SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Interaction
of
demographic
factors
with
the
results
of
the
surgery
for
degenerative
disease
of
the
cervical
spine:
a
retrospective
evaluation
夽
Celso
Garreta
Prats
Dias,
Bruno
Braga
Roberto,
Lucas
Basaglia,
Mario
Lenza,
Rodrigo
Junqueira
Nicolau,
Mario
Ferretti
∗HospitalIsraelitaAlbertEinstein,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received30June2016 Accepted15August2016 Availableonline24August2017
Keywords:
Cervicalvertebrae/surgery Qualityoflife
Degenerativediseases Prognosis
Cohortstudy
a
b
s
t
r
a
c
t
Objective:Degenerativediseaseofthecervicalspineisa frequentsourceofintermittent neckpain,wherethepredominantsymptomisaxialneckpain.Theindicationsforsurgical treatmentarereservedforthecaseswheretheconservativetreatmenthasnotrelievedthe symptomsorthepatientpresentsprogressiveneurologicalimpairment.Theobjectiveof thisstudywastoevaluatetheprognosticfactorsinvolvedinpatientssubmittedtosurgical treatmentofthecervicalspine.
Methods:Thestudyanalyzeddatafrompatientssubmittedtocervicalspinesurgerybetween July2011andNovember2015(n=58).Theevaluateddataincludedsmokinghabits, hyperten-sion,diabetes,overweight,surgicaltechnique,andnumberoflevelsoffusion.Theprimary outcomewasdefinedaspainandthesecondaryoutcomeswerequalityoflifeanddisability. Results:Astatisticallysignificantdifferencewasfoundbetweenbaselineandthe12-month post-operativeresultsregardingpaininfavorofnon-hypertensivepatients(p=0.009)and discectomyplusinstrumentation(p=0.004).Therewasalsosignificantdifferencebetween theresultsofneckdisabilityinfavorofnon-hypertensivepatients(p=0.028)andpatients withbodymassindexlowerthan25kg/m2(p=0.005).Therewasnosignificantinteraction betweenanyanalyzeddataandthequalityoflifescoreresults.
Conclusions: Non-hypertensivepatients,thosewithbodymassindexlowerthan25kg/m2, andthosesubmittedtodiscectomycombinedwitharthrodesisofthecervicalspinearethe mostbenefitedbycervicaldegenerativediseasesurgery.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
PaperdevelopedattheHospitalIsraelitaAlbertEinstein,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil. ∗ Correspondingauthor.
E-mails:[email protected],[email protected](M.Ferretti). http://dx.doi.org/10.1016/j.rboe.2017.08.007
Interac¸ão
dos
dados
demográficos
com
os
resultados
da
cirurgia
da
doenc¸a
degenerativa
da
coluna
cervical:
uma
avaliac¸ão
retrospectiva
Palavras-chave:
Vértebrascervicais/cirurgia Qualidadedevida
Doenc¸asdegenerativas Prognóstico
Estudocoorte
r
e
s
u
m
o
Objetivo: Adoenc¸adegenerativadacolunacervicaléumafontefrequentededorcervical intermitente,naqualossintomaspredominantessãodoraxialcervical.Asindicac¸õespara cirurgiasãoreservadasparaoscasosdefalhadotratamentoconservadoroucomsintomas neurológicosprogressivos.Oobjetivodesteestudofoiavaliarosfatoresprognósticosdos pacientessubmetidosaotratamentocirúrgicodacolunacervical.
Métodos: Oestudoavaliouospacientessubmetidosàcirurgiadacolunacervicalentrejulho de2011enovembrode2015(n=58).Asvariáveisdecomparac¸ãoavaliadasforamtabagismo, hipertensão,diabete,sobrepeso,técnicacirúrgicaaplicadaenúmerodeníveisdeartrodese. Odesfechoprimáriofoidefinidocomodoreosdesfechossecundáriosforamqualidadede vidaedisfunc¸ão.
