Mar-Apr 2010; 18(2):287-94 www.eerp.usp.br/rlae
Corresponding Author: Cristina Maria Galvão
Universidade de São Paulo. Escola de Enfermagem de Ribeirão Preto Av. Bandeirantes, 3900
Monte Alegre
CEP:14040-902 Ribeirão Preto, SP, Brasil E-mail: [email protected]
Surgical Positioning: Evidence for Nursing Care
1Camila Mendonça de Moraes Lopes
2Cristina Maria Galvão
3The goal of surgical positioning is to promote access to the surgical site. It should be carried
out correctly to ensure patient safety and prevent complications. This integrative literature
review aimed to search for and evaluate available evidences in literature about nursing care
related to surgical positioning of adult patients in the intraoperative period. Pubmed, Cinahl
and Lilacs databases were used for the selection of the articles. The sample consisted of 20
articles. The synthesis of the available evidence showed that included studies focused on
three main topics: risk factors for developing complications, complications due to surgical
positioning and nursing care related to surgical positioning. Among the gaps in the research
theme, the need to conduct studies on effective devices for each type of surgical position
is highlighted.
Descriptors: Perioperative Nursing; Nursing Care; Research.
1 Paper extracted from Master’s Thesis “Posicionamento Cirúrgico: evidências para o cuidado de enfermagem”, presented to Escola de
Enfermagem de Ribeirão Preto, Universidade de São Paulo, SP, Brazil.
Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, WHO Collaborating Centre for Nursing Research Development, SP, Brazil:
2 RN, M.Sc. in Nursing. E-mail: [email protected].
Posicionamento cirúrgico: evidências para o cuidado de enfermagem
O posicionamento cirúrgico tem como principal inalidade promover o acesso ao sítio
cirúrgico e deve ser realizado de forma correta para garantir a segurança do paciente
e prevenir complicações. O presente estudo teve como objetivo buscar e avaliar as
evidências disponíveis na literatura sobre os cuidados de enfermagem, relacionados ao posicionamento cirúrgico do paciente adulto no período intraoperatório. O método
de pesquisa adotado foi a revisão integrativa da literatura. Para a seleção dos artigos,
utilizaram-se as bases de dados PubMed, Cinahl e Lilacs. A amostra constitui-se de 20
artigos. Na síntese das evidências constatou-se que os artigos incluídos enfocaram três tópicos principais, a saber: os fatores de risco para o desenvolvimento de complicações;
as complicações decorrentes do posicionamento cirúrgico e os cuidados de enfermagem
relacionados ao posicionamento cirúrgico. Dentre as lacunas do tema investigado,
destaca-se a necessidade de condução de estudos sobre dispositivos eicazes para cada
tipo de posição cirúrgica.
Descritores: Enfermagem Perioperatória; Cuidados de Enfermagem; Pesquisa.
Posicionamiento quirúrgico: evidencias para el cuidado de enfermería
El posicionamiento quirúrgico tiene como principal inalidad promover el acceso al sitio
quirúrgico y debe ser realizado de forma correcta para garantizar la seguridad del paciente
y prevenir complicaciones. El presente estudio tuvo como objetivo buscar y evaluar las
evidencias disponibles en la literatura sobre los cuidados de enfermería, relacionados al posicionamiento quirúrgico del paciente adulto en el período intraoperatorio. El método de investigación adoptado fue la revisión integradora de la literatura. Para la selección de los artículos, se utilizaron las bases de datos PubMed, Cinahl y Lilacs. La muestra se constituyó de 20 artículos. En la síntesis de las evidencias se constató que los artículos incluidos enfocaron tres tópicos principales, que son: los factores de riesgo para el
desarrollo de complicaciones, las complicaciones provenientes del posicionamiento
quirúrgico y los cuidados de enfermería relacionados al posicionamiento quirúrgico. Entre los vacíos del tema investigado, se destaca la necesidad de conducir estudios sobre dispositivos eicaces para cada tipo de posición quirúrgica.
