www.jped.com.br
ORIGINAL
ARTICLE
Hyperuricemia
is
associated
with
low
cardiorespiratory
fitness
levels
and
excess
weight
in
schoolchildren
夽
,
夽夽
Luiza
N.
Reis
a,
Jane
D.P.
Renner
b,
Cézane
P.
Reuter
c,d,
Jorge
A.
Horta
b,
Dulciane
N.
Paiva
e,
Andréia
R.
de
M.
Valim
b,
Ana
P.
Sehn
a,
Elza
D.
de
Mello
c,
Miria
S.
Burgos
e,∗aUniversidadedeSantaCruzdoSul(UNISC),SantaCruzdoSul,RS,Brazil
bUniversidadedeSantaCruzdoSul(UNISC),ProgramadePós-graduac¸ãoemPromoc¸ãodaSaúde.DepartamentodeBiologiae
Farmácia,SantaCruzdoSul,RS,Brazil
cUniversidadeFederaldoRioGrandedoSul(UFRGS),ProgramadePós-graduac¸ãoemSaúdedaCrianc¸aedoAdolescente,Porto
Alegre,RS,Brazil
dUniversidadedeSantaCruzdoSul(UNISC),DepartamentodeEducac¸ãoFísicaeSaúde,SantaCruzdoSul,RS,Brazil eUniversidadedeSantaCruzdoSul(UNISC),ProgramadePós-graduac¸ãoemPromoc¸ãodaSaúde,DepartamentodeEducac¸ão
FísicaeSaúde,SantaCruzdoSul,RS,Brazil
Received25August2016;accepted29November2016 Availableonline24April2017
KEYWORDS
Hyperuricemia; Physicalfitness; Overweight; Child; Adolescent
Abstract
Objective: Toevaluatethepossibleassociationbetweenhyperuricemiaandcardiorespiratory
fitnesslevels/nutritionalprofile,groupedintoasinglevariable,inschoolchildren.
Method: Cross-sectionalstudyof2335studentsfromElementaryschools,aged7---17yearsof
both genders, stratified by conglomerates ofa municipality inSouthern Brazil. Body mass index(BMI)wascalculatedandcardiorespiratoryfitness(CRF)wasassessedbythe6-minute run/walktest.TheBMIandCRFweregroupedintoasinglevariable,considering:(1)lowand normalweight/fit;(2)lowandnormalweight/unfit;(3)overweight-obesity/fit;(4) overweight-obesity/unfit. The Poisson regression (prevalence ratio, PR) was used for the association betweenhyperuricemiaandBMI/CRFratiowith95%confidenceintervalsanddifferenceswere consideredsignificantwhenp<0.05.
夽
Pleasecitethisarticleas:ReisLN,RennerJD,ReuterCP,HortaJA,PaivaDN,ValimAR,etal.Hyperuricemiaisassociatedwithlow cardiorespiratoryfitnesslevelsandexcessweightinschoolchildren.JPediatr(RioJ).2017;93:538---43.
夽夽
StudycarriedoutatUniversidadedeSantaCruzdoSul(UNISC),SantaCruzdoSul,RS,Brazil.
∗Correspondingauthor.
E-mail:[email protected](M.S.Burgos). http://dx.doi.org/10.1016/j.jped.2016.11.011
Results: Thereisanassociation,althoughsubtle,betweenthepresenceofhyperuricemiawith lowlevelsofCRFandthepresenceofexcessweight,whengroupedintoasinglevariable.Boys andgirlswiththisconditionhavehigherprevalenceofhyperuricemia(PR:1.07;p=0.007for boys;PR:1.10;p<0.001forgirls).
Conclusion: Together,excessweightandlowlevelsofcardiorespiratoryfitnessareassociated
withthepresenceofhyperuricemiainschoolchildren.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
PALAVRAS-CHAVE
Hiperuricemia; Aptidãofísica; Excessodepeso; Crianc¸a;
Adolescente
Hiperuricemiaestáassociadacombaixosníveisdeaptidãocardiorrespiratória eexcessodepesoemescolares
Resumo
Objetivo: Avaliarapossívelrelac¸ãoentrehiperuricemiacomaptidãocardiorrespiratóriaeo
estadonutricional,agrupados,emescolares.