Resultados: Encontramosdiferenc¸aestatisticamentesignificativaentreosescoresdedor de baseeaos12mesesapósa cirurgia,favorável aospacientessemhipertensão arte-rialsistêmica(p=0,009)eaossubmetidosàdiscectomiacominstrumentac¸ão(p=0,004). Tambémhouvediferenc¸aestatisticamentesignificativanaavaliac¸ãodadisfunc¸ãoda col-unacervical:oresultadofoimaisfavorávelparaospacientessemdiagnósticopréviode hipertensão(p=0,028)eparaospacientescomIMCmenordoque25kg/m2(p=0,005).Não seobservouevidênciadeinterac¸ãosignificativaentreosdadosavaliadoseosresultadosdo questionáriodequalidadedevida.
Conclusões: Ospacientesnãohipertensos,comíndicedemassacorpóreamenordoque 25kg/cm2esubmetidosàartrodesecombinadaàdiscectomia,sãoosmaisbeneficiados comoprocedimentocirúrgicodadoenc¸adegenerativadacolunacervical.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Thedegenerativechangesofthespineareanatomical adjust-mentstothecontinuousstressofcompressionanddistraction on the spinestructures.1–3 During this adaptation process, sometissuechangesareremarkable,suchascalcificationof ligamentsandformationofosteophytes.Inthecervicalspine, osteophytesformedintheendplatesandjointfaces repre-senttheboneelementsthatcausecompression,whereasdisc protrusion, yellow ligament or hypertrophic joint capsules mayaggravate or initiatethe compressionbysoft tissues.3 Theprevalenceofpatientswithadegenerativediscdisease isuncertain,asinanasymptomaticpopulationthepresence ofradiographicsignsofdegenerationofthecervicalspinecan reach80%.4–6Whensymptomsarepresent,itsprogressionto moreseverecasesishighlyvariableandpoorlydefined.7
Degenerativediseases ofthecervical spineare frequent causes of intermittent cervical pain in adult and elderly patients,withthepredominantsymptombeingaxial cervi-calpain,whichoriginatesfromthedegenerationofthediscs, vertebralplateaus,facetjointsorthegrowthofosteophytes.1–3 Frequently,thereisanassociationwithneurological symp-toms. Magnetic resonance imaging is indicated for these patients.2,8Mostcasesofdegenerativecervicalspinedisease, orcervicalradiculopathyrespondtoconservativetreatment, which consists of postural advice, changes in daily life activities,cervical immobilizations, isometricexercisesand
medication.1,2,8Indicationsforsurgicaltreatmentarereserved forcasesinwhichpainhasnotbeensolvedwith conserva-tivetreatment,orwhenthereisprogressionofneurological deficits.1,2,8,9
Depending on the disease presented by the patient, two principlesare soughtafterthrough surgicaltreatment: decompressionandfusion(alsoknownasarthrodesis).1,2,7,10 Decompressionisindicated incasesinwhich degenerative changescausedirectneuralcompression.Thefusion,onthe otherhand,isindicatedincasesthatpresentinstabilityorloss ofmechanicalintegrityofthecervicalspine.Thisprocedure mayalsohavebeneficialeffectsoncompressivesymptoms, throughappropriatedistractionappliedinthesegment, espe-ciallyincaseswherethereisforaminalstenosis.1,10
lifescales,presenceofneurologicalsymptoms,andeven psy-chosocialfactors.12,13 Anderson et al.12 concludedthat the factorsofgreaterclinicalrelevanceforpoorresultswerethe useofpreoperativeweakanalgesics, andthe helpofsome typeoffinancialassistancebythepatientduetoincapacity causedbythecervicaldisease.Thesamestudyshowedthat thefactorsrelatedtogoodresultswereadvancedage,high preoperativeNDIandoccupationinprofitablejobs.13
Theobjectiveofthisstudywastoevaluatetheprognostic factorsofpatientssubmittedtocervicalspinesurgical treat-ment.