Descriptores: Enfermería Perioperatoria; Atención de Enfermería; Investigación.
Introduction
Intraoperative nurses are responsible for planning
and putting in practice nursing interventions that
minimize or make it possible to prevent complications
deriving from the anesthetic-surgical procedure, with a
view to the patient’s safety, comfort and individuality(1).
The patient’s surgical positioning is an important
procedure in intraoperative nursing care. The main goal
of this procedure is to promote optimal exposure of the
surgical site and, at the same time, prevent complications
deriving from surgical positioning. Therefore, teamwork
and the use of speciic positioning devices and equipment
for each patient are essential. Nurses share the decision
on how to best position the patient to facilitate activities
during anesthesia and surgery with the team (surgeon,
anesthetist and nursing staff). For this purpose, the
patient’s anatomic and physiological alterations need
to be identiied, associated with the type of anesthesia,
procedure type and surgical time he/she will be
submitted to, so that the positioning is adequate and
does not cause postoperative complications(2).
This research is motivated by the lack of Brazilian
the importance of research to support decision making by
perioperative nurses, who have limited access to literature
due to a lack of time and dificulties to seek and analyze
available evidence and apply it in clinical practice.
The theoretical framework adopted to develop this
research was Evidence-Based Practice (EBP). The EBP
approach integrates the best evidence from research
with professionals’ clinical competency and patients and
family members’ preferences in decision making in
high-quality health care(3).
The practice of EBP in nursing encourages nurses to
do research directed at clinical practice needs and/or the
use of research results available in literature(4).
Purpose
This research aimed to search for and assess
evidence available in literature about nursing care
related to surgical positioning of adult patients in the
intraoperative period.
Methodological procedure
The adopted research method was an integrative
literature review. This method includes systemized
analysis and synthesis of research results on the same
theme, contributes to deepen the research theme,
supports decision making and, consequently, the
improvement of clinical practice, based on preexisting
research results(5-6).
The following steps were followed to elaborate this
integrative review: identiication of theme or formulation
of guiding question; sampling or literature search for
studies; assessment of studies included in the review;
discussion and interpretation of results and synthesis of
knowledge evidenced in analyzed articles or presentation
of integrative review results(5,7).
The guiding question to elaborate the integrative
review was: what is the nursing care related to surgical
positioning of adult patients in the intra-operative
period?
For the article search, the internet was used
to access the following databases: PubMed (digital
biomedical and health science iles from the US
National Institutes of Health), CINAHL (Cumulative
Index to Nursing and Allied Health Literature) and
LILACS (Latin American and Caribbean Health Science
Literature).
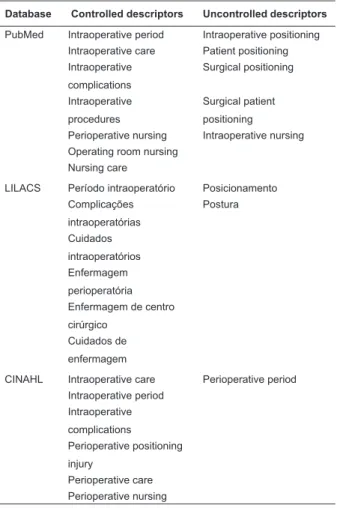
Keywords related to the theme were selected
and it was checked in the databases whether these
were controlled descriptors according to each speciic
database indexation. Table 1 displays the descriptors
used to conduct the integrative review.