Método: Estudotransversalcom2335escolaresdaeducac¸ãobásicade7a17anos,deambos
os sexos, estratificadosporconglomerados deum munícipio dosuldo Brasil.Foi calculado o índice de massa corporal (IMC) e a aptidão cardiorrespiratória (APCR) foi avaliada pelo teste decorrida/caminhada de6minutos. OIMC eaAPCRforamagrupados emuma única variável,considerando:1)baixopeso-normal/apto;2)baixopeso-normal/inapto;3) sobrepeso-obesidade/apto;4)sobrepeso-obesidade/inapto.AregressãodePoisson(razãodeprevalência; RP)foiutilizadaparaassociac¸ãoentrehiperuricemiaearelac¸ãoAPCR/IMCcomintervalosde confianc¸ade95%ediferenc¸assignificativasconsideradasparap<0,05.
Resultados: Observa-seassociac¸ão,emborasutil,entreapresenc¸adehiperuricemiacombaixos
níveisdeAPCReapresenc¸adeexcessodepeso,deformaagrupada.Meninosemeninas,com estacondic¸ão,têmmaiorprevalênciadehiperuricemia(RP:1,07;p=0,007;RP:1,10;p<0,001, respectivamente),emcomparac¸ãoaosseusparescombonsníveisdeAPCReestadonutricional adequado.
Conclusão: Deformaconjunta,oexcessodepesoeosbaixosníveisdeaptidão
cardiorrespi-ratóriaestãoassociadoscomapresenc¸adehiperuricemiaemescolares.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Cardiorespiratoryfitness(CRF)isastrongpredictorof mor-talityinadults.ItslevelsinadolescencearerelatedtoCRF in adulthood.1 Additionally, theincidenceof lowlevelsof
CRFinchildrenandadolescentshasincreased.2
Currently, CRF has been associated with the presence ofmetabolicsyndromeinschoolchildren.3Itisknownthat
lowlevelsofCRFinchildhoodarepredictorsof metabolic risk; therefore, maintaining adequate levels of CRF since childhoodis criticaltoreduce theincidence of metabolic syndromeinadulthood.4
LowlevelsofCRFhavebeenassociatedwiththeclassic parametersofmetabolicsyndromeinschoolchildren.5Other
non-traditionalmetabolic risk markers, suchas uric acid, have alsobeen associatedwithlow levelsofCRF, demon-stratingthatchildren andadolescentswithlowCRFlevels havehigherlevelsofthismarker.6
However, the literature is scarce on the association between hyperuricemia, CRF levels, and the presence of overweight/obesityinchildrenandadolescents,especially inBrazil.Theidentificationofanontraditionalmarker,such asuricacid,associatedwithlowlevelsofCRF andexcess
weightin childhood and adolescence, may help pediatri-cians tomake an early diagnosis, aswell as other health professionals,particularlyphysicaleducationandnutrition professionals,tocreateinterventionsaimedat preventing theoccurrenceofmetabolicriskinadulthood.Moreover,the presentstudybringsanewapproach,asitjointlyevaluates thelevelsofCRFandBMIofschoolchildren.Thescarcityof informationandtheimportanceofthesubjectjustifiedthe developmentofthepresentstudy,whichaimedtoevaluate apossibleassociationbetweenhyperuricemiaand cardiore-spiratoryfitnesslevelswithnutritionalstatus,groupedinto asinglevariable,inschoolchildren.
Methods
apopulationof20,380students.Thesedatawereobtained fromtheofficialmunicipalgovernmentagencies.
Thepresentstudyispartofalargerresearchproject enti-tled‘‘Schoolchildren’sHealth---PhaseIII’’,approvedbythe ResearchEthicsCommittee(REC)ofUniversidadedeSanta CruzdoSul(UNISC)underCAAENo.31576714.6.0000.5343, according to Resolution 466/12 of the National Health Council. Allevaluations wereconducted in the University grounds,by professionalsqualified for each function. The schoolchildrenwere enrolledin thestudy only aftertheir parents or guardians signed the informed consent form, andchildrenolderthan12yearsalsoagreedtocollaborate throughatermofassent;thestudyonlyincludedthosewho hadnorestrictionsonbloodcollection.