Material
and
methods
Studydesignandsetting
Thisisacross-sectional studythat evaluatedthe database betweenJuly2011andNovember 2015ofpatients undergo-ingsurgeryforthetreatmentofcervicalspinedegenerative diseasesinaprivatequaternaryhospitalinSãoPaulo,Brazil. Duringthisperiod,90surgerieswereperformedtotreat cer-vicalspinedegenerativedisease.Thestudywassenttoand accepted by the Ethics and Research Committee (number 49217515.6.0000.0071).
Inclusionandexclusioncriteria
Inclusioncriteria:(1)adultsof18yearsorabove,with indi-cation for surgery of the cervical spine for stenosis, with or without myelopathy or cervical hernia;(2) submitted to surgical treatment; (3) with no contraindication to general anesthesia;(4)withanunderstandingofthePortuguese lan-guage and after accepting a written consent form so to completethequestionnaires.
Exclusioncriteria:patientswith(1)spinefractures;(2) sco-liosis;(3)congenitaldeformitiesofthespine;(4)spinetumors; (5)spinalinfection;(6)previoussurgeryonthecervicalspine; (7)inabilitytoparticipateinthefollow-up(duetoinabilityto readorcompletetherequiredforms).
Patients’demographicdata
Thefollowing data were collected based on each patient’s medicalrecord,
- Age(inyears).
- Gender(femaleormale).
- Weight,heightandBMI(inkg,mandkg/m2,respectively). - Previousadjuvant therapies (physiotherapy,acupuncture,
hydrotherapyorGPR).
- Previousdiagnosisofhypertension. - Previousdiagnosisofdiabetes. - Previousdiagnosisoffibromyalgia. - Smokingorsmokinghabits.
- Alcoholismorhabitofdrinkingalcoholicbeverages. - Surgical techniqueapplied(simple discectomyor
discec-tomywithfusion).
Thedatausedforanalysisandcomparisonoftheresults weresmoking,hypertension,diabetes,overweight(IMC>25), clustering(surgicaltechniqueapplied)andnumberoflevels offusion.
The sample analyzed consisted of 58 patients submit-ted to surgery for the treatment of degenerative diseases ofthespine.Datafrom the32other patients’recordswere insufficientforstatisticalanalysisorwerenotfound.Oneof the patientsdidnotrespondtothe EVAandNDI question-naires, sothese twovariables hadatotal Nof57 patients. Surgeries occurred between July 2011and November 2015. Thebodymassindex(BMI)rangedfrom20.7 to42.0kg/m2, withanaverageof27.3kg/m2(SD=4.60kg/m2).Mostpatients (89.7%)underwentcervicalfusionsurgery.Theseoperations, involving anterior fusion, used at least one plaque, four screws and one cage, two screws and a cage were added for each additional level of fusion. The remaining proce-dures(10.3%)weresimpleposteriordiscectomy,withoutthe needforimplants.Asforcomorbiditiesandsocialdata,41.4% werehypertensive,12.1%werediabetics,13.8%weresmokers, therewerenocasesofalcoholismorpatientswith fibromyal-gia.
Evaluatedoutcomes
The primary outcome was pain, assessed by visual ana-log scale (VAS)rangingfromzero to10(zero,pain absence and 10 maximum pain).14,15 Secondary outcomes were: (1) aqualityoflifescalewasassessed,measuredbythe ques-tionnaire EQ-5D16 validated for the Portuguese language17; (2) theNeck DisabilityIndex18 validated forthePortuguese language.19
Thevisualanalogscaleusedwasthenumericalone,which rangesfromzeroto10,zerobeingtheabsenceofpain,and10 themostseverepain.Thus,1–3wasconsideredmildpain,4–6, moderatepain,and7–10,severepain.15
The EQ-5D used was the EQ-5D-3L, which consists of two columns, one ofwhich describes the five dimensions evaluated: (1) mobility; (2) self-care;(3) usual activities; (4) pain/discomfort;(5)anxiety/depression.Thesecondpresents theanalogscale,consistingofthreelevelsforeachdimension, rangingfrom“noproblemtoperform”to“disability”, associ-atedwithagradeof1–3,respectively.16Thefinalresultisa sequenceof5digits,withfiguresfrom1to3,whichshould beanalyzedtogetherwithatablethatshowstherespective scoreresults,whichcanvaryfrom−0.594to+1(unitvalue),to
thepointthattheresultslowerthanorequaltozeroindicate significantdisability.
