdisease(MRD).7In30%ofpatientstreated accordingtotheBrazilianGBTLILLA-99study,thepresenceof MRDonDay28ofinductionwastheindependentprognostic factorwiththegreatestimpactinmultivariateanalysis,when theEFSwasanalyzedinrelationtotheageandWBCcountat diagnosis.9
Table4–ResultsoftheCoxproportionalhazardsmodel ofprognosticfactorsofacutelymphoblasticleukemiafor asampleof76childrenandadolescentstreatedatthree referralcentersinCeará,Brazil,betweenSeptember 2007andDecember2009.
Variables Coefficient SEM p-value
Age(≥9years) 2.31 2.340 0.019
Riskgroup 1.18 1.004 0.320
InitialWBCcount 6.04 2.644 0.008
CD10(Calla) 2.75 1.767 0.070
WBC>5.0×109cells/L(Day8) 0.76 0.761 0.450 Lymphoblasts>1000cells/L(Day8) 4.01 2.159 0.030 Bonemarrowanalysis(Day28) 0.43 0.372 0.710
SEM:standarderrorofthemean;WBC:whitebloodcellcount.
developedcountries(0.5–1.4%),21,23 suggestingtheinduction mortalityrateisshortofsatisfactoryatBraziliancenters.In thisstudy,infectionwasthemostcommoncauseofdeath.
Atfiveyears,theOSandEFSinthecurrentsamplewere 72% and71.2%, respectively.As expected,the survivalrate was higher for low-risk patients (83%) than for high-risk patients(59%; Figure 1Aand B). Thecorresponding figures were70%±3.6%and69%±2.4%fortheGBTLI-ALL-93protocol and74.2±1.7%and68±1.8%fortheGBTLI-ALL-99protocol, withasignificantdifference infavoroflow-riskpatients.8,9 OurfiguresareslightlybetterthanthoseofLeiteetal.17and Pereira,18butnotasgoodasthefigurescurrentlyreportedby AmericanandEuropeancollaborativechildhoodcancer treat-mentgroups.21,23
TheOSandEFSwerebetterforB-ALLpatients,thoughthe differencewasnotstatisticallysignificant.Thisfindingdiffers fromtheGBTLI-ALL-93protocolinwhichtheEFSatsixyears wassignificantlylowerforT-ALLpatients.8Thisdisagreement mightbeattributedtothe small numberofT-ALLpatients in our study; however, in a study published bythe Dana-Farbergroup,differencesinsurvivalbetweenT-ALLandB-ALL (78%±4%vs.86%±1%)werenotsignificanteither,despitethe findingofincreasedriskofinductionfailureandrelapse.23
Inthe current study,the OS wassignificantly betterfor undernine-year-oldpatientsandpatientswithWBCcountat diagnosis<50.0×109cells/L(Figure1Cand1D),asdocumented inseveralotherstudies.8,9,21,23
Inthemultivariateanalysis(Table4),WBCcountat diag-nosis>50.0×109cells/L,agegreaterthannineyearsandhigh peripherallymphoblastcounts(>1000cells/L)onDay8were
significantlyassociatedwithpoorsurvival.Noother prognos-ticfactors (FAB classification, CD10expressionor DI) were significant.
Overall,theclinicalandlaboratoryfeaturesobservedinthis studyarecompatiblewiththeresultsreportedinthe GBTLI-ALL93and99protocolsandelsewhereintheliterature.The multivariateanalysisindicatedthatage,initialWBCcountand earlyresponsetotreatmentwereindependentprognostic fac-tors,whereasgender,FABclassification,CD10expressionand DIwerenot.
Theestimatedsurvival rates foundwere inferior tothe resultsobtainedindevelopedcountries.The5-yearEFSrate waslowerthanthatreportedintheliterature.However, low-riskpatientshadabetterprognosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
WewouldliketoexpressourthankstoDr.AntônioAldoMelo andDr.aMariaHelenaPitombeirafromtheFederalUniversity ofCearáfortheircriticalreviewofthemanuscript.
r
e
f
e
r
e
n
c
e
s
1.BathiaS,RobinsonL.Epidemiologyofleukemiainchildhood. In:NathanDG,OrkinSH,GinsburgD,LookAT,editors. NathanandOski’sHematologyofInfancyandchildhood.6th ed.Philadelphia:Saunders;2003.p.1081–100.
2.PuiCH,RobisonLL,LookAT.Acutelymphoblasticleukemia. Lancet.2008;371(9617):1030–43.
3.MörickeA,ReiterA,ZimmermannM,HelmutG,MartinS, MichaelD,etal.Risk-adjustedtherapyofacutelymphoblastic leukemiacandecreasetreatmentburdenandimprove survival:treatmentresultsof2169unselectedpediatricand adolescentpatientsenrolledintheTrialALL-BFM95.Blood. 2008;111(9):4477–89.
4.SmithM,ArthurD,CamittaB,CarrollAJ,CristW,GaynonP, etal.Uniformapproachtoriskclassificationandtreatment assignmentforchildrenwithacutelymphoblasticleukemia.J ClinOncol.1996;14(1):18–24.
5.FriedmannAM,WeinsteinHJ.Theroleofprognosticfeatures inthetreatmentofchildhoodacutelymphoblasticleukemia. Oncologist.2000;5(4):321–8.
6.MorickeA,ZimmermannM,ReiterA,GadnerH,OdenwaldE, HarbottJ.Prognosticimpactofageinchildrenand
adolescentswithacutelymphoblasticleukemia:datafrom thetrialsALL-BFM86,90,and95.KlinPadiatr.
2005;217(6):310–20.