To calculate sample size, the G*Power 3.1 program (Heinrich-Heine-Universität --- Düsseldorf, Germany) was used, considering Poisson regression as a statistical test (presenceversusabsenceofhyperuricemiaasadependent variable).A test power(1−ˇ)=0.95,significancelevel of
˛=0.05, and an effect size of 0.30, asindicated by Faul etal.,7wereconsidered.Therefore,aminimumsampleof
655studentswasestimatedtocomprisethesample. Intotal,25schoolspublicandprivateschools,bothrural andurban, participatedinthestudy.Theassessedschools wereselectedbydrawinglots,followingthe proportional-ityof theschoolchildren population density,according to thecityregion(Center,North,South,East,andWest)and urban and rural area. Subsequently, the lists of students wereobtainedfromtheselectedschools,andthestudents weredrawnbylotsforthesigningoftheinformedconsent form.
Schoolchildrenenrolledintheselectedschools,ofboth genders,aged between 7and 17 years andwho returned thesignedconsentformandtermofassentwereincluded inthestudy,totaling2502students.Ofthese,167subjects wereexcludedduetotheinabilitytohavebloodcollected andundergotheCRFtest,orduetoremovalofdiscrepant data(outliers)fromthedatabase,afterverificationinthe exploratoryanalysis.
The BMI was calculated through the formula BMI=weight/height2 (kg/m2). To assess weight and
height,thestudentsweremeasured/weighedbarefootand wearing light clothing. The BMI was classified according to the percentile curves by age and gender.8 The values
obtainedwerereclassifiedintotwocategories:low-normal weightandoverweight-obesity. CRF wasevaluatedbythe 6-minute walk/run test. The students were previously advised to wear appropriate footwear and light clothing toundergothe test. The resultswere obtained inmeters coveredbytheschoolchild andclassifiedaccordingtothe tablesoftheBrazilianSportsProject(ProjetoEsporteBrasil [PROESP-BR])for genderand age,asin thehealthy range (goodCRFlevels,fit)orintheriskrange(lowCRF;unfit).9
Thenutritionalstatus/CRFvariablewascategorizedusing theBMIandCRFdata,obtainedseparately.Theresultswere classified into four categories: (1) low-normal weight/fit; (2)low-normal weight/unfit; (3)overweight-obese/fitand (4)overweight-obese/unfit.
Pubertalstagewasclassifiedbasedonpubichairinfive categoriesasTanner stageI(prepubertal),stageII (initial development),stageIII(continuingmaturation1),stageIV (continuingmaturation2),orstageV(matured).10Asurvey
card withfigures it waspresented to the schoolchildren, where the subjects indicated the one that most closely resembledtheirstageofdevelopment.
Blood for uric acid measurement was collected from the brachial vein after a 12-hour fasting; the collection was made at the UNISC Exercise Biochemistry Laboratory by trained professionals (pharmacists and nursing techni-ciansoftheUniversity),followingbiosafetystandards.Uric acidlevelsin theserumofeach patientweredetermined by the photometric enzymatic method, using a conven-tional reagent Kovalent and the Miura 200 automated system (I.S.E., Rome, Italy). Uric acid levels<5.5mg/dL wereconsiderednormal;levels≥5.5mg/dLwereconsidered
hyperuricemia.
The data were analyzed using the statistical program SPSS(IBMCorp.Released2013.IBMSPSSStatisticsfor Win-dows,Version23.0,NY,USA).First,theShapiro---Wilkstest was used to test the normality of the continuous data. Descriptiveanalyseswereexpressedasfrequenciesand per-centages. The chi-squared test was used tocompare the descriptivecharacteristics of the studentsby gender.The associationbetweentheoutcomevariable(hyperuricemia) and the categorized variable nutritional status/CRF was testedusingPoissonregression,usingprevalenceratios(PR) and95%confidenceintervals(CI).Theanalyseswere strati-fiedbygender,beingadjustedfortheagegroupandpubertal stage.Differenceswereconsideredsignificantatp<0.05.
Results
Atotalof2335studentswereevaluated.Regardingthe asso-ciation between the nutritional status and CRF, 21.9% of theboysand27.3%ofthegirlswereclassifiedinthegroup overweight-obesity/unfit(Table1).