Database Controlled descriptors Uncontrolled descriptors
PubMed Intraoperative period Intraoperative positioning Intraoperative care Patient positioning Intraoperative
complications
Surgical positioning
Intraoperative procedures
Surgical patient positioning
Perioperative nursing Intraoperative nursing Operating room nursing
Nursing care
LILACS Período intraoperatório Posicionamento Complicações
intraoperatórias
Postura
Cuidados intraoperatórios Enfermagem perioperatória Enfermagem de centro cirúrgico
Cuidados de enfermagem
CINAHL Intraoperative care Perioperative period Intraoperative period
Intraoperative complications
Perioperative positioning injury
Perioperative care Perioperative nursing
Table 1 – Controlled and uncontrolled descriptors
according to selected databases
With a view to a broad article search, all possible
combinations among the descriptors were searched in
each database. The following inclusion criteria were
adopted: article on nursing care to adult patients in
surgical positioning in the intraoperative period; published
in English, Spanish and Portuguese between July 1998
and July 2008 and articles without distinguishing the
adopted research design.
The articles were selected by their title and
abstract, in line with the study goal and in compliance
with the inclusion criteria. Six hundred references were
preselected in PubMed, 140 in LILACS and 754 in CINAHL,
totaling 1494 articles, which resulted in a sample of 20
articles that were analyzed in full. To extract the data,
a previously published and validated data collection
instrument was used(8). To analyze the evidence level
Rev. Latino-Am. Enfermagem 2010 Mar-Apr; 18(2): 287-94.
review, the concepts proposed by nursing researchers
were used(3,9).
The articles were analyzed and summarized
descriptively, allowing readers to assess the quality
of evidence (evidence level) available in literature on
the research theme, support decision making in daily
intraoperative nursing and identifying knowledge gaps
with a view to future research.
Results
Twenty articles were included in the review,
nineteen of which were published in English and one in
Portuguese; among the publications’ countries of origin,
the United States predominated with thirteen articles.
Papers were published in a range of journals, particularly
the AORN Journal (four articles).
With regard to the evidence level, only one study
showed a strong evidence level (level II) with an
experimental design, i.e. controlled randomized clinical
trials; one study was considered of moderate evidence
level (level III) with a quasi-experimental design, i.e.
assessments (process analysis), and eight studies
presented weak evidence (levels VI and VII), three
with a non-experimental design, two descriptive,
cross-sectional studies and three experience reports. In the
same sense, the other ten studies (narrative literature
reviews) are not classiied according to the adopted
hierarchical system. Tables 2, 3, 4 and 5 show the
synthesis of the analyzed articles.
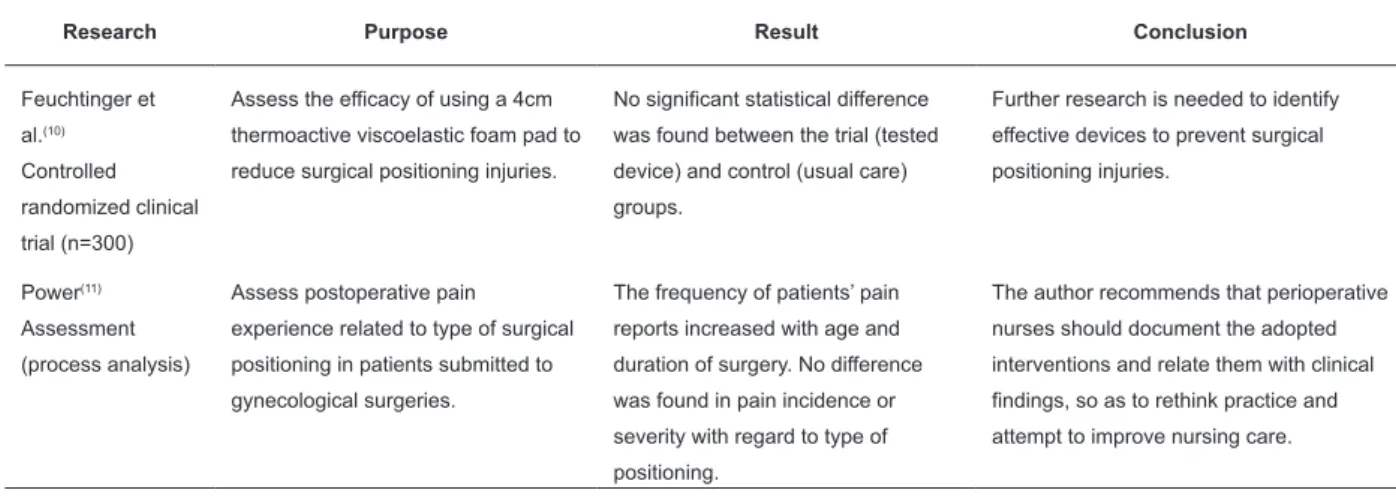
Table 2 – Synthesis of research with experimental and quasi-experimental research design
Research Purpose Result Conclusion
Feuchtinger et al.(10) Controlled randomized clinical trial (n=300)
Assess the efficacy of using a 4cm thermoactive viscoelastic foam pad to reduce surgical positioning injuries.