7.BorowitzMJ,DevidasM,HungerSP,BowmanWP,CarrollAJ, CarrollWL,etal.Clinicalsignificanceofminimalresidual diseaseinchildhoodacutelymphoblasticleukemiaandits relationshiptootherprognosticfactors:aChildren’s OncologyGroupStudy.Blood.2008;111(12):5477–85. 8.SociedadeBrasileiradeOncologiaPediátrica.Sociedade
BrasileiradeHematologiaeHemoterapia.Campinas: ProtocoloCooperativoGBTLI-LLA-93;1993.
9.SociedadeBrasileiradeOncologiaPediátrica.Protocolode TratamentodaLeucemiaLinfoblásticaAgudana Infância-GBTLI-LLA-1999,Campinas;2000.
10.RCoreTeam.R:Alanguageandenvironmentforstatistical computing.Vienna,Austria:RFoundationforStatistical Computing;2012.Availablefrom:
http://web.mit.edu/rv3.0.1/fullrefman.pdf
11.CoxDR.Regressionmodelsandlifetables.JRStatSocSerB Methodol.1972;34:187–95.
12.PuiCH,KaneJR,CristWM.Biologyandtreatmentofinfant leukemia.Leukemia.1995;9(5):762–9.
13.SchaferES,HungerSP.Optimaltherapyforacute
lymphoblasticleukemiainadolescentsandyoungadults.Nat RevClinOncol.2011;8(7):417–24.
15.PuiCH,PeiD,CampanaD,BowmanPW,SandlundJT,Ribeiro RC,etal.Improvedprognosisforolderadolescentswithacute lymphoblasticleukemia.JClinOncol.2011;29(4):386–91. 16.BarretoLHS[dissertac¸ãomestrado]Estudodesobrevidaem
crianc¸asportadorasdeleucemialinfoblásticaaguda. Salvador:UniversidadeFederaldaBahia;2001.
17.LeiteEP,MunizMT,SoutoFR,BandeiraFM,MeloRM.Fatores prognósticosemcrianc¸aseadolescentescomLeucemia LinfoideAguda.RevBrasSaúdeMaternInfant.
2007;7(4):413–21.
18.PereiraWV[tesedoutorado]Aspectosepidemiológicos, biotipologiaeevoluc¸ãodotratamentodaleucemialinfocítica agudanainfânciaeadolescêncianoRioGrandedoSul.São Paulo:UniversidadedeSãoPaulo;2010.
19.ShusterJJ,WackerP,PullenJ,HumbertJ,LandVJ,MahoneyDH Jr,etal.PrognosticsignificanceofsexinchildhoodB
precursoracutelymphoblasticleukemia:aPediatricOncology GroupStudy.JClinOncol.1998;16(8):2854–63.
20.SchrappeM,CamittaB,PuiCH,EdenT,GaynonP,Gustafsson G,etal.Long-termresultsoflargeprospectivetrialsin childhoodacutelymphoblasticleukemia.Leukemia. 2000;14(12):2193–4.
21.SilvermanLB,GelberRD,DaltonVK,AsselinBL,BarrRD, ClavellLA,etal.Improvedoutcomeforchildrenwithacute lymphoblasticleukemia:resultsofDana-FarberConsortium Protocol91-01.Blood.2001;97(5):1211–8.
22.TeuffelO,StanullaM,CarioG,LudwigWD,ZimmermannM, SchrappeM,etal.Anemiaandsurvivalinchildhoodacute lymphoblasticleukemia.Haematologica.2008;93(11):1652–7. 23.GoldbergJM,SilvermanLB,LevyDE,DaltonVK,GelberRD,
LehmannL,etal.ChildhoodT-cellacutelymphoblastic
leukemia:theDana-FarberCancerInstituteAcute LymphoblasticLeukemiaConsortiumExperience.JClin Oncol.2003;21(19):3616–22.
24.AricóM,ValsecchIMG,RizzariC,BarisoneE,BiondiA, LocatelliF,etal.Long-termresultsoftheAIEOP-ALL-95Trial forChildhoodAcuteLymphoblasticLeukemia:insightonthe prognosticvalueofDNAindexintheframeworkof
Berlin-Frankfurt-Munsterbasedchemotherapy.JClinOncol. 2008;26(2):283–9.
25.DastugueN,SuciuS,PlatG,SpelemanF,CavH,GirardS,etal. Hyperdiploidywith58-66chromosomesinchildhoodB-acute lymphoblasticleukemiaishighlycurable:58951CLG-EORTC results.Blood.2013;121(13):2415–23.
26.BrandaliseSR.Prognosticvalueofday8peripheralblood responseforchildrenwithacutelymphocyticleukemia.In: ZanderAR,editor.Genetechnology:stemcellandleukemia research.Berlin:Spring-Verlag;1996.p.421–8.
27.Coustan-SmithE,SanchoJ,HancockML,RazzoukBI,Ribeiro RC,RiveraGK.Prognosticsignificanceofmeasuringearly clearanceofleukemiccellsbyflowcytometryinchildhood acutelymphoblasticleukemia.Blood.2002;100(1):52–8. 28.ManabeA,OharaA,HasegawaD,KohK,SaitoT,KiyokawaN,
etal.Significanceofthecompleteclearanceofperipheral blastsafter7daysofprednisolonetreatmentinchildrenwith acutelymphoblasticleukemia:TheTokyoChildren’sCancer StudyGroup(TCCSG)StudyL99-15.Haematologica. 2008;93(8):1155–60.
29.VaghelaN,AnandIS,TrivediDH,JaniM.Prognosticvalueof peripheralbloodblastpercentageonday8inlongtermcure inpatientswithALL.WorldJPharmacyPharmSci.