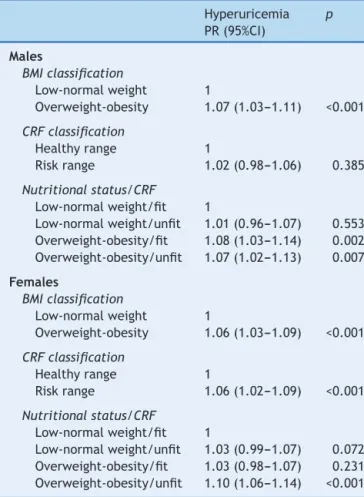
When hyperuricemia was separately associated with nutritionalstatus,itwasobservedthatoverweightorobese male students had a higher prevalence of hyperuricemia whencomparedwasstudentswithlowornormalweight(PR: 1.07, p<0.001). This association was alsoverified among girls,this(PR:1.06,p<0.001).WhenassociatedwithCRF, unfitgirlshadhigherprevalence ofhyperuricemia thanfit girls(PR:1.06,p<0.001;Table2).
Anassociation,albeitsmall,wasobservedbetween hype-ruricemiaandnutritionalstatus/CRFgroupedintoasingle variable,adjustedforageandpubertalstage(Table2).Unfit maleschoolchildrenwithexcessweighthadahigher preva-lenceofhyperuricemiawhencomparedwithfitindividuals withnormalweight(PR:1.07,p=0.007).Similarvalueswere found forboyswithexcessweight,butwhohadgoodCRF (PR: 1.08,p=0.002).Among the assessedgirls,significant differences were found only when comparing overweight andpoorCRFwithnormalweightandgoodCRFlevels(PR: 1.10,p<0.001).
Discussion
Table1 Sampledescription.SantaCruzdoSul,Brazil,2014---2015.
Male (n=1033)
n(%)
Female (n=1302)
n(%)
p
Agerange
Child(6---9years) 289(28.0) 342(26.3) 0.190
Adolescent(10---17years) 744(72.0) 960(73.7)
BMIclassification
Low-normalweight 606(58.7) 795(61.1) 0.129
Overweight-obesity 427(41.3) 507(38.9)
CRFclassification
Healthyrange 600(58.1) 487(37.4) <0.001
Riskrange 433(41.9) 815(62.6)
Nutritionalstatus/CRF
Low-normalweight/Fit 399(38.6) 335(25.7) <0.001
Low-normalweight/Unfit 207(20.0) 460(35.3)
Overweight-obesity/Fit 201(19.5) 152(11.7)
Overweight-obesity/Unfit 226(21.9) 355(27.3)
Pubertalstage
I 262(25.4) 308(23.7) 0.018
II 244(23.6) 326(25.0)
III 189(18.3) 297(22.8)
IV 262(25.4) 272(20.9)
V 76(7.4) 99(7.6)
Uricacid
Normal 844(81.7) 1192(91.6) <0.001
Hyperuricemia 189(18.3) 110(8.4)
Ethnicity
Caucasian 825(75.7) 1051(74.7)
Black 105(9.6) 115(8.2) 0.430
Mixedrace 142(13.0) 215(15.3)
NativeBrazilian 6(0.6) 10(0.7)
Asian 12(1.1) 16(1.1)
Placeofresidence
Urban 806(78.0) 1068(82.0) 0.009
Rural 227(22.0) 234(18.0)
BMI,bodymassindex;CRF,cardiorespiratoryfitness;chi-squaredtest,consideringthecomparisonbetweengenders.
genders who had both overweight/obesity and low levels ofCRF.
Itisnoteworthythat,althoughthisassociationissmall, it is relevant, since the sample comprised children and adolescentsand changesin uric acid levelsaremore fre-quentlyobservedintheadultpopulation.Itisknownthat,in theseindividuals,serumuricacidlevelsareassociatedwith severalcardiometabolicrisk factors,andhyperuricemia is predictiveofobesitydevelopment.11Althoughuricacidhas
an antioxidant function in the extracellular environment, it has detrimental effects when it enters the cells. Its detrimentalimpactincludesendothelialfunctioninhibition, plateletaggregationinduction,andchronicsystemic inflam-mation,amongothers.12,13
Based on the results found, it a higher prevalence of hyperuricemia was observed in schoolchildren of both genders with excess weight, corroborating the current
literature.Leeetal.,14 whenassessing2284childrenaged
6---12 years in 104 schools in 13 cities in Taiwan, found thathyperuricemiaisassociatedwithmetabolicsyndrome, mainly with obesity and abdominal fat. In a study of 2614 school-aged children (4---18 years) in the city of Bogalusa,UnitedStates,Sunetal.13evaluatedthe
associa-tionbetweenuricacidandtheindividualcomponentsofthe metabolicsyndrome;elevatedlevelsofuricacidshoweda strongerassociationwithBMI.