No significant statistical difference was found between the trial (tested device) and control (usual care) groups.
Further research is needed to identify effective devices to prevent surgical positioning injuries.
Power(11) Assessment (process analysis)
Assess postoperative pain experience related to type of surgical positioning in patients submitted to gynecological surgeries.
The frequency of patients’ pain reports increased with age and duration of surgery. No difference was found in pain incidence or severity with regard to type of positioning.
The author recommends that perioperative nurses should document the adopted interventions and relate them with clinical findings, so as to rethink practice and attempt to improve nursing care.
Table 3 – Synthesis of research with non-experimental research design
Research Purpose Result Conclusion
Roeder et al.(12) Descriptive cross-sectional research
Assess capillary pressure supported in the heel and calf region in individuals in lithotomy position.
Pressure increases with increased height of calf support in variation of lithotomy position and the larger the support surface, the lower the capillary pressure supported.
The authors recommend the use of the lowest heel position; placement of support under the greatest contact area and maintaining the patient in the lithotomy position for the shortest possible time.
Matos, Piccoli(13) Descriptive cross-sectional research
Verify the frequency of the risk for perioperative positioning injury nursing diagnosis, defining characteristics and related factors.
The diagnosis was identified in 100% of the sample. The defining characteristics and identified factors were loss of habitual protective barrier after anesthesia and commitment of tissue perfusion after cold in surgery room with frequencies of more than 50%.
Nurses should plan actions based on each patient’s specific characteristics, the patient’s surgical positioning is what determines a safe and efficient procedure.
Stevens et al.(14) Retrospective correlation research
Analyze the injuries of patients submitted to urological surgical procedures, correlated with predisposing factors.
Surgical positioning and prolonged surgery time were significantly associated with the development of skin injuries. The risk of developing injuries is greater in patients placed in the lateral position, which is chosen in urological surgeries.
Table 4 – Synthesis of expert opinion and experience report research
Research Purpose Synthesis
AORN(15) Expert opinion
Offer perioperative nurses best-practice guidelines for patient positioning.
The Association constructed practical recommendations in six standards, which are: I. Preoperative assessment of patient’s special surgical positioning needs, II. Devices to support positioning should be available, clean and preferably maintain normal capillary interface pressure, III. The nurse should monitor the patient’s body alignment and tissue integrity based on physiological principles, IV. After the positioning, the nurse should assess the patient again, V. Positioning documentation should follow “AORN Recommended practices for documentation of perioperative nursing care”, VI. Institutional standards and procedures for deciding on patient positioning should be reviewed and updated every year and should be followed by all participants in this activity.
Richardson(16) Expert opinion
Describe the use of a type of leg holder and its benefits during surgical patient positioning.
The author describes the use of a new type of leg holder to place the patient in the lithotomic position, which is called “Direct Placement Leg Holders” (DPLHs). This device is easy to move, fix and position, besides reducing heel and calf pressure. It facilitates routine and promotes patient safety. Nurses are responsible for providing the best equipment and guaranteeing its correct use so as to provide better patient care.