(completedisability).18,19Intheeventthattherearequestions leftblank,theresultobtainedisdividedbythetotalnumber ofquestions answeredand thenthisvalueismultipliedby 100.19
Thescores obtainedduring the postoperative follow-up visitswerecomparedwiththepre-operativescores,andthe variationsofatleast2.6pointsfortheEVAscore,0.24points fortheEQ-5Dand17.3%forNDIwereconsidered clinically significant,assuggestedbyParkeretal.11
Alloftheaforementionedoutcomeswereevaluated pre-operativelyandthenat1,2,3,6and12monthsoffollow-up, depending on the attendance and commitment of each patient,whichisalsodescribedandanalyzed.
Statisticalanalysis
Qualitative variables were described by absolute frequen-ciesand percentages,andthe numericalonesbysummary measures such as average, standard deviation, median, interquartilerange,minimumandmaximumvalues.20
Theinfluenceofinterestfactorsinthevariationofthescore scales throughoutthe follow-up wasevaluated by general-izedestimationequationmodels,consideringthecorrelation betweenthemeasurementsofthesamepatientinthe differ-entmomentsofevaluation(preoperativeandwith1,3,6and 12monthsoffollow-up).
ThemodelsfortheEVAandNDIscaleswereadjustedwith negativebinomialdistribution,and fortheEQ-5Dscalethe normaldistributionwasused.Multiplecomparisonswere cor-rectedbytheBonferronimethod.
Theresultsofthe modelswere presentedintablesand graphsbyadjustedaveragevaluesandconfidenceintervals of95%.
TheseanalyzeswereperformedwiththehelpoftheSPSS software(SPSSInc.Released2008.SPSSStatisticsforWindows, Version17.0,Chicago:SPSSInc.)andalevelofsignificanceof 5%wasconsidered.21,22
Results
A model of generalized estimation equations (GEE) was adjusted,considering the evaluationsofVAS,NDI and EQ-5Dthroughoutthefollow-upandthedifferentdemographic statesofthepatients.
Mainoutcome–painvisualanalogicalscore(VAS)
Therewasastatisticallysignificantdifferencebetweenthepre andpostoperativescoresat3,6and12monthsinthe assess-ment ofthe presenceor absence ofSAH,whichwas more favorableforpatientswithoutpreviousdiagnosisof hyperten-sion(p=0.009),asdescribedinTable1.
Inaddition,theaverageVASfornon-hypertensivepatients (4.4points)comparedtotheaveragepreoperativevalues(7.3 points)werealsoclinicallysignificant,accordingtothestudy byParkeretal.,11 whichconsideredtheminimumvariation of2.6points intheVAS.Onthe otherhand,the hyperten-sivepatientsvariedinaverageonly1.1pointsbetweenthe
Table1–Estimateaveragesandconfidenceintervalof 95%forVASscalescoresinpre-andpost-evaluations accordingtothediagnosisofhypertension.
Evaluation Hypertension
No(n=33) Yes(n=24)
Pre 7.3[6.4;8.1] 6.1[4.8;7.3] 1month 2.7[1.5;4.0] 4.8[3.5;6.2] 3months 2.3[1.2;3.5] 4.4[3.3;5.4] 6months 4.8[3.6;5.9] 3.5[2.1;4.9] 12months 4.4[3.0;5.8] 5.0[3.7;6.3] Effectofinteraction 0.009
preoperativeandthe12-monthpostoperativeevaluation,from 6.1to5points.