Oneexplanationfortheassociationbetweenbodyfatand hyperuricemiawould betheincrease intheproduction of ketoacids during thenight in individualswith morebody fat,whichwouldcausecompetitionbetweentheacids for renalexcretion,inadditiontoapossiblegenetic predisposi-tiontolowerexcretionofuricacidinsomeethnicgroups.14
Table2 AssociationbetweenhyperuricemiaandCRFwith BMI.
Hyperuricemia PR(95%CI)
p
Males
BMIclassification
Low-normalweight 1
Overweight-obesity 1.07(1.03---1.11) <0.001
CRFclassification
Healthyrange 1
Riskrange 1.02(0.98---1.06) 0.385
Nutritionalstatus/CRF
Low-normalweight/fit 1
Low-normalweight/unfit 1.01(0.96---1.07) 0.553 Overweight-obesity/fit 1.08(1.03---1.14) 0.002 Overweight-obesity/unfit 1.07(1.02---1.13) 0.007
Females
BMIclassification
Low-normalweight 1
Overweight-obesity 1.06(1.03---1.09) <0.001
CRFclassification
Healthyrange 1
Riskrange 1.06(1.02---1.09) <0.001
Nutritionalstatus/CRF
Low-normalweight/fit 1
Low-normalweight/unfit 1.03(0.99---1.07) 0.072 Overweight-obesity/fit 1.03(0.98---1.07) 0.231 Overweight-obesity/unfit 1.10(1.06---1.14) <0.001
PR,prevalenceratio;CI,confidenceinterval;analysisadjusted forageandpubertalstage;BMI,bodymassindex;CRF, cardio-respiratoryfitness.
togetherwiththesynthesisof triglyceridesanddecreased excretionofuricacidasaresultofhyperinsulinemia,which accompaniesobesity.12
Thepresentstudyshowedthatonlygirlswhoareinthe CRF risk zone had a higher prevalence of hyperuricemia. Nosignificant associationswerefoundinthemalegender, whichcorroboratesastudy carriedoutwithindividualsof all agestreated at the Cardiovascular Healthare Program of Universidade Federal de Vic¸osa, Minas Gerais, Brazil, which indicated differences between the genders when uricacidalterationsareassociatedwithbiomarkersof car-diometabolic risk, such as excess weight and sedentary lifestyle.15
These alterations may be associated with the fact that boys and girls differ in several parameters, such as insulin resistance, inflammatory markers, and amino acid catabolismproducts.16Additionally,girlshaveahigher
per-centage of body fat, lower levels of CRF, and are less active,17 whichmayinfluencetheobtainedresults.
When associated with CRF and nutritional status, the prevalence of hyperuricemia is higher in individuals with excess weightcombined withlow levels of CRF. This was observed in both boys and girls. In the male gender, it was observed that students with excess weight and with good levels of CRF also have a higher prevalence of
hyperuricemia. Thus, excess weight appears to carry a higher health risk behavior than adequate levels of CRF. Nonetheless,Barnettetal.,inastudyof1045children(aged 7---12 years)inNewYork, UnitedStates, associated inade-quatelevels of CRFwith obesity,considering both as risk factors for cardiovascular diseases; moreover, CRF classi-fiedintheriskzoneinadolescencewasassociatedwithhigh percentagesofbodyfatinadulthood.18
InSpain,astudyhasshownthatchildrenwithlowlevels ofCRFhavehigherlevelsofuricacid.6Notwithstanding,
lit-tleis knownabout the influenceof physical fitness,since there are few studies associating physical exercise and serumuricacidlevelsinchildrenandadolescents.