Carris, Franczek(17) Experience report
Describe a surgical positioning device for patients submitted to endoscopic urological procedures.
The authors describe difficulties to place obese patients in the lithotomic position after induced anesthesia. They report on the use of a 91.44x60.96cm smooth plastic device that is cheap and normally used for snow sliding, covered by a surgical drape and placed under the patient. Soon after anesthetic induction, this device helps to slide the patient to the lower part of the table, a simple procedure that facilitated patient positioning, avoiding injuries in the patient and team, and which can be used at any other surgical center.
Murphy(18) Experience report
Report on three cases with legal decisions involving intraoperative injuries deriving from surgical positioning.
In the three cases of surgical positioning injuries, no negligence by the perioperative nursing team was evidenced. It serves as an alert to nurses though, so as to take care while transporting, transferring and positioning the patient on the surgery table, using due protection and padding, highlighting the importance of documentation so as to provide legal support for the delivered care.
Schulman et al.(19) Experience report
Describe an intraoperative positioning technique for burned patients.
The technique is used to permit free access to structures that need to be debrided in burned patients. Correct positioning favors a shorter surgery time and, consequently, decreases the number of interventions and reduces the risk of complications.
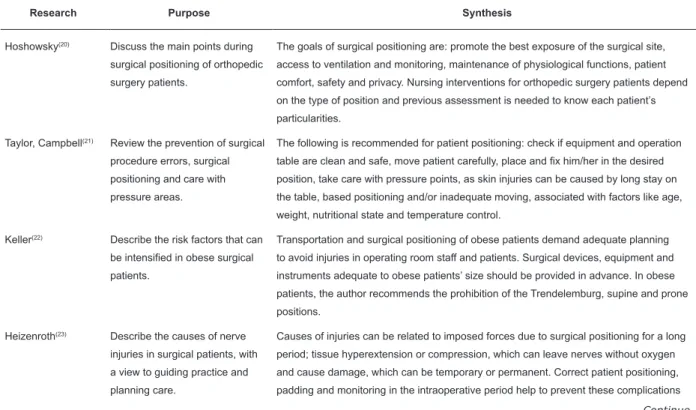
Table 5 – Synthesis of narrative literature review research
Research Purpose Synthesis
Hoshowsky(20) Discuss the main points during surgical positioning of orthopedic surgery patients.
The goals of surgical positioning are: promote the best exposure of the surgical site, access to ventilation and monitoring, maintenance of physiological functions, patient comfort, safety and privacy. Nursing interventions for orthopedic surgery patients depend on the type of position and previous assessment is needed to know each patient’s particularities.
Taylor, Campbell(21) Review the prevention of surgical procedure errors, surgical positioning and care with pressure areas.
The following is recommended for patient positioning: check if equipment and operation table are clean and safe, move patient carefully, place and fix him/her in the desired position, take care with pressure points, as skin injuries can be caused by long stay on the table, based positioning and/or inadequate moving, associated with factors like age, weight, nutritional state and temperature control.
Keller(22) Describe the risk factors that can be intensified in obese surgical patients.
Transportation and surgical positioning of obese patients demand adequate planning to avoid injuries in operating room staff and patients. Surgical devices, equipment and instruments adequate to obese patients’ size should be provided in advance. In obese patients, the author recommends the prohibition of the Trendelemburg, supine and prone positions.
Heizenroth(23) Describe the causes of nerve injuries in surgical patients, with a view to guiding practice and planning care.
Causes of injuries can be related to imposed forces due to surgical positioning for a long period; tissue hyperextension or compression, which can leave nerves without oxygen and cause damage, which can be temporary or permanent. Correct patient positioning, padding and monitoring in the intraoperative period help to prevent these complications
Rev. Latino-Am. Enfermagem 2010 Mar-Apr; 18(2): 287-94.