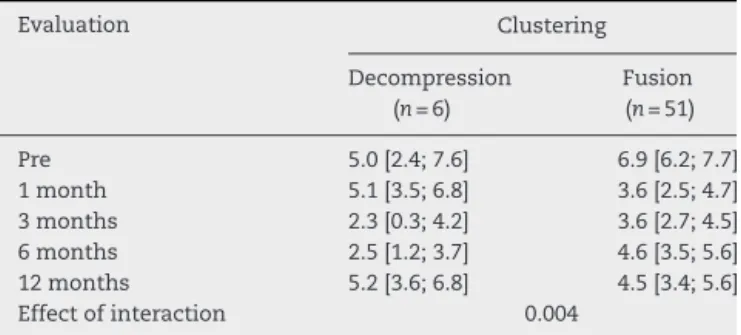
Therewasastatisticallysignificantdifferencebetweenthe pre and postoperativescoresat3, 6and 12months inthe comparison between the procedures of simplediscectomy and discectomy with instrumentation, it was more favor-able for patients who underwent discectomy in addition to instrumented fusion (p=0.004), as described in Table 2. Thisevaluation,however,wasnotclinicallysignificant,when comparingpreandpostoperativeaverages,accordingtothe minimumvariationconsidered.
No evidence of significant interaction was observed between the following data and the evaluations of EVA throughout the follow-up, that is, there was no evidence thatthevariationinEVAscoresdependsonsmokinghabits (p=0.569), diagnosis ofdiabetes(p=0.076),overweight with BMIhigherthan 25kg/m2 (p=0.381),ornumber oflevelsof fusion(p=0.151).
Secondaryoutcome–dysfunctionNeckDisabilityIndex (NDI)
TherewasastatisticallysignificantdifferenceforNDIbetween pre and postoperativescoresat3, 6and 12months inthe assessment ofthe presenceor absence of hypertension, it wasmorefavorableforpatientswithoutprevious diagnosis ofhypertension(p=0.028),asdescribedinTable3.
There was also a statistically significant difference for NDI betweenthe preand postoperativescores at3, 6 and 12 months in the evaluation of the presence or not of
Table2–Estimateaverageandconfidenceintervalof 95%forVASscalescoresinpre-andpost-evaluations accordingtothetypeofsurgery.
Evaluation Clustering
Decompression (n=6)
Fusion (n=51)
Table3–Estimateaverageandconfidenceintervalof 95%forVASscalescoresinpre-andpost-evaluations accordingtothediagnosisofhypertension.
Evaluation Hypertension
No(n=33) Yes(n=24)
Pre 21.2[17.7;24.7] 21.7[18.0;25.5] 1month 15.6[12.1;19.1] 15.3[10.4;20.2] 3months 11.5[8.0;14.9] 17.2[12.9;21.6] 6months 14.6[10.8;18.5] 13.0[9.0;17.1] 12months 11.2[6.7;15.8] 15.5[11.5;19.5] Effectofinteraction 0.028
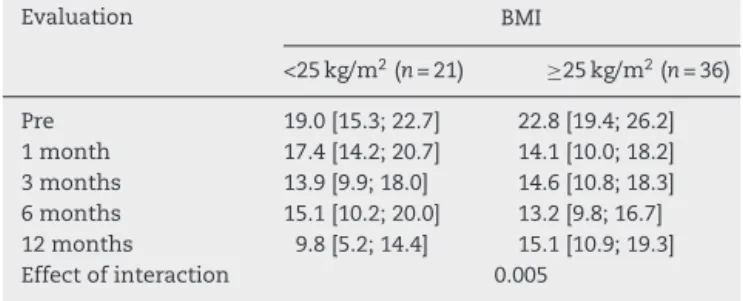
Table4–Estimateaverageandconfidenceintervalof 95%forNDIscalescoresinpre-andpost-operative evaluationsaccordingtothelevelofBMI.