Nishidaetal.,12 inNabeshima,Japan,verifiedthe
influ-enceofphysicalactivityintensityandaerobicfitnessonuric acidconcentrationin71obeseadultmen.Moderate phys-ical activity intensity wasassociated withlower levels of uricacid.Villegasetal.19 verifiedtheprevalence andrisk
factorsofhyperuricemiain3978adultmen(40---74years)in Shanghai,China.Physicalactivitywasinverselyassociated with hyperuricemia prevalence, whereas BMI and weight gain were positivelyassociated. Williams,20 in the United
States,analyzedthedistance coveredperweek and coro-nary risk factorsin 8282 malerunners(15---80 years).The datawereobtainedthroughaquestionnaire,whilethe lev-elsofbiochemicaldata,includinguricacid,wereobtained fromdataprovidedbytherunners’physicians.Among the conclusions,itwasobservedthatindividualswhorangreater distanceshadlowerlevelsofuricacid,whichmaybe asso-ciatedwithbetterlevelsofCRF.
Studies with children and adolescents that associated CRFanduricacidlevelsareveryscarce.Thepresentstudy bringsimportantcontributionstotheunderstandingofuric acidbehaviorinrelationtoclinicalandmetabolicvariables. Itisnoteworthytherepresentativenumberofsubjects, chil-drenandadolescents,whosedatawerescarcelyavailableto date.Theauthorsbelieveitisimportanttoaddthe measure-mentofserumuricacidlevelstotheevaluationprotocols inchildrenandadolescents,asitmayallowtheassessment ofpossiblecardiovascularcomplicationsinthebeginningof theirdevelopment.Barnettetal.alsoemphasizethe impor-tance of physical educationclasses at school asa wayto increase the CRF levelsin children and adolescents.This canbeachievedbypromotingnotonlytheirparticipationin physical activityclasses,butalsoinactivitiesthatleadto CRFimprovement,bringingbenefitsbothinchildhoodand adolescence,aswellasinadultlife.18
The present study contributes with knowledge in the area,sincetheassociationofuricacidlevelswithCRFand excess weight in children and adolescents is still poorly established, especiallyin Brazil. The association between elevateduricacidlevelswithCRFandnutritionalstatusmay help healthcareprofessionalsin the diagnosis,treatment, and prevention of metabolic risk conditions in childhood. Additionally, thestudybrings anewapproachbygrouping theCRFandBMIvariablesintoasingleone.Anotherstrength of the study is the fact that it contains a representative sampleofapopulationthatlacksresearch.
thestudents’foodconsumption andthepresenceof arte-rialhypertension,notassessedinthepresentstudy;these variablescouldindirectlyinfluenceserumuricacidlevels. Itis alsoknownthat obesity isa multifactorialcondition, whichcanalsobeinfluencedbyotherinflammatorymarkers. The use of BMI should also be considered, since it is notthebestparametertoevaluateobesity.Althoughuseful instudies witha representativesample, asinthepresent study,itdoes notdifferentiatebetweenleanandfatbody mass. Further studies that can correlate the intensity of exercise with changes in serum uric acid levels are sug-gested,sothatitmaybepossibletoexplorethebeneficial effectsofanactivelifestyleonhyperuricemia.
Hyperuricemiashowedaslightassociationwiththe pres-enceofexcessweightandlowlevelsofCRF,whenassessed together.The measurement of uricacid in childhoodmay beausefulpublichealthcaremeasureforearlyintervention andpreventionoffuturecardiovascularcomplications.
Funding
UniversidadedeSantaCruzdoSul(UNISC).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.DennisonBA,StrausJH,MellitsED,CharneyE.Childhood phys-ical fitness tests: predictorof adultphysical activity levels? Pediatrics.1988;82:324---30.
2.GayaAR,ReuterCP,ReuterÉM,FrankeSI,PráD,GayaAC,etal. Cumulativeincidenceofyouthobesityisassociatedwithlow cardiorespiratoryfitnesslevelsandwithmaternaloverweight. Motriz:RevEducFis.2015;21:407---14.
3.LiaoW,XiaoDM,HuangY,YuHJ,YuanS,ChenT,etal.Combined associationofdietandcardiorespiratoryfitnesswithmetabolic syndrome in Chinese schoolchildren.Matern Child Health J. 2016;20:1904---10.