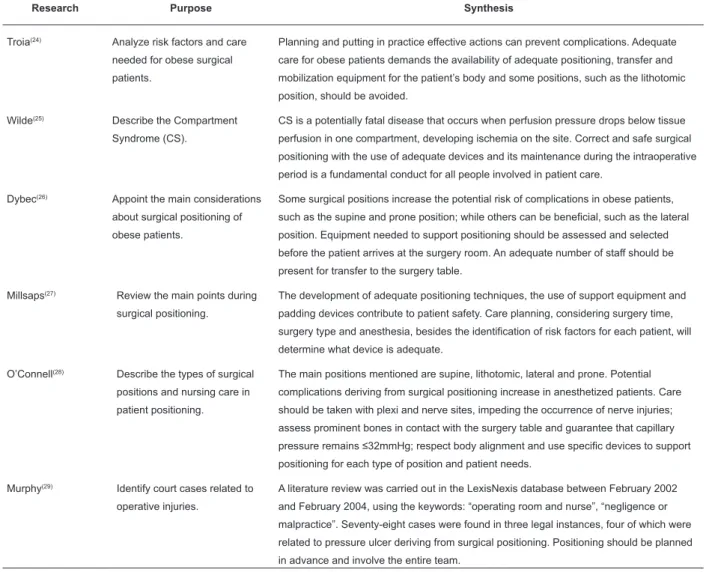
Table 5 – Continuation
Research Purpose Synthesis
Troia(24) Analyze risk factors and care needed for obese surgical patients.
Planning and putting in practice effective actions can prevent complications. Adequate care for obese patients demands the availability of adequate positioning, transfer and mobilization equipment for the patient’s body and some positions, such as the lithotomic position, should be avoided.
Wilde(25) Describe the Compartment Syndrome (CS).
CS is a potentially fatal disease that occurs when perfusion pressure drops below tissue perfusion in one compartment, developing ischemia on the site. Correct and safe surgical positioning with the use of adequate devices and its maintenance during the intraoperative period is a fundamental conduct for all people involved in patient care.
Dybec(26) Appoint the main considerations about surgical positioning of obese patients.
Some surgical positions increase the potential risk of complications in obese patients, such as the supine and prone position; while others can be beneficial, such as the lateral position. Equipment needed to support positioning should be assessed and selected before the patient arrives at the surgery room. An adequate number of staff should be present for transfer to the surgery table.
Millsaps(27) Review the main points during surgical positioning.
The development of adequate positioning techniques, the use of support equipment and padding devices contribute to patient safety. Care planning, considering surgery time, surgery type and anesthesia, besides the identification of risk factors for each patient, will determine what device is adequate.
O’Connell(28) Describe the types of surgical positions and nursing care in patient positioning.
The main positions mentioned are supine, lithotomic, lateral and prone. Potential complications deriving from surgical positioning increase in anesthetized patients. Care should be taken with plexi and nerve sites, impeding the occurrence of nerve injuries; assess prominent bones in contact with the surgery table and guarantee that capillary pressure remains ≤32mmHg; respect body alignment and use specific devices to support positioning for each type of position and patient needs.
Murphy(29) Identify court cases related to operative injuries.
A literature review was carried out in the LexisNexis database between February 2002 and February 2004, using the keywords: “operating room and nurse”, “negligence or malpractice”. Seventy-eight cases were found in three legal instances, four of which were related to pressure ulcer deriving from surgical positioning. Positioning should be planned in advance and involve the entire team.
Discussion
The synthesis of research data from the review
studies revealed that these focused on three main
themes, which were: risk factors for the development
of complications, complications deriving from surgical
positioning and nursing care related to the patient’s
surgical positioning.
Preoperative assessment of each surgery patient’s
risk factors and their consideration in the elaboration
of the care plan can contribute so as not to develop
complications in the intraoperative period(20-28). All
identiied risk factors should be documented, as well as
orientations patients received(29).