Evaluation BMI
<25kg/m2(n=21) ≥25kg/m2(n=36)
Pre 19.0[15.3;22.7] 22.8[19.4;26.2] 1month 17.4[14.2;20.7] 14.1[10.0;18.2] 3months 13.9[9.9;18.0] 14.6[10.8;18.3] 6months 15.1[10.2;20.0] 13.2[9.8;16.7] 12months 9.8[5.2;14.4] 15.1[10.9;19.3] Effectofinteraction 0.005
overweight;itwasmorefavorableforpatientswithBMIlower than25kg/m2(p=0.005),asdescribedinTable4.
Theoutcomesdescribedabovedidnotreachclinically sig-nificantNDIvariationaccordingtothestudybyParkeretal.,11 whichshouldbeatleast17.3%.
Therewasnoevidenceofsignificantinteractionbetween the following data and NDI assessments during follow-up, i.e., there is no evidence that variation in NDI scores dependsonsmokinghabits(p=0.791),diagnosisofdiabetes (p=0.918),clustering(p=0.374),ornumberoflevelsoffusion (p=0.388).
Secondaryoutcome–EuroQol(EQ-5D)questionnaire regardingqualityoflife
There was no evidence of significant interaction between thedataassessedandtheresultsoftheEuroQolqualityof life questionnaire throughout the follow-up, that is, there was no evidence that the variation in the EuroQol scores dependson the smoking habit (p=0.115), diagnosis of dia-betes(p=0.721),orSAH(p=0.423),overweightwithBMIover 25kg/m2(p=0.444),clustering(p=0.087),ornumberoflevels offusion(p=0.884).
Discussion
Ingeneral,surgeryfordegenerativecervicalspinediseaseby discectomywithor withoutanteriorfusion, apartfromthe evaluationstratifiedbydemographicdata,showedshort-and long-termimprovementinourevaluation.Ontheotherhand, whenthepatientswerestratifiedintosubgroups,differences
betweentheoutcomeswerefound,butagreater understand-ingofthecomplexphysiopathologyofthedegenerativedisc disease is still necessary to find the real causes for these events.
Inarecentstudy,Murrayetal.comparedthesurgical out-comesofpatientswithdegenerative cervicalspine,and no differencesamongtheresultsofthestatisticalanalysiswere foundintheresultsforpainorqualityoflifeamongthe dif-ferentdemographicaspects:gender,age,ethnicity,smoking, BMI,surgicallevelorprevioustreatment,whichcontrastwith someresultsofthepresentstudy.23
The combined analysis of our results with the current literature suggests that surgery for degenerative cervical spinedisease hasgood resultsinshortand longtermsbut presents statistically significant differences among demo-graphicgroups,whichmayguidethechoiceofthepatientwho willhavegoodresultsandpossiblyavoidorpostpone unneces-sarysurgery,andpatientswhowillhavelesssignificantresults inthelatepostoperativeperiod.
Ourstudyconcludedthatallpatientsarebenefitedtosome degreewithsurgeryfordegenerative cervicalspinedisease, butthosewhoareoverweight,whoundergosimple decom-pressionor whohaveaprevious diagnosisofhypertension are the ones who have the least improvement in pain or qualityoflife.Otheroperativetechniquesunderdevelopment may further improve this paradigm, but new longitudinal and prospectiveclinicalstudiesare stillnecessarytobetter evaluatetheoutcomes and possiblecomplications. Current studies show little statistical difference in the outcome of painordysfunctionwhencomparedtodiscectomyprocedures with fusion, and discectomy witharthroplasty, inorder to maintainsegmentmobility.23–25Newformsofoutcome eval-uationand questionnairesarealsounderdevelopmentand validationtoreach increasinglyaccurate conclusionsabout subjectiveandindividualdataratherthanashallow compar-isonofradiographicresultsthatmaynotfaithfullyexpress patientsatisfaction.26
Study
limitations
Aweakpointoftheretrospectivestudiesthatshouldbetaken intoaccountisthefactthatpatientsarenotrandomlyselected foreachtypeoftreatment,andthatthereisalsonopossibility ofblinding,whichresultsinnon-homogeneousgroups.The studysamplewasrelativelysmall;inaddition,manypatients didnotrespondtoallquestionnairesontheirreturn.Another selectionbiasisrevealedatthelevelofhealthcareinwhich theAlbertEinsteinIsraeliteHospitalis,attendingmostly pri-vateorhealthplanpatients,whichlimitsthediversification ofcases.Somedecisivefactorsthatledtotheconductofthe procedureweredisregardedbythemethod,suchaspresence ofinstabilityorpreoperativefacetarthritis,whichwouldneed tobeevaluated,forexample,fromimagingtestsandusually indicateanteriorcervicalfusion.