4.Schmidt MD, Magnussen CG, Rees E, Dwyer T, Venn AJ. Childhoodfitnessreducesthelong-termcardiometabolicrisks associated with childhood obesity. Int J Obes. 2016;40: 1134---40.
5.Machado-Rodrigues AM, Leite N, Coelho-e-Silva MJ, Martins RA,Valente-dos-SantosJ,MascarenhasLP,etal.Independent associationofclusteredmetabolic riskfactorswith cardiore-spiratoryfitness in youth aged 11---17 years. Ann Hum Biol. 2014;41:271---6.
6.Llorente-CantareroFJ,Pérez-NaveroJL,deDiosBenitez-Sillero J,Mu˜noz-VillanuevaMC,Guillén-delCastilloM,Gil-CamposM. Non-traditionalmarkersofmetabolicriskinprepubertal chil-dren withdifferentlevelsofcardiorespiratoryfitness.Public HealthNutr.2012;15:1827---34.
7.Faul F,Erdfelder E, Buchner A, Lang A-G. Statistical power analysesusingG*Power3.1:Testsforcorrelationandregression analyses.BehavResMethods.2009;41:1149---60.
8.WHO. World Health Organization. Growth reference 5---19 years. 2007. [cited 30 Nov 2015]. Available from:
http://www.who.int/growthref/who2007bmiforage/en/ 9.ProjetoEsporteBrasil:manual2015.[cited3Nov2015].
Avail-ablefrom:https://www.proesp.ufrgs.br.
10.TannerJM.Growthatadolescence:withageneralconsideration ofeffectsofhereditaryandenvironmentalfactorsupongrowth andmaturationfrombirthofmaturity.2nded.YnitedKingdom:
BlackwellScientificPublishers;1962.
11.NejatinaminiS,Ataie-JafariA,QorbaniM,NikoohematS, Kel-ishadiR,AsaveshH,etal.Associationbetweenserumuricacid levelandmetabolicsyndromecomponentes.JDiabetesMetab Disord.2015;14:70.
12.NishidaY,Iyadomi M,HigakiY,TanakaH, HaraM,TanakaK. Influenceofphysicalactivity intensityand aerobicfitnesson theanthropometricindexandserumuricacidconcentrationin peoplewithobesity.InternMed.2011;50:2121---8.
13.SunD,LiS,ZhangX,FernandezC,ChenW,SrinivasanSR,etal. Uricacidisassociatedwithmetabolicsyndromeinchildrenand adultsina community:theBogalusaHeart Study. PLoSOne. 2014;9:e89696.
14.Lee MS, Wahlgvist ML, Yu HL, Pan WH. Hyperuricemia and metabolicsyndromeinTaiwanesechildren.AsiaPacJClinNutr. 2007;16:594---600.
15.SilvaHA,CarraroJC,BressanJ,HermsdorffHH.Relac¸ãoentre ácidoúricoesíndromemetabólicaemumapopulac¸ãocomrisco cardiometabólico.Einstein(SãoPaulo).2015;13:202---8. 16.Newbern D, Gumus Balikcioglu P, Balikcioglu M, Bain J,
Muehlbauer M,StevensR, etal. Sexdifferences in biomark-ers associated with insulin resistance in obese adolescents: metabolomicprofilingandprincipalcomponentsanalysis.JClin EndocrinolMetab.2014;99:4730---9.
17.HongHR,HaCD,KongJY,LeeSH,SongMG,KangHS.Rolesof physicalactivityandcardiorespiratoryfitnessonsexdifference ininsulinresistanceinlateelementaryyears.JExercNutrition Biochem.2014;18:361---9.
18.BarnettLM,BeurdenEV,MorganPJ,BrooksLO,BeardJR.Does childhoodmotorskillproficiencypredictadolescentfitness?J SportsMedPhysFitness.2008;40:2137---44.
19.VillegasR,XiangYB,CaiQ,FazioS,LintonM,LiH,etal. Preva-lenceanddeterminantsofhyperuricemiainmiddle-aged,urban Chinesemen.MetabSyndrRelatDisord.2010;8:263---70. 20.WilliamsP.Relationshipofdistancerunperweektocoronary