The main risk factors mentioned were:
general anesthesia – situation in which the body loses physiological protection for compensation mechanisms
and is susceptible to muscle and/or nerve injuries
and pain. Using drugs like muscle relaxants and pain
medication can mask and delay the diagnosis of
intraoperative injuries(20-28);
age – elderly or very young patients can have a more sensitive skin and greater probability to develop skin
injuries(20-21, 25, 27- 28) ;
weight – assess the body mass index, as obesity and overweight can lead to a higher potential of complications
due to positioning and low weight causes increased
exposure of the patient’s bone prominences, which
are regions more susceptible to the appearance of skin
injuries(20-22, 24-28);
immobility or mobilization problems – make surgical
positioning more dificult and can favor the formation of
blood clots and pressure points(20, 23--25, 27-28);
body temperature control problems – as a result of hypothermia, body structures depend on more oxygen
and, without the necessary inlow, this can favor the
preexisting health conditions - diabetes mellitus,
cancer, kidney failure, low preoperative hematocrit and
hemoglobulin levels, vascular, heart and respiratory
diseases and conditions affecting the immune system
can favor the development of complications(20-22, 24-28);
prolonged surgery time - surgeries longer than two hours can affect the oxygenation of compressed tissues
and favor the occurrence of pressure ulcers(20-28) .
All studies assessed(10-29) appointed that the
patient’s surgical positioning causes some negative
impact on body systems and can entail several
complications, such as: musculoskeletal pain, joint
dislocation, peripheral nerve damage, skin injuries,
cardiovascular and pulmonary problems and even
compartment syndrome.
The following stand out among nursing care
recommendations in the analyzed articles: respect body
alignment; take actions for pressure areas; reduce
friction, shear and pressure; check bone prominences;
select and make available positioning devices according
to each patient’s needs and relate them with the surgery
type and time; move, transport and position the patient
with an adequate number of staff and using adequate
equipment to avoid occupational and patient injuries;
document all positioning procedures(10,20-22,24,26-28).
The main surgical position recommendations are:
supine – use pillows or supports for the head and below the knees, place arms at a maximum angle of 90º
with the body, keep legs uncrossed, pay attention with
hyperextension of the feet;
prone – protect face, eyes and chin, favor access to tubes and monitoring lines, maintain neck alignment,
place roll cushion from the collar bone to the iliac crest
and under the legs and feet, leave genitals free, protect
feet against hyperlexion;
lateral – maintain spinal alignment, observe ears, place a support under the head, armpit region and between
the legs, keep leg in contact with the table lexed in the
hip region and the superior leg stretched;
lithotomy – maintain arms in arm holders at a maximum angle of 90º, pad hip, buttocks and body sides, use the lowest leg elevation for the shortest possible time and
minimize the hip abduction degree.
Conclusion
The conclusion of this integrative literature review evidences the importance of nursing actions in surgical
positioning, including the prevention of complications
deriving from this procedure, the assessment of each patient’s needs and the availability of adequate equipment
and devices. Nurses should become consumers of
research results and/or conduct studies in response to
daily problems, and should also seek strategies to put available evidence in clinical practice. In the authors’
opinion, this will imply the consolidation of
Evidence-Based Practice.
References
1. Galvão CM. A prática baseada em evidências: uma contribuição para amelhoria da assistência de enfermagem perioperatória. [livre-docência]. Ribeirão Preto (SP): Escola de Enfermagem de Ribeirão Preto da Universidade de São Paulo; 2002. 114 p. 2. St-Arnaud D, Paquin M. Safe positioning for neurosurgical patients. AORN J. 2008; 87(6):1156-72.
3. Melnyk BM, Fineout-Overholt E. Making the case for evidence-based practice. In: Melnyk BM, Fineout-Overholt E. Evidence-based practice in nursing & healthcare: a guide to best practice. Philadelphia: Lippincott Williams & Wilkins; 2005. p. 3-24. 4. Galvão CM, Sawada NO, Rossi LA. A prática baseada em evidências: considerações teóricas para sua implementação na enfermagem perioperatória. Rev Latino-am Enfermagem 2002; 10(5):690-5.