Virtues
of
the
study
filledoutbythenursingteam,allowsustomakeadequately safeconclusionstowriteahistoricalcohortstudysuchasthe presentone.Theresultsmayhelppredict betterlong-term resultsfromdemographicdata,whichshouldbeassociated withthesurgeon’sexperience.
Conclusion
In the sample studied, smoking habits, previous diagnosis ofdiabetes,or thenumber oflevels offusion donot influ-encetheprognosisofcervicalspinesurgery,intermsofpain, qualityoflifeanddysfunction.Ontheotherhand,patients with hypertension were less favored in relation to pain and dysfunction. In addition, overweight patients, defined asBMIgreater than 25kg/m2, didnotachieve asignificant improvementindysfunctionasthose withBMIlower than 25kg/cm2. Patientswhounderwent discectomywithfusion hadbetterpainscoresafter12 monthsthan those submit-tedtosimplediscectomyalone.Therefore,non-hypertensive patientswithaBMIlowerthan 25kg/cm2 andsubmittedto combinedfusionwithdiscectomyseemtobemorefavored withthe surgicalprocedure fordegenerative cervical spine disease.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
To the team of the Center for the Researcher Support (NAP)ofourinstitutionforthedatastatisticalanalysisand attention.
r
e
f
e
r
e
n
c
e
s
1. GrobD.Surgeryinthedegenerativecervicalspine.Spine (PhilaPa1976).1998;23(24):2674–83.
2. TakagiI,EliyasJK,StadlanN.Cervicalspondylosis:anupdate onpathophysiology,clinicalmanifestation,andmanagement strategies.DisMon.2011;57(10):583–91.
3. TeraguchiM,YoshimuraN,HashizumeH,MurakiS,Yamada H,MinamideA,etal.Prevalenceanddistributionof intervertebraldiscdegenerationovertheentirespineina population-basedcohort:theWakayamaSpineStudy. OsteoarthritisCartilage.2014;22(1):104–10.
4. BodenSD,McCowinPR,DavisDO,DinaTS,MarkAS,WieselS. Abnormalmagnetic-resonancescansofthecervicalspinein asymptomaticsubjects:aprospectiveinvestigation.JBone JointSurgAm.1990;72(8):1178–84.
5. ErnstCW,StadnikTW,PeetersE,BreucqC,OsteauxMJC. PrevalenceofannulartearsanddischerniationsonMR imagesofthecervicalspineinsymptomfreevolunteers.EurJ Radiol.2005;55(3):409–14.
6. NakashimaH,YukawaY,SudaK,YamagataM,UetaT,KatoF. Abnormalfindingsonmagneticresonanceimagesofthe cervicalspinesin1211asymptomaticsubjects.Spine(Phila Pa1976).2015;40(6):392–8.
7.TetreaultL,GoldsteinCL,ArnoldP,HarropJ,HilibrandA, NouriA,etal.Degenerativecervicalmyelopathy:aspectrum ofrelateddisordersaffectingtheagingspine.Neurosurgery. 2015;77Suppl.4:S51–67.
8.McCormackBM,WeinsteinPR.Cervicalspondylosis.An update.WestJMed.1996;165(1–2):43–51.
9.HuppertJ,BeaurainsJ,SteibJP,BernardP,DufourT,HovorkaI. Comparisonbetweensingle-andmulti-levelpatients: clinicalandradiologicaloutcomes2yearsaftercervicaldisc replacement.EurSpineJ.2011;20(9):
1417–26.
10.vanLimbeekJ,JacobsWC,AndersonPG,PavlovPW.A systematicliteraturereviewtoidentifythebestmethodfora singlelevelanteriorcervicalinterbodyfusion.EurSpineJ. 2000;9(2):129–36.
11.ParkerSL,GodilSS,ShauDN,MendenhallSK,McGirtMJ. Assessmentoftheminimumclinicallyimportantdifference inpain,disability,andqualityoflifeafteranteriorcervical discectomyandfusion:clinicalarticle.JNeurosurgSpine. 2013;18(2):154–60.
12.AndersonPA,SubachBR,RiewKD.Predictorsofoutcome afteranteriorcervicaldiscectomyandfusion:amultivariate analysis.Spine(PhilaPa1976).2009;34(2):161–6.
13.SokolowskiMJ,JacksonAP,HaakMH,MeyerPRJr,Szewczyk SokolowskiM.Acuteoutcomesofcervicalspineinjuriesin theelderly:atlantaxialvssubaxialinjuries.JSpinalCordMed. 2007;30(3):238–42.
14.GrotleM,BroxJI,VøllestadNK.Concurrentcomparisonof responsivenessinpainandfunctionalstatusmeasurements usedforpatientswithlowbackpain.Spine(PhilaPa1976). 2004;29(21):E492–501.
15.HuskissonEC.Measurementofpain.JRheumatol. 1982;9(5):768–9.
16.EuroQolGroup.EuroQol–anewfacilityforthemeasurement ofhealth-relatedqualityoflife.HealthPolicy.
1990;16(3):199–208.
17.FerreiraPL,FerreiraLN,PereiraLN.Contributosparaa validac¸ãodaversãoportuguesadoEQ-5D.ActaMedPort. 2013;26(1):664–75.
18.VernonH,MiorS.Theneckdisabilityindex:astudyof reliabilityandvalidity.JManipulativePhysiolTher. 1991;14(7):409–15.
19.CookC,RichardsonJK,BragaL,MenezesA,SolerX,KumeP, etal.Cross-culturaladaptationandvalidationoftheBrazilian PortugueseversionoftheNeckDisabilityIndexandNeckPain andDisabilityScale.Spine(PhilaPa1976).2006;31(14): 1621–7.
20.AltmanDG.Practicalstatisticsformedicalresearch.London: CRCPress;1990.
21.PaulaGA.Modelosderegressãocomapoiocomputacional. SãoPaulo:InstitutodeMatemáticaeEstatísticada UniversidadedeSãoPaulo;2013.
22.PinheiroJC,BatesDM.Mixed-effectsmodelsinSandS-PLUS. Statisticsandcomputingseries.NewYork,NY:
Springer-Verlag;2000.
23.MurreyD,JanssenM,DelamarterR,GoldsteinJ,ZiglerJ,TayB, etal.Resultsoftheprospective,randomized,controlled multicenterFoodandDrugAdministrationinvestigational deviceexemptionstudyoftheProDisc-Ctotaldisc replacementversusanteriordiscectomyandfusionforthe treatmentof1-levelsymptomaticcervicaldiscdisease.Spine J.2009;9(4):275–86.
24.MaldonadoCV,PazRD,MartinCB.Adjacent-level
degenerationaftercervicaldiscarthroplastyversusfusion. EurSpineJ.2011;20Suppl.3:403–7.
randomized,controlled,multicenterIDEclinicaltrial.Spine (PhilaPa1976).2015;40(11):759–66.
26.AmentJD,YangZ,ChenY,GreenRS,KimKD.Anovel quality-of-lifeutilityindexinpatientswithmultilevel