5. Mendes KDS, Silveira RCCP, Galvão CM. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto Contexto Enferm. 2008; 17(4): 758-64. 6. Mendes KDS, Galvão CM. Liver transplantation: evidence for nursing care. Rev Latino-am Enfermagem 2008; 16(5):915-22. 7. Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs. 2005; 52(5):546-53.
8. Ursi ES, Galvão CM. Prevenção de lesões de pele no período
perioperatório: revisão integrativa da literatura. Rev Latino-am Enfermagem 2006; 14(1):124-31.
9. Polit DF, Beck CT, Hungler BP. Fundamentos de pesquisa em enfermagem: métodos, avaliação e utilização. Porto Alegre (RS): ArtMed; 2004. 487 p.
10. Feuchtinge J, Bie R, Dassen T, Halfens R. A 4-cm thermoactive viscoelastic foam pad on the operating table to prevent pressure ulcer during cardiac surgery. J Clin Nurs. 2006; 15(2): 162-7. 11. Power H. Patient positioning outcomes for women undergoing gynaecological surgeries. Can Oper Room Nurs J. 2002; 20(3):7-10, 27-30.
12. Roeder RA, Geddes LA, Corson N, Pell C, Otlewsk M, Kemeny A. Heel and calf capillary-support pressure in lithotomy positions. AORN J. 2005; 81(4):821-5.
13. Matos FGOA, Piccoli M. Diagnóstico de enfermagem risco para lesão perioperatória por posicionamento identificado no período transoperatório. Ciência, Cuidado e Saúde 2004; 3(2): 195-201.
14. Stevens J, Nichelson E, Linehan M, Thompson N, Liewehr D, Venzon, et al. Risk factors for skin breakdown after renal and adrenal surgery. Urology 2004; 64 (2):246-9.
Rev. Latino-Am. Enfermagem 2010 Mar-Apr; 18(2):287-94.
practices for positioning the patient in the perioperative practice setting. AORN J. 2001; 73(1):231-8.
16. Richardson C. Use of leg positioning holders. Br J Perioper Nurs. 2004; 14(3):127-30.
17. Carris J, Franczek T. Patient positioning: snow fun in the OR. Today Surg Nurse 1999; 21(3):47-8.
18. Murphy EK. Negligence cases concerning positioning injuries. AORN J. 2004; 80(2):311-4.
19. Schulman CI, Namias BJ, Rosales O, Pizano LR, Ward CG, Namias N. A portable, universal patient positioning and holding system for use in the burn patient ‘The Burnwalter’. Burns 2005; 31(5):647-9.
20. Hoshowsky VM. Surgical positioning. Orthop Nurs. 1998; 17(5):55-65.
21. Taylor M, Campbell C. Patient care in the operating department (1). Br J Theatre Nurs.1999; 9(6):272-5.
22. Keller C. The obese patient as a surgical risk. Semin Perioper Nurs.1999; 8(3):109-17.
23. Heizenroth P. Surgery: it’s got some nerve! Hosp Nurs. 2001; 31(10):32hn1-4.
24. Troia C. Promoting positive outcomes in obese patients. Plast Surg Nurs. 2002; 22(1):10-7, 28.
25. Wilde S. Compartment syndrome. The silent danger related to patient positioning and surgery. Br J Perioper Nurs. 2004; 14(12):546-50, 552-4.
26. Dybec RB. Intraoperative positioning and care of the obese patient. Plast Surg Nurs. 2004; 24(3):118-22.
27. Millsaps CC. Pay attention to patient positioning! RN 2006; 69(1):59-63.
28. O’Connell MP. Position impact on the patient positioning. Nurs Clin North Am. 2006; 4(12):173-92.
29. Murphy EK. Protecting patients from potential injuries. AORN J. 2004; 79(5):1013-6.
Received: May. 6th